
Abstract

Dear Editor:
Over the past several weeks, the enduring undercurrent throughout our battle with the COVID-19 pandemic has been continued uncertainty—not only regarding clinical prognosis and understanding of the virus's effects, but also in addressing health care systems' day-to-day availability and allocation of resources. For nephrology providers, addressing unpredictability of the disease trajectory is largely familiar territory.1,2 Now, however, nephrology providers—along with other front-line providers in the ICUs and emergency rooms—are tasked with guiding our patients and colleagues through the process of dialysis decision making in the face of these added uncertainties. Compounding these issues is the heightened emotional state of patients and families as they hear bad news and struggle to make sense of the situation. How can we best respond to this situation?
By anchoring our dialysis decision-making conversations in a simple three-step communication framework, the Three-Stage Protocol, we can better navigate uncertainty, explore possible treatment pathways, and arrive at a goal-concordant recommendation. 3 The Three-Stage Protocol was originally designed for all clinicians who may not have had formal communication training and breaks down any serious illness conversation into (1) sharing knowledge of the medical condition with patients and families, with the overarching goal of delivering a clear prognostic statement (“the punchline”); (2) clarifying the patient's goals of care (GOC); and (3) making a recommendation based on the agreed-upon goals (Fig. 1).
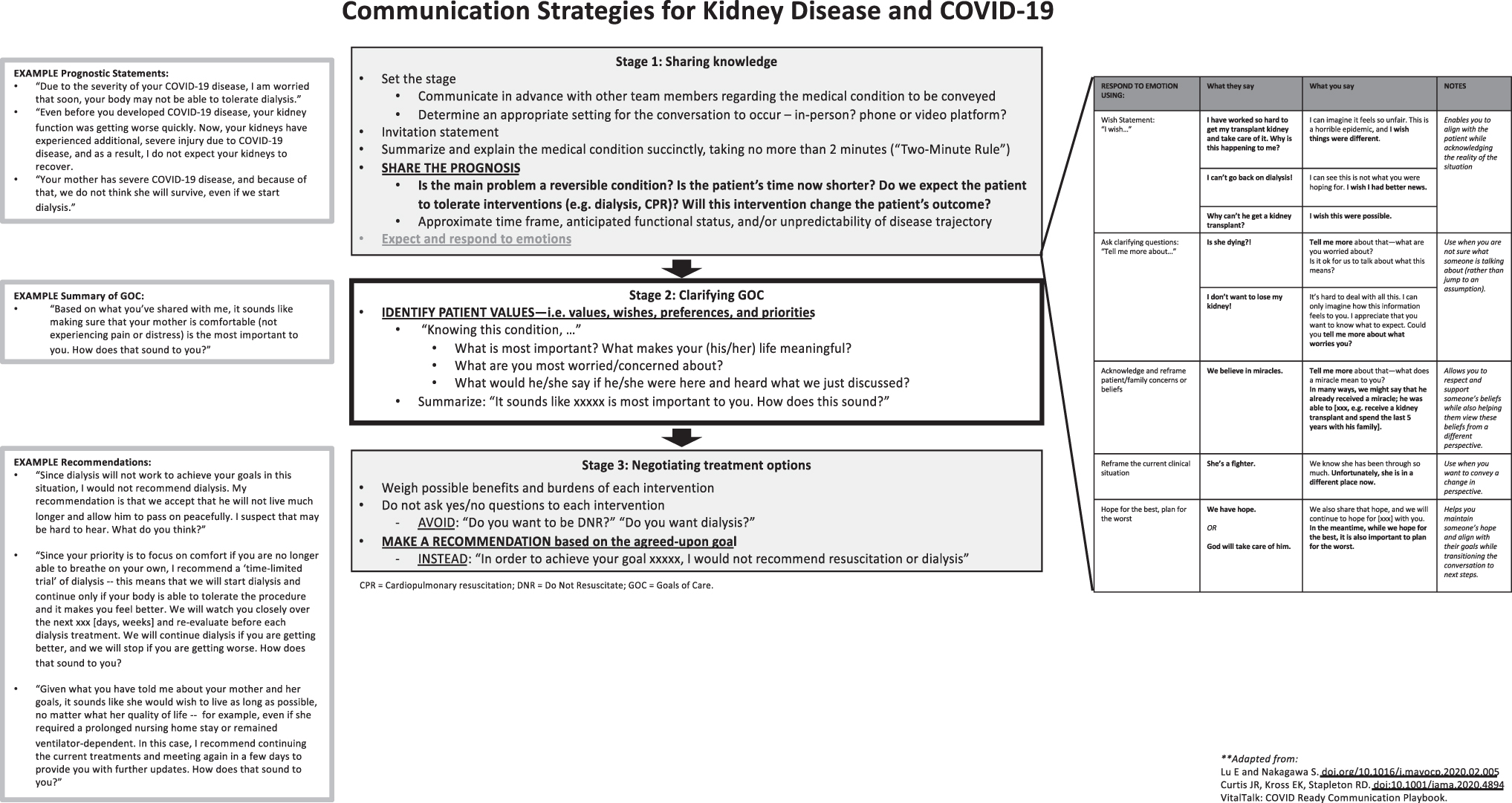
Communication strategies for kidney disease and COVID-19.
In this study, we have adapted the Three-Stage Protocol for dialysis decision making in the context of COVID-19, expanding on challenging scenarios, for example language, and common questions or emotional reactions that nephrology providers may continue to face in the coming days.
In Stage 1, after we have “set the stage” for the conversation, the focus is on sharing the prognosis effectively. This requires the provider to synthesize the available clinical and laboratory data into a single succinct statement that will then drive the rest of the conversation. This may depend on the provider's goals for the conversation, that is, whether the provider is “breaking bad news” or aims to discuss a change in treatment plan. Importantly, the prognostic statement may convey not only time as overall survival or renal survival and disease reversibility, but also of ability to tolerate dialysis in this context and/or expectation of dialysis to change the outcome. An effective prognostic statement removes some of the uncertainty for the patient and provider, such that both are now on the same page (Fig. 1).
In response to the prognosis delivered, we expect significant emotional responses. These emotions may reflect both the prognostic information they have just received and the underlying uncertainty shared by clinicians. Providers may be faced with challenging emotional statements; in these situations, it is helpful to be prepared with different communication techniques that can avoid escalating emotions and further distress (Fig. 1).
The Three-Stage Protocol emphasizes following these steps in a sequential manner to ensure that identifying the patient's GOC is not overlooked, regardless of the urgency of the situation. This, in turn, makes sure that instead of asking, “Do you want dialysis?” or opening the conversation with, “It looks like you will need dialysis soon,” we are able to make a comprehensive recommendation that accounts for the patient's overall clinical picture and priorities (Fig. 1). In some cases, a time-limited trial may be best aligned with patient goals. Similarly, an “informed assent” approach may be appropriate if the patient's goals are clear. 4
In this way, the Three-Stage Protocol can help patients, families, and providers define a concrete plan despite all of the uncertainties of COVID-19. One caveat to using the Three-Stage Protocol, however, is that it is not designed for crisis care situations in which resources or interventions (e.g., dialysis) are rationed or no longer offered; for this, we suggest additional resources. 5 Furthermore, we encourage continued early collaboration with interdisciplinary palliative care colleagues, who can provide communication skills expertise for challenging situations. Together, we thus aim to help organize—if not remove—the uncertainty surrounding our care of patients during this time.