
Abstract
Background:
Little is known about the experience of treatment burden, or the difficulties that arise when the treatment workload overwhelms one's ability to take on treatment activities, at the end of life.
Objective:
We first assessed rates of treatment burden experienced by all older adults in the last three years of life. Among the subset of our sample who had multiple chronic conditions (MCCs), we determined correlates of treatment burden with sociodemographic, health, and caregiving factors.
Design:
We conducted a cross-sectional study using nationally representative data from the National Health and Aging Trends Study (NHATS).
Setting/Subjects:
Our sample included 356 adults, aged 65 years and older, who died within three years of completing the 2012 NHATS Treatment Burden Questionnaire. Our MCC cohort included only those in our sample with two or more chronic conditions.
Measurements:
Our measure of treatment burden included reports of difficulty in managing treatment activities, delays in treatments, or feeling that physicians asked for too much. We built a composite measure to identify burden if participants reported that at least one item occurred sometimes or often.
Results:
Forty-three percent of older adults in their last three years of life experienced treatment burden. Among individuals with MCCs, bivariate analysis found that treatment burden was associated with being a racial minority and having depression, anxiety, and a cancer diagnosis. These associations were not statistically significant in a multivariable model.
Conclusion:
Treatment burden is a common experience among older adults regardless of sociodemographic, clinical, and caregiving factors.
Introduction
With almost half of the U.S. population living with at least one chronic illness, 1 patients are increasingly required to take on the management of their own health care activities, such as adhering to complex treatment programs and navigating difficult health care systems. 2 Treatment burden arises when the demands of self-managing one's treatment activities exceed an individual's capacity to take it on. As such, the concept of treatment burden includes both objective and subjective components. Objectively, workload demands that can contribute to feelings of burden include self-management responsibilities such as medication adherence, administrative tasks, and managing finances.3,4 However, treatment burden is a subjective experience; patient resources, care network, and physical and emotional capacity to manage health care can mitigate the burden of workload responsibilities.5–7 Attempting to alleviate burdensome workloads of overwhelmed patients is a necessary component to person-centered care.8,9
Treatment burden has emerged as an important consideration for older adults, who often must learn to live with multiple chronic illnesses.10–12 Older adults, especially those with multiple chronic conditions (MCCs), can be subjected to polypharmacy and may struggle with completing health care tasks.13,14 As physical and cognitive abilities decline, older adults become increasingly reliant on caregivers, who may themselves struggle to provide adequate assistance.15–17 In short, the imbalance between workload and capacity that leads to burden becomes especially consequential in older adults with limited means to manage complicated medical needs.
Despite its relevance to the clinical care of older adults with chronic conditions, the experience of treatment burden at the end of life is not well understood. Care at the end of life can become complicated and can increase strain on patients and their caregivers. 18 Several studies on end-of-life decision making have consistently found burden to be a consideration in deciding treatment courses.19–22 Furthermore, studies have acknowledged the benefits of decreasing treatment burden in the context of specific terminal illnesses, such as end-stage renal disease or cancer,20–24 but it is unclear how treatment burden presents across the overall population of older adults.
To better understand how treatment burden presents at the end of life, we examined nationally representative data from the National Health and Aging Trends Study (NHATS) to assess treatment burden through a general measure that broadly inquires about the presence of burdensome treatment activities in disease self-management. We first determined the prevalence of treatment burden over the last three years of life among older adults in the United States. While the end-of-life period has been defined as ranging from weeks to years before death,25,26 we included the last three years of life in our analysis to gain a more comprehensive picture of how the prevalence of treatment burden might change over time. To focus on those with significant disease burden at the end of life, we then limited further analysis to older adults with MCCs in their last three years of life and measured the association of sociodemographic, health, treatment workload, capacity, and care context factors with treatment burden. We hypothesized that treatment burden will increase in cohorts closer to their time of death.
Methods
Data source and study sample
This study draws on survey data collected by NHATS, a longitudinal population-based survey of health and disability among a representative sample of individuals aged 65 years and older living in the contiguous United States.27,28 Respondents were eligible for this study if they completed the Treatment Burden Questionnaire (TBQ) in the 2012 NHATS Engagement in Health Care Module (n = 2253) and died within three years of doing so (n = 356). We excluded respondents with three or more missing responses to the four burden items (n = 8).
To ensure that we captured those in the last three years of life with a high burden of treatment difficulties, our bivariate and multivariate analyses were limited to individuals with MCCs (n = 238). We defined MCCs as the presence of two or more of the following self-reported conditions: heart attack, heart disease, arthritis, diabetes, lung disease, dementia, and cancer. This definition was informed by previous studies of MCCs in older adults.29.30
Main measure
The primary outcome of interest was treatment burden. Survey respondents were asked to reflect on the work they do to manage their health and rate how often they experienced the following four aspects of burden: (1) difficulty in self-management of health care activities; (2) difficulty experienced by close friends and family in managing the respondent's health; (3) medical tasks getting delayed or not done; and (4) feeling that health care providers asked the respondent to do too much. Participants rated difficulties associated with each of four burden items as occurring “never,” “rarely,” “sometimes,” or “often.” We dichotomized the presence of burden for each item as experiencing it sometimes or often, as others have done. 9
However, given that some respondents managed their own health, while others received assistance from close friends and family, as indicated in the first two items of the measure, we considered responses for these items together, such that a positive response would be reporting difficulty with either self-management of health care activities or management by close friends and family. In this way, the treatment burden measure could be used to assess difficulty with treatment management regardless of the ability to self-manage care. Therefore, our final measure of treatment burden identified participants who indicated that they sometimes or often experienced difficulty among themselves or their family, delays in completing medical tasks, or felt that their doctors ask them to do too much.
Other measures
Several studies have conceptualized treatment burden to be determined by the patient's workload in addition to their capacity to take on that workload.3,4,7 These models have also acknowledged that one's capacity and workload are buffered by socioeconomic circumstances and the ability to engage one's care network. 7 We therefore considered measures within the following five categories: sociodemographic factors, health characteristics, workload, individual capacity, and care context.
Sociodemographic factors and health characteristics
Demographic characteristics included age, sex, race, education, and average yearly income in dollars. For our multivariate analysis, subgroups in race were dichotomized into a white category, including non-Hispanic whites and other, and a minority category, including non-Hispanic blacks and Hispanics. Health characteristics included self-reported quality of health and hospital stays within the last year. Mean number of medical conditions was a count of the following: heart attack, stroke, cancer, heart disease, hypertension, arthritis, osteoporosis, diabetes, lung disease, hip fracture, dementia, depression, and anxiety.
Individual capacity
Presence of dementia was determined by NHATS classification of probable dementia. 31 Depression and anxiety were categorized as scores of ≥3 according to established cut points of the PHQ-2 and GAD-2 measures, respectively.32,33 Impairments with activities of daily living were defined as receiving help with eating, getting cleaned, using the toilet, dressing, indoor walking, or getting out of bed. Changes in health were measured by determining differences in self-reported health from 2011 to 2012. Changes in mobility were determined by respondents indicating that they leave their homes more often, less often, or the same as they did in the previous year.
Workload
Participants reported whether they took prescription medication in the past month. Receiving help with medications was defined as reporting that others were involved in medication management in the last month. Receiving help with doctor appointments was defined as indicating that others accompanied them to appointments in the last year.
Care context
Participants' care contexts included marital status, living arrangements, and the presence of paid helpers. Helpers included those who helped with personal care, mobility, household, or medical activities. Respondents were categorized by decision-making preferences with doctors and loved ones, as done previously. 9 Respondents also reported who they managed health care with. Hospice use was measured both as a dichotomized yes/no and a count of days in hospice.
Time to death
Months to death were calculated by determining the number of months between when participants completed the survey and their reported death, as determined by NHATS interviewers. For our descriptive analysis, we divided our sample into six-month cohorts based on their time to death. For our multivariable analysis, we grouped our sample into three cohorts of yearlong intervals.
Statistical methods
We measured the prevalence of total treatment burden as well as each of the three separate burden items for each six-month cohort. Then, limiting the sample to those with MCCs, we compared differences in sociodemographic and health characteristics, workload, capacity, and care contexts using bivariate analysis. To identify predictors of burden, we ran two multivariable logistic regression models: the first (minimally adjusted model) included sociodemographic factors (age, race, and sex) and years to death, and the second model (fully adjusted model) added variables that showed a statistically significant effect on treatment burden in the bivariate model. Therefore, our final fully adjusted model included demographics (age, race, and sex), health variables (depression, anxiety, and cancer diagnosis), and years to death. A p-value of <0.05 was considered statistically significant. We used STATA, version 15.1, to conduct all analyses.
The Johns Hopkins University Institutional Review Board (IRB) approved the NHATS protocol, and all participants provided written informed consent. The Icahn School of Medicine at Mount Sinai's IRB approved the study.
Results
Aim 1: Prevalence of treatment burden in the last three years of life
Among older adults, in their last three years of life, 43.3% report treatment burden (Table 1). Specifically, 35% found it difficult for themselves or their families to manage medical tasks, 21% experienced delays in completion of medical tasks, and almost 12% felt that their health care providers ask them to do too much. When we divided our sample into cohorts based on the time between their interview and their death, we found that rates of treatment burden remained relatively constant regardless of how close individuals were to their time of death (Fig. 1).
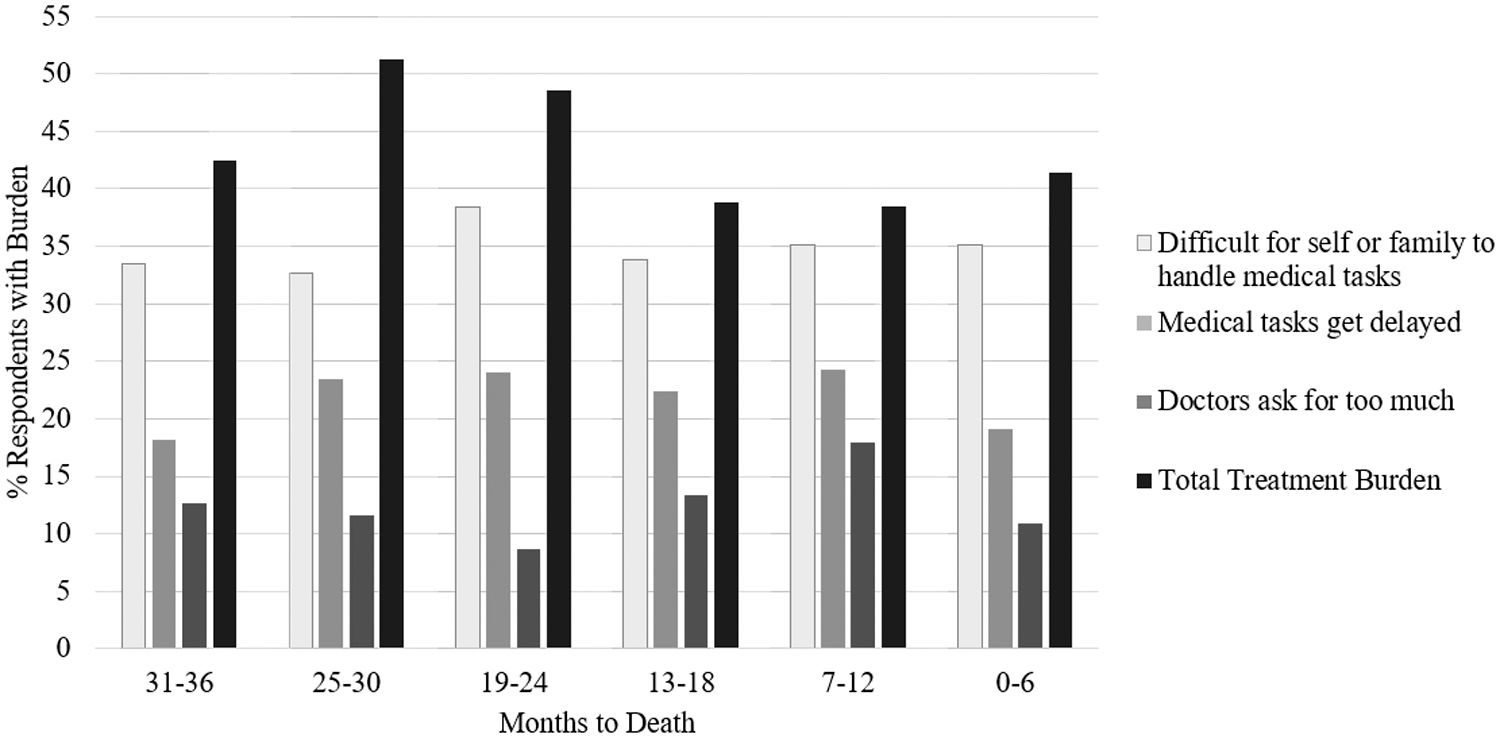
Prevalence of treatment burden in the general population in the last three years of life by six-month intervals.
Prevalence of Treatment Burden Among Older Adults in the Last Three Years of Life
Total TB defined as experiencing one or more of the above treatment burden items.
MCCs, multiple chronic conditions.
Aim 2: Characterizing treatment burden among older adults with MCCs
The prevalence of treatment burden was slightly higher among those with MCCs (43.7%). In our bivariate analysis, we found that rates of treatment burden varied significantly by race (Table 2). Among those with treatment burden, 8.7% self-reported as non-Hispanic black and 10.0% self-reported as Hispanic, compared with 5.9% and 4.0% among those without burden, respectively (p < 0.05). Self-report of cancer was significantly associated with treatment burden, with 44.4% of those with burden reporting a cancer diagnosis, compared with 51.1% without burden (p < 0.05); 34.3% of individuals with burden reporting depression, compared with 22.3% without burden; and 28.7% reporting anxiety, compared with 17.7% without burden (p < 0.05).
Unadjusted Bivariate Analysis of Sociodemographic, Health, Workload, Capacity, and Care Context Associations with Treatment Burden among Older Adults with Multiple Chronic Conditions
Bolded p-values indicate significant values.
Table 3 reports the results of logistic regression models examining predictors of treatment burden among older adults with MCCs in their last three years of life. We did not find a statistically significant association between clinical characteristics and treatment burden in our adjusted models.
Logistic Regression Predicting Treatment Burden with Sociodemographic and Mental Health Factors
Model 1: adjusted for age, sex, race, and years to death.
Model 2: adjusted for age, sex, race, years to death, depression, anxiety, and self-report of cancer.
Discussion
In a nationally representative study of older adults, we determined the prevalence of treatment burden over the last three years of life. This is the first study to assess treatment burden in this population and to measure trends in treatment burden as individuals approach death. We found that 43.3% of older adults in their last three years of life experienced treatment burden. This is higher than previous estimates of the prevalence of burden (37.9%) in the general population of older adults. 9
Notably, our data demonstrate that rates of treatment burden remain high regardless of how close individuals are to their time of death, with similar rates among individuals in their last 2.5–3 years of life (42.5%) and individuals in their last six months of life (41.4%). With regard to individual measures of burden, 40–50% of respondents in each six-month cohort reported difficulty among themselves or their families in managing health care tasks. In contrast, only half that number of respondents attribute their burden to their physicians asking them to do too much. The sources of burden are varied and multidimensional and might not result directly from the orders of a physician. 34 For example, the difficulty associated with educating oneself about self-management practices or traveling to appointments can contribute to the burden of staying healthy,5,10,34 but may not be discussed with a doctor in the same way that a medication regimen is.
Given the well-acknowledged vulnerability of individuals with MCCs to treatment burden,13,14,17,34,35 we focused our analyses on older adults with two or more chronic conditions. Among those with MCCs in their last three years of life, 43.7% experienced treatment burden. Unlike previous studies of treatment burden in older adults, we did not detect significant associations with health characteristics such as age, self-reported health, and number of chronic conditions.9,36 These prior studies focused on different populations; Wolff and Boyd examined a nationally representative sample of older adults, while Schreiner et al.'s study focused on patients being discharged from skilled nursing facilities to home. Our study focused on those at the end of life, who may be more uniformly ill than other populations.
While we found significant associations between treatment burden and race, depression, anxiety, and cancer diagnosis in our bivariate analysis, these results were no longer statistically significant in adjusted models. The effect sizes for the association between treatment burden and both depression and race remained similar between bivariate and multivariable analyses, indicating that there may be an association that our sample size was not large enough to detect. Further research is necessary to better understand racial disparities in treatment burden. 34 Our bivariate analysis also indicated that individuals with depression reported higher rates of burden. Although the causal relationship between depression and burden cannot be determined in our data, previous studies have found that treatment burden was highly influenced by the social, emotional, and cognitive work of managing health care.9,21
Interestingly, we did not see an increase in burden levels among individuals closer to their time of death as hypothesized. One possible explanation is that older adults may already have established expectations for their treatments and therefore do not perceive potential elevations in disease complexity or objective treatment workload as increasing burden. Familiarity and acceptance of disease have been found to alleviate perceptions of burden.37,38 Still, it is important to consider reasons why treatment burden remains elevated, affecting almost half of individuals in their last years of life, in the last months of life. An emphasis on self-management of chronic illnesses, which does not acknowledge each patient's unique capabilities and circumstances, might contribute to the persistence of treatment burden through to the time of death. 39 Our study points to the need for clinicians to work with patients to balance treatment workload and capacity and ultimately decrease the burden of complex treatment regimens.
Several recommendations have been made to improve assessment of treatment burden in the clinical setting. Sheehan et al. propose delivering a short survey assessing treatment burden, such as the NHATS scale or the Multimorbidity Treatment Burden Questionnaire (MTBQ), 35 to provide clinicians with meaningful data capturing experiences of treatment burden as patients move through their illness trajectory. 40 The Minimally Disruptive Medicine research team has been exploring how to integrate this practice into doctor visits.41,42 Palliative care clinicians are well positioned to address this gap in person-centered care. Patients at the end of life have a wide range of preferences as to how much treatment burden they are willing to endure, 22 and perceptions of burden vary depending on individual circumstances.4,40,43 Our study is not able to distinguish heterogeneous trajectories at the end of life that may be masking rising treatment burden in subpopulations. It is therefore imperative for clinicians to remain attuned to mitigating treatment burden in a way that is consistent with patient goals. Palliative care clinicians are known to be skilled in acknowledging treatment preferences and goals of patients 11 and can be consulted to help older adults with MCCs weigh care decisions in the face of treatment burden.
Our study is limited to our measure of treatment burden, which varies greatly from other measures of burden. For example, the 48-item Patient Experience with Treatment and Self-Management (PETS) Questionnaire measures burden on a 4- or 5-point Likert scale and the 7-item TBQ assesses burden on a scale from 0 to 10.44,45 The 10-item MTBQ was created to measure burden among MCC populations. 35 The TBQ, MTBQ, and PETS assessments have all been validated for populations with chronic conditions, and the NHATS survey is the only measure that has been used to assess national trends in treatment burden. We modified our measure of burden slightly from the only prior study using this NHATS measure to better capture treatment burden across individuals with varying abilities to self-manage care, as described above. There is no gold standard measure of treatment burden, and future work should consider multiple assessments, including the Health Care Task Difficulty Scale assessing caregiver difficulty with health care activities, 13 to expand our understanding of how care networks experience treatment burden.
While our study is novel in taking advantage of the essentially random time interval between the NHATS survey and death to assess the trajectory of treatment burden over time, the sickest individuals who are closest to death are more likely to rely on proxy reporters, therefore potentially introducing measurement error that could lead to underestimation of treatment burden as death approaches. Finally, we were limited in our ability to compare trajectories of treatment burden across specific illnesses, such as different cancer types, and sociodemographic groups due to sample size, as treatment burden was only assessed in the Engagement in Health Care Module of the NHATS conducted in 2012. While the approach we used to assess trends in burden before death without relying on clinician prognostication has been well established,46–48 our study design and sample size make it difficult to follow the same individuals as they approach death and look at fine-grained intervals such as weeks or months before death.
We found that treatment burden persists at high rates among older adults and those with MCCs in their last three years of life. Our research builds on a foundation of qualitative research that has examined treatment burden at the end of life.19,21,49 To our knowledge, our study is the first to quantify treatment burden across the U.S. population of older adults at the end of life, and our results suggest the importance of considering treatment burden when building treatment plans for older adults, even as they approach the end of life.
Footnotes
Funding Information
This work was supported by the Patricia S. Levinson Summer Research Award from the Icahn School of Medicine at Mount Sinai.
Author Disclosure Statement
No competing financial interests exist.