
Abstract
Background:
Pain is common among patients with cardiopulmonary conditions; however, there are increasing concerns, but limited research, regarding use of opioids for pain in patients with noncancer conditions.
Objective:
To compare patterns of opioid prescribing among older adults reporting pain with cardiopulmonary conditions and/or cancer.
Design:
Observational study using data from the Surveillance, Epidemiology, and End Results-Medicare Health Outcomes Survey resource linked to Medicare Part D prescription claims.
Setting/Subjects:
We identified patients who self-reported moderate-to-severe pain interference with daily activities. Patients were stratified by (1) self-reported history of cardiopulmonary conditions; (2) were within five years of cancer diagnosis; (3) had both conditions; or (4) neither.
Measurements:
We characterized opioid prescribing within 30 days of survey and one-year follow-up using logistic regression and Cox proportional hazard time-to-event analyses.
Results:
Of 10,516 patients with moderate-to-severe pain (1758 cardiopulmonary conditions, 3383 cancer, 2861 both, 2514 neither), 46% were aged ≥75 years, 65% were non-Hispanic white, and 10% non-Hispanic black. At survey, 1627 (15.5%) received opioids. Adjusted proportions of opioid use were lower for patients with cardiopulmonary conditions only (14%) compared with cancer only (17%; p < 0.001) and both conditions (17%; p < 0.001) but higher than patients with neither condition (13.1%; p < 0.001). There was no difference in time to initiation of opioids at follow-up among patients with cardiopulmonary conditions only, relative to cancer only (adjusted hazard ratio 1.03; 95% confidence interval 0.88–1.21).
Conclusions:
Opioid use is lower among patients with pain and cardiopulmonary conditions relative to patients with cancer. Findings emphasize the importance of pain assessment and management for patients with cardiopulmonary conditions.
Introduction
Approximately 29
Opioids are the most commonly prescribed medications used for moderate to severe pain management. 13 However, there remains little guidance on the use of opioids for treatment of pain specific to older adults with cardiopulmonary conditions. Opioids are discussed in the context of dyspnea, not pain, in cardiopulmonary condition clinical management guidelines.14,15 Moreover, although opioids are a mainstay of treatment for cancer-related pain, nonopioid therapy is preferred for noncancer-related pain as first-line therapy. 16 Recent studies have reported higher rates of opioid use among older adults with pain and cancer, relative to those with cardiopulmonary conditions.17–20 However, few population-based studies have examined patterns of and characteristics associated with opioid prescribing among patients with these conditions and how prescribing and characteristics change over time.8,11,13
Understanding patterns of opioid use among older adults with cardiopulmonary conditions and pain has become an important research focus due to competing interests over providing adequate pain relief with concerns over opioid efficacy, side effects, and safety.21,22 Similar to patients with cancer, 8 demographic and clinical characteristics may facilitate or impede opioid receipt. In this context, characterizing opioid prescribing patterns among older adults with pain and cardiopulmonary conditions and cancer is essential to identify and address barriers to appropriate and safe pain management. Therefore, we sought to compare patterns of opioid prescribing among older adults with cardiopulmonary conditions and/or cancer. We hypothesized that fewer patients with cardiopulmonary conditions would be prescribed opioids and would be less likely to receive opioids over time relative to patients with cancer.
Methods
Data
Our data source was the Surveillance, Epidemiology, and End Results (SEER)-Medicare Health Outcomes Survey (MHOS) with a novel linkage to Medicare Part D claims. SEER provides detailed cancer registry data from selected regions within the United States, including cancer types, stage, histology, and diagnosis date. MHOS is administered by the Centers for Medicare and Medicaid Services (CMS) and includes self-reported sociodemographic characteristics as well as responses to a chronic condition checklist and health and functional status questions on the Veteran's Rand 12 item survey (VR-12). 23 The survey is administered annually to randomly sampled Medicare beneficiaries enrolled in Medicare Advantage (MA) plans. The SEER-MHOS represents a linkage of patients with a SEER-reported cancer who responded to an MHOS survey and MHOS respondents without cancer who reside in SEER regions.23,24 Medicare Part D prescription drug claims for the period from 2007 through 2014 were linked for Part D-enrolled MHOS respondents.
Sample selection
We selected patients who reported moderate-to-severe pain interference with daily activities. Pain interference was measured using the Bodily Pain subscale of the VR-12 survey, 25 which asks, “During the past 4 weeks, how much did pain interfere with your normal work (include both work outside the home and housework)?” Patients were included in the sample if they reported moderate (some of the time) or severe (quite a bit, extremely) pain on the VR-12 pain interference question, as reported in past reports.8,26
We stratified patients by health condition to include patients with (1) cardiopulmonary conditions only, (2) cancer only, (3) both conditions, or (4) neither. Patients were included in the cardiopulmonary conditions only group if they self-reported having any of the following conditions on the MHOS chronic condition checklist: coronary artery disease, heart failure, other heart problems, emphysema, asthma, and COPD. We selected patients with cardiopulmonary conditions who completed at least one MHOS between January 2008 and December 2012, resided in a SEER region at survey, and who did not self-report cancer on any MHOS survey. Patients were included in the cancer group if they had only one primary cancer, any invasive disease or Stage 0 breast cancer, and were diagnosed between January 2003 and December 2012 per the MHOS-SEER dataset. Patients in the cancer group had to complete at least one MHOS between January 2008 and December 2012 within five years after their cancer diagnosis. Patients with both cardiopulmonary conditions and those with neither condition were stratified into separate groups for analysis. We excluded patients if they self-reported a cancer history on the MHOS that did not correspond to a SEER diagnosis, their cancer diagnosis month was unknown or if the cancer diagnosis was first reported on a death certificate or autopsy, those whose age was ≤65 years at MHOS date, and those without continuous enrollment in Medicare Parts A, B, MA, and Part D during the 12 months pre–post the MHOS month or until death.
Outcome measures and covariates
The primary outcome was receipt of prescription opioid medications for treatment of pain. We also collected data on nonopioid prescription pain medications. We created categories of opioids, nonopioid analgesic (nonsteroidal anti-inflammatory drugs, local anesthetics), and adjuvant pain medications (antiepileptics and selected antidepressants). We did not include steroids because they are prescribed for multiple clinical conditions and we were unable to distinguish the indication for use. We identified and categorized relevant individual medications for pain based on input from the literature,18,27 clinical guidelines, 28 and with consultation with clinicians and pharmacists with specialization in palliative care and oncology. Next, we searched Part D claims to identify relevant generic drug names, including combination medications. We searched for evidence of drug supply by prescription during two time periods: (1) the MHOS date and prior 30 days; and (2) the 12 months after the MHOS.
Study covariates included beneficiary demographics (age, race/ethnicity, gender, marital status, and educational attainment), chronic conditions, beneficiary death within 12 months of survey date, zip-code level percentage of the population living in poverty, region (Northeast, South, Midwest, and West) as defined by the U.S. Census Bureau, MA plan type (health maintenance organization or preferred provider organization [PPO]/other) and receipt of the Part D low-income subsidy (LIS, full or partial vs. none). We selected chronic conditions with known associations with pain that were available on the self-reported chronic condition checklist on the MHOS. All models controlled for pain interference (moderate and severe). For patients with cancer we report cancer type (breast, prostate, colorectal, lung, and other), cancer stage at diagnosis, and initial therapy derived from SEER.
Analysis
We used chi-square or Student's t tests to describe sample characteristics overall and by condition (cardiopulmonary conditions, cancer, both, and none). We calculated sample percentages receiving pain medications by type (any, opioid, nonopioid, and adjuvant) and compared percentages across conditions using chi-square analysis. We estimated multivariable logistic regression models to test for associations between conditions and opioids at MHOS survey, adjusting for covariates. Results are reported as predictive margins and 95% confidence intervals (CIs). Next, we conducted Cox proportional hazard time-to-event analyses to examine associations between condition group and time to opioid initiation, conditional on no opioids observed at MHOS survey date. Death during follow-up and survival past 12 months with no opioid prescribed were treated as censoring events. In sensitivity analysis we stratified the sample by patients who did and did not die during the 12 months of follow-up. Models were adjusted for covariates previously described as well as nonopioids and adjuvant medications during the initial observation period. All comparisons were two-sided with α = 0.05. Analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, NC) and Stata 15 (Statacorp, College Station, TX). Per federal regulation 45 CFR 46.101(b)(4), the Yale Human Investigation Committee determined that this research was exempt from further review.
Results
The sample included 10,516 patients of which 1758 had cardiopulmonary conditions, 3383 had cancer, 2861 had both conditions, and 2514 had neither. Of the sample, 45.6% were ≥75 years, 49.2% were male, and 65% were white non-Hispanic ethnicity (Table 1). More than 50% of the sample came from the West census region (54.9%), and 24.2% received the Part D LIS. More than two-thirds (68.4%) of the sample reported moderate pain interference and 31.6% reported severe pain levels. Nearly one-quarter (23.2%) of the sample died within one year of MHOS date. Additional characteristics specific to patients with cancer are reported in the Supplementary Table S1. Beneficiary characteristics among condition groups differed significantly for all characteristics except education level and insurance plan type. Patients with both conditions (40.9%) followed by cardiopulmonary conditions (37.8%) had the highest proportions of severe pain, followed by cancer only (26.2%) and neither condition (23.9%; p < 0.001). Mortality was highest among patients with both conditions, with 34.8% dying in the year after MHOS date, followed by cancer (24.1%), cardiopulmonary conditions (21.3%), and neither (9.8%) (p < 0.001).
Sample Characteristics N = 10,516
Source: SEER-MHOS-Part D linked data, 2008–2012.
p Value reported for comparison of distribution across health conditions.
HMO, health maintenance organization; LIS, low-income subsidy; MHOS, Medicare Health Outcomes Survey; N/A, not applicable; SEER, Surveillance, Epidemiology, and End Results.
More than 27% of patients received pain medication at MHOS survey date, with 15.5% receiving an opioid, 21.9% receiving a nonopioid analgesic, and 19.2% receiving an adjuvant pain medication (Fig. 1). Unadjusted medication rates overall and for each medication category were highest among patients with both conditions, followed by patients with cardiopulmonary conditions and patients with cancer only. For example, 19.7% of patients with both conditions, 15.8% of patients with cardiopulmonary conditions, 14.9% of cancer patients, and 11.3% of patients with neither condition reported opioids at baseline (p < 0.001).

Medication therapy for pain management by type, overall, and by condition (unadjusted).
Factors associated with receipt of opioids
In adjusted models, among patients with cardiopulmonary conditions, 13.8% received opioids at MHOS survey date (95% CI 12–15%) compared with 16.7% of patients with cancer only (95% CI 15.4–18%; p < 0.001; Fig. 2). There were no differences in adjusted proportions among patients with both conditions relative to patients with cancer only (p = 0.82). At the time of MHOS survey, 9.6% (95% CI 8.9–10.4%) of patients with moderate pain and 26.5% (95% CI 24.9–28.0%) of patients with severe pain received opioids (p < 0.001; Table 2). Opioid receipt was higher for women (16.5%; 95% CI 15.5–17.4%) compared with men (14.4%; 95% CI 13.4–15.3%, p = 0.004), decreased with increasing age >74 years, and increased for patients who reported stroke, arthritis, or sciatica (p < 0.05 for all). Among patients who died in the year after MHOS, 19.9% had opioids prescribed at the time of MHOS survey (95% CI 18.3–21.5%) compared with 14% of patients who did not die during follow-up (95% CI 13.2–14.7%; p < 0.001).

Adjusted levels (predictive margins) for opioid medication receipt by condition.
Adjusted Levels (Predicted Margins) for Use of Opioids at Survey
Source: SEER-MHOS-Part D linked data, 2008–2012.
p Values reported for comparison of predictive margins for each attribute compared with a reference category.
CI, confidence interval; HMO, health maintenance organization; LIS, low-income subsidy; MHOS, Medicare Health Outcomes Survey; SEER, Surveillance, Epidemiology, and End Results.
Factors associated with initiation of opioids at follow-up
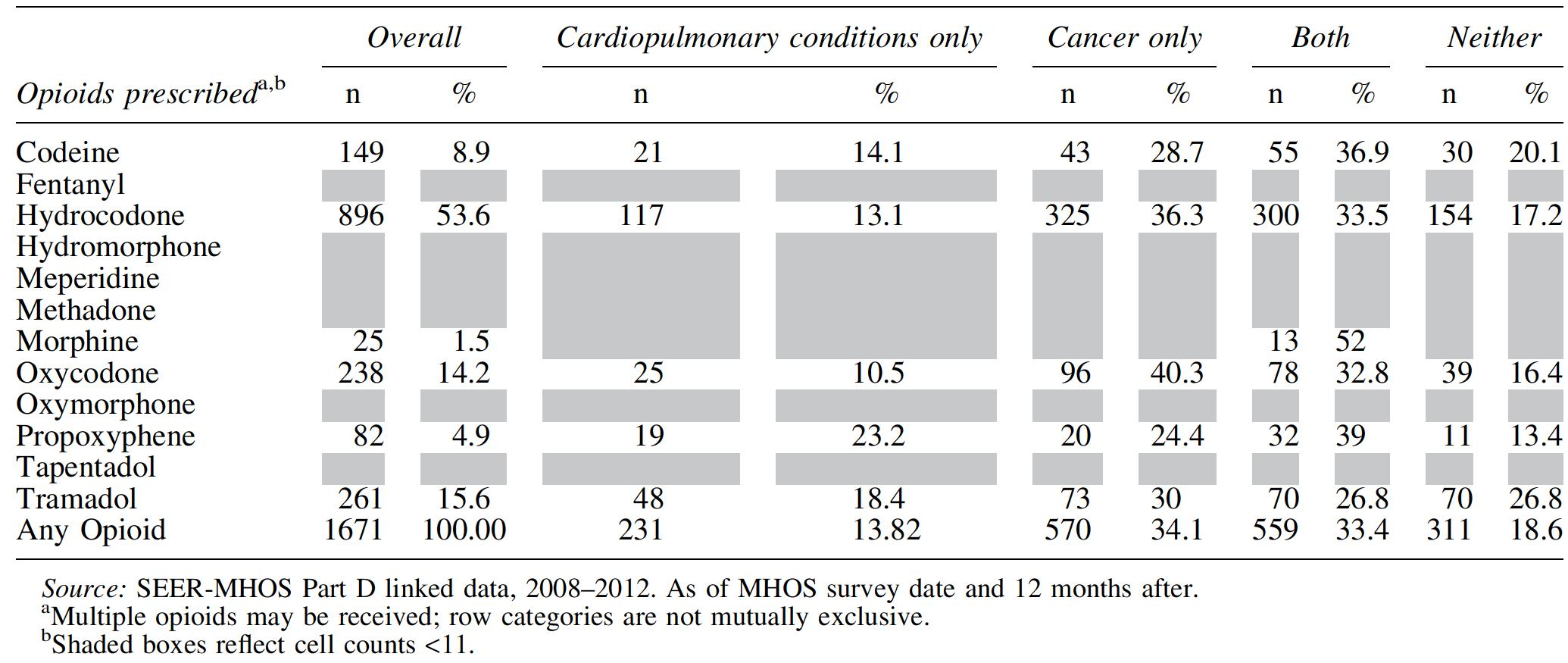
Among those without opioids at survey (n = 9104), opioids were initiated for 18.4% (n = 1671) of patients. Thirty-four percent of patients with cancer received opioids at follow-up, followed by 33.5% of patients with both conditions, 18.6% with neither condition, and 13.8% with cardiopulmonary conditions (Table 3). Of the total sample who received opioids at follow-up, 53.6% received hydrocodone, 15.6% received tramadol, and 14.2% oxycodone. In unadjusted analysis patients with cardiopulmonary conditions had the shortest median time to initiation of opioids (77 days; 95% CI 56–102), followed by patients with both conditions (81 days; 95% CI 70–92), cancer only (93 days; 95% CI 81–107), and neither (105 days; 95% CI 85–123).
Opioids Prescribed at Follow-Up
In adjusted time-to-event analyses, relative to cancer, there were no significant differences in the time to initiation of opioids among patients with cardiopulmonary conditions or among patients with both cardiopulmonary conditions and cancer (Table 4). There was no difference in time to initiation of opioids by covariates, including age group, gender, race/ethnicity, education, chronic conditions, region, part D LIS, plan type, or death within one year of survey date. Patients with a prescription for nonopioid analgesics or adjuvant medications at the time of survey were more likely to receive opioids at follow-up relative to patients without analgesics or adjuvant medications at MHOS survey date (nonopioid analgesics adjusted hazards ratio [AHR] 1.63, 95% CI 1.31–2.02; adjuvant pain medications AHR 2.90, 95% CI 2.40–3.49). In sensitivity analysis there was no difference in time to initiation of opioids by condition group among patients who died during follow-up (Supplementary Table S2).
Hazard Ratios for Time to Initiation of Opioids
Source: SEER-MHOS-Part D linked data, 2008–2012.
p Values reported for comparison of hazard ratios for each attribute compared with a reference category.
CI, confidence interval; HMO, health maintenance organization; HR, hazard ratio; LIS, low-income subsidy; MHOS, Medicare Health Outcomes Survey; SE, standard error; SEER, Surveillance, Epidemiology, and End Results.
Discussion
Using a novel linkage between the MHOS survey, the SEER cancer registry, and Medicare Part D claims data among patients ≥65 years, we found that patients with cardiopulmonary conditions who reported moderate to severe pain were almost 20% less likely to receive an opioid relative to patients with cancer at baseline. However, when followed over time, those patients with cardiopulmonary conditions with moderate to severe pain who were opioid naive at baseline were as likely as patients with cancer to receive opioids at follow-up. Taken together, our findings suggest that symptoms and symptom management, as opposed to specific health conditions or demographic and other clinical factors, guide clinician decision making regarding opioid prescribing. Moreover, our findings highlight the inherent complexities in examining patterns of opioid prescribing and the need for future research examining prescribing practices for these patients over time.
The findings support our hypothesis that rates of opioid prescribing are lower for patients with cardiopulmonary conditions compared with patients with cancer. This finding aligns with prior research, which also found less use of opioids in cardiopulmonary condition populations using administrative claims.17,18 For example, Barbera et al. found rates of opioid prescribing that were 43% and 26% higher among patients with recent and past cancer relative to noncancer patients, respectively. 17 Opioids have long been a mainstay treatment for patients with cancer experiencing pain.29,30 Although patients with cardiopulmonary conditions often report pain as frequently and of similar severity to patients with cancer, 31 clinical practice guidelines offer few recommendations for the treatment of pain for these conditions. Moreover, clinicians may feel unease in prescribing opioids for the treatment of pain in this population, for whom prognosis is less clear relative to patients with cancer. Although our data do not represent populations beyond 2012, given the 2016 US Centers for Disease Control and Prevention (CDC) guidelines that recommend against the use of opioids for noncancer pain, 16 it is likely that the differences in use of opioids among cardiopulmonary conditions and cancer patients will continue.
Surprisingly, we found that opioid-naive patients with cardiopulmonary conditions who reported moderate to severe pain were just as likely to receive opioids at follow-up relative to cancer patients with similar pain levels. Patient demographic and clinical characteristics were significantly associated with an opioid prescription at baseline in addition to disease condition and pain interference. Others have also found that characteristics, including younger age32,33 and female gender33,34 are associated with increased prescriptions for opioids in nonmalignant conditions. These characteristics were not associated with an opioid prescription in the results of our time-to-event analysis; only severe pain interference (relative to moderate) and the use of nonopioid analgesics and/or adjuvant pain medications were associated with an opioid prescription. Moreover, models accounted for death during follow-up. If more patients in the cancer group died before having the opportunity to receive opioids, differences between groups would be closer to the null. Thus, this finding may suggest that pain severity and adequacy of pain management at baseline drive downstream opioid prescribing, potentially overcoming clinicians' reluctance to prescribe opioids among patients with noncancer pain. Alternatively, completion of the MHOS survey might have activated patients to seek out treatment for untreated or undertreated pain, resulting in similar opioid prescribing among patients with cancer and cardiopulmonary conditions.
Although our findings appear contradictory, they reflect the nuances and inherent complexities in examining opioid prescribing patterns among patients with malignant and nonmalignant conditions. To our knowledge, little research has examined the drivers of opioid prescribing among patients with both cardiopulmonary conditions and cancer over time and the juxtaposition of both provider and patient behaviors that underpin the eventual decision to prescribe opioids to these patients. Although our findings suggest symptoms, symptom severity, and prior therapeutics are primary considerations in the decision to prescribe opioids among patients with cardiopulmonary conditions, more research is needed. Moreover, there remains controversy over the appropriateness and use of opioids for patients with cardiopulmonary conditions as well as other nonmalignant conditions. Our findings emphasize the importance of pharmacological and nonpharmacological interventions that target pain management to augment downstream opioid prescribing among patients with cardiopulmonary conditions.
This study had several limitations. First, this study was conducted in a sample derived from MA participants, which may limit the generalizability of study findings. Opioid prescribing practices may differ among patients with cardiopulmonary conditions versus cancer because of differences in the demographic and clinical characteristics of participants enrolled in other insurance programs such as traditional Medicare that offer alternative prescription benefits. Second, we were unable to include nonprescription pain medications in the analysis and thus likely underestimated patients' use of nonopioid medications for pain management. Third, we relied on self-reported measures of health conditions and symptoms, which may result in under-reporting. Fourth, our analysis reflects opioid prescriptions rather than the actual ingestion of the opioid by the patient, a limitation of any study utilizing claims data for opioid research. Fifth, we could not differentiate between opioids prescribed for pain and those prescribed for dyspnea, although opioids are often prescribed to address pain and dyspnea in tandem, particularly for patients with cardiopulmonary conditions for whom dyspnea is a common complaint. Sixth, patients ≥80 years are heterogenous and prescribing patterns likely differ by age among this group. Finally, although we could not control for heart failure or COPD severity, we did control for symptom severity, both of which likely impact the timing of when opioids are prescribed.
Conclusion
In a population-based sample of older adults with moderate to severe pain we found that patients with cardiopulmonary conditions were less likely to receive opioids relative to patients with cancer. However, among patients who were opioid naive, those with cardiopulmonary conditions were as likely to receive opioids during one-year follow-up as cancer patients. Study findings suggest that pain severity and prior use of therapeutics may drive opioid prescribing over specific health conditions and emphasize the importance of timely pain assessment and management for patients with cardiopulmonary conditions.
Footnotes
Authors' Contributions
All authors participated in all aspects of the conduction of the study and manuscript preparation.
Acknowledgments
The authors acknowledge the efforts of the National Cancer Institute, the CMS, Information Management Services (IMS), Inc., and the SEER Program tumor registries in the creation of the SEER-MHOS database.
Funding Information
S.L.F. received funding from the CTSA Grant Number TL1 TR001864 from the National Center for Advancing Translational Science (NCATS), a component of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH. S.L.F. was also supported by the Department of Veterans Affairs Office of Academic Affiliations through the National Clinical Scholars Program. C.J.P. is a Paul Calabresi Scholar supported by the OSU K12 Training Grant for Clinical Faculty Investigators (K12 CA133250) and is a consultant for Potentia Metrics. S.W.'s institution receives funding from Genentech to support his research. In the past 36 months, J.S.R. received research support through Yale University from Medtronic, Inc., and the Food and Drug Administration (FDA) (U01FD004585), from the Centers of Medicare and Medicaid Services (CMS) (HHSM-500-2013-13018I), and from the Blue Cross Blue Shield Association to better understand medical technology evaluation; J.S.R. currently receives research support through Yale University from Johnson and Johnson, from the FDA (U01FD005938), from the Medical Device Innovation Consortium as part of the National Evaluation System for Health Technology (NEST), from the Agency for Healthcare Research and Quality (R01HS022882), from the National Heart, Lung and Blood Institute of the National Institutes of Health (NIH) (R01HS025164, R01HL144644), and from the Laura and John Arnold Foundation. A.J.D.'s institution receives research funding from Celgene Corporation. A.J.D. has a family member who receives consultant/advisory funding from Abbvie, Celgene, Daiichi Sankyo, Kyowa Hakko Kirin, Jazz Pharmaceuticals, and Tolero Pharmaceuticals. No other author reports any conflict of interest.
This research was funded through a contract with the National Cancer Institute (Contract HHSN261201700690P). This study used data from the SEER-MHOS-linked data resource. The interpretation and reporting of these data are the sole responsibility of the authors and do not reflect the positions of the National Cancer Institute, the CMS, or the U.S. Department of Health and Human Services.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.