
Abstract
Background:
Palliative care is expanding as part of treatment, but remains underutilized in trauma settings. Palliative care consultations (PCC) have shown to reduce nonbeneficial, potentially inappropriate interventions (PII), as decision for their use should always be made in the context of both the patient's prognosis and the patient's goals of care.
Objective:
To characterize trauma patients who received PCC and to analyze the effect of PCC and do-not-resuscitate (DNR) orders on PII in severely injured patients.
Setting/Subjects:
Retrospective cohort study of 864 patients admitted to two level 1 trauma centers: 432 patients who received PCC (PCC group) were compared with 432 propensity score match-controlled (MC group) patients who did not receive PCC.
Measurements:
PCC in a consultative palliative care model, PII (including tracheostomy and percutaneous endoscopic gastrostomy) rate and timing, DNR orders.
Results:
PCC rate in trauma patients was 4.3%, with a 5.3-day average time to PCC. PII were done in 9.0% of PCC and 6.0% of MC patients (p = 0.09). In the PCC group, 74.1% of PII were done before PCC, and 25.9% after. PCC compared with MC patients had significantly higher mechanical ventilation (60.4% vs. 18.1%, p < 0.001) and assisted feeding requirements (14.1% vs. 6.7%, p < 0.001). We observed a statistically significant reduction in PII after PCC (p = 0.002). Significantly less PCC than MC patients had PII following DNR (26.3% vs. 100.0%, p = 0.035).
Conclusions:
PCC reduced PII in severely injured trauma patients by factor of two. Since the majority of PII in PCC patients occurred before PCC, a more timely administration of PCC is recommended. To streamline goals of care, PCC should supplement or precede a DNR discussion.
Background
Palliative care (PC) is expanding as part of treatment in medical and surgical patients; however, it remains underutilized in trauma settings. Data on the prevalence and timing of PC in trauma patients are scarce and inconsistent, varying widely depending on the studied population and implemented PC model. Lilley et al. reported that among trauma patients 65 years or older who died within 180 days of discharge, only 2.1% received inpatient PC. 1 Benjenk et al. found a 33.9% rate of palliative care consultations (PCC) in a group of severely injured trauma patients. 2 Hua et al. described a 14.7% rate of PCC in trauma/burn intensive care unit (ICU) patients at their institution with a trigger-based model of PC. 3
Clinicians agree that PC implementation improves end-of-life planning, increases patient and family satisfaction, and reduces ICU cost.4–10 Furthermore, PCC have shown to potentially reduce nonbeneficial services.11,12 Potentially inappropriate interventions (PII) can cause patients physical and mental suffering, and financial burden with no benefit. However, published data on PII remain sparse, particularly in trauma patients.
Tracheostomy (TS) and percutaneous endoscopic gastrostomy (PEG) are some of the most common PII. A study by Hoffman emphasized that the need for TS and PEG portends a poor prognosis, and therefore, the decision to place a TS or a PEG should always be made in the context of both the patient's prognosis and the patient's goals of care. 13 This is in line with a reported high mortality of 19.2% in patients with TS, who are often some of the sickest of all. 14
A limited number of previous studies looked at the effects of PCC on PII, but those were completed in medical and surgical ICU.15–18 Therefore, an analysis of PII in trauma patients with PCC warrants additional investigation.
Objective
The objective of this study was to describe the characteristics of trauma patients who received a PCC and to analyze the effect of a PCC and do-not-resuscitate (DNR) order on PII in the care of severely injured patients at two level 1 trauma centers. We hypothesized that the number of PII would be reduced after a PCC in this group of patients.
Methods
This institutional review board-approved, retrospective cohort study was granted a waiver of informed consent and included 864 patients admitted to two level 1 trauma centers between December 2012 and May 2019. The exclusion criteria were as follows: age 16 and younger, and death within 24 hours of admission to a trauma center.
Four hundred thirty-two patients who received a PCC during their hospital stay were identified from hospital records and designated as the PCC group. The other 432 patients were propensity score matched from the remaining 10,056 admitted trauma patients who did not receive a PCC and designated as the match-controlled (MC) group. The use of propensity matching was intended to equalize the quantitatively mismatched populations of patients with and without a PCC. The propensity match covariates included the following: injury severity score (ISS), mechanism of injury, gender, and hospital length of stay (HLOS). This approach ensured the comparability of both groups in the severity and mechanism of injury and access to PC. The HLOS matching was important, as it was shown previously that trauma patients with HLOS of more than four days had significantly greater odds of receiving a PCC. 2 The four covariates chosen for propensity matching were thought to most significantly affect the outcome, which was the implementation of a PCC. The matching resulted in two comparable groups that were similar in these four major characteristics.
Palliative care is a comprehensive approach that not only includes discussion about the goals of care, advanced directives, and pain management, but it also addresses the PII. The definition of a “potentially inappropriate” treatment has evolved over time, and it is the recommended term to describe all treatments that have at least some chance of accomplishing the effect sought by the patient. The term “futile intervention” should be restricted to describe procedures that cannot accomplish the intended goal but are requested by the patient's surrogate. 19 The study was focused on only one aspect of PC and included patients who received a PCC for discussion of the withdrawal of curative treatment.
The comparison of the PCC and MC groups included variables: age, race, Glasgow Coma Score (GCS), traumatic brain injury (TBI) incidence, DNR order presence, mechanical ventilation requirement, ICU admission, and mortality. Mortality data included in-hospital mortality and mortality within six months after discharge. Additional analyses included the rates and timing of PII in both groups.
The two most common PII, TS or PEG, were analyzed. Within the PCC group, the timing of PII was analyzed in two scenarios, whether it preceded or followed the PCC. We also studied the timing from admission and the documented reasons for TS and PEG placement. To analyze if PCC had an impact on PII, we extracted the frequency of TS and PEG recommendations from consultation reports. We then used the frequency of PII recommendations to calculate the rate of PII placed to the PII recommended.
All variables were identified via ICD-9 codes, ICD-10 codes, and extracted from patients' medical records. In patients with a noted DNR order (prehospital or in-hospital) a “DO NOT RESUSCITATE ORDER” form and a “Withhold or Withdrawal of Life-Prolonging Procedures Consent” form were used. The first form is an agreement to withdraw cardiopulmonary resuscitation (CPR) or resuscitative methods in the event of cardiac or respiratory arrest, while the second form is used to consent to withholding of life-sustaining treatments, such as mechanical ventilation or artificial nutrition.
Statistical analysis was performed using IBM SPSS Statistics software version 23.0 (IBM, Armonk, NY). Propensity matching was done without replacement, 1:1, and with a caliper of 0.02. The analyses included group characteristics and bivariate correlation comparisons. Categorical variables were analyzed with the chi-squared test. Variable means were analyzed using independent samples t-test and Mann–Whitney U test depending on the distribution. One-way analysis of covariance (ANCOVA) was used to account for confounding variables, such as the presence of TBI, age, GCS, and ICU admission, in the analysis of reduction of PII following a PCC. Statistical significance was assumed when the calculated p-value was below 0.05.
Results
PCC were implemented in 4.3% of all trauma patients admitted to our two level 1 trauma centers. Patients in the PCC and MC groups had a comparable average ISS of over 17 (≥16 denotes a serious injury), which resulted from falls in more than 80.0% of both populations. The two groups were predominantly male (60.0%) and stayed in the hospital on average seven to eight days. The average time to PCC was 5.3 days.
Patient characteristics are presented in Table 1. The PCC group was older, more often white race, with lower GCS, higher TBI incidence, higher rate of DNR, higher requirements of mechanical ventilation, more ICU admissions, and higher mortality. In the PCC group, 8.1% of patients were discharged to a skilled nursing facility or a rehabilitation center, 3.9% expired in-hospital, and 87.7% of patients were discharged to hospice, with a total mortality of 90.7% within six months of discharge. In the MC group, 41.0% of patients were discharged home, 40.8% were discharged to a skilled nursing or rehabilitation facility, and 3.9% expired in-hospital.
Characteristics of Palliative Care Consultation and Match-Controlled Groups
Denotes a statistically significant difference.
DNR, do-not-resuscitate; ICU, intensive care unit; MC, match controlled; PCC, palliative care consultations.
Overall, PII were performed in 9.0% of PCC patients and in 6.0% of MC patients (p = 0.09). The distribution of all PII in both groups is presented in Figure 1. In the PCC group, 40 PII (74.1%) were done before the PCC, and 14 (25.9%) were done after. There were a total of 39 patients in the PCC group with 54 PII. The mortality in this patient population was 92.3%, with 64.0% of PII being placed by request of the family. Furthermore, 57.4% of PII were implemented after the first week from admission/trauma, which was not part of the immediate care.
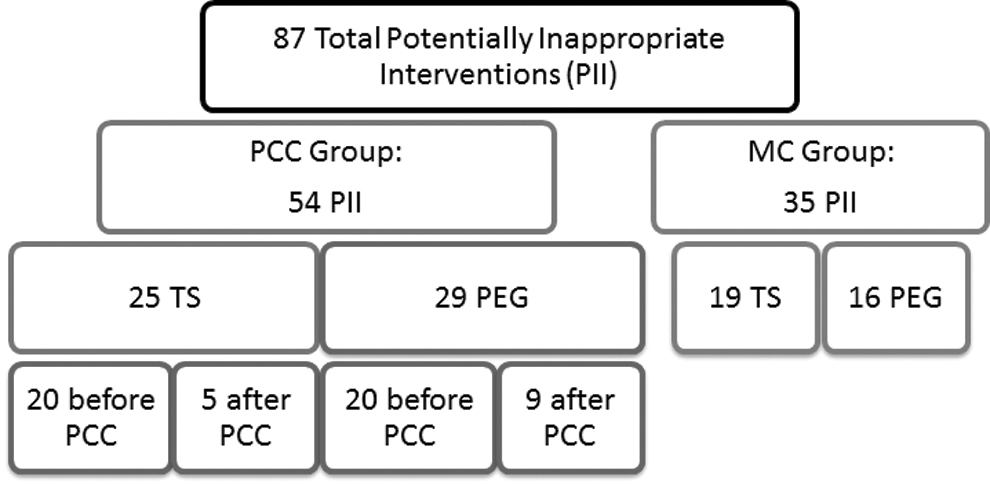
Number of potentially inappropriate interventions (TS and PEG) in PCC and MC groups. MC, match controlled; PCC, palliative care consultations; PEG, percutaneous endoscopic gastrostomy; TS, tracheostomy.
The number of PII in regard to PCC timing is presented in Figure 2. When comparing PII in the MC group with PII done after PCC in the PCC group, there was a statistically significant reduction in the number of PII performed after a PCC (p = 0.002). ANCOVA showed that having a PCC was a statistically significant factor (p = 0.001) affecting the number of PII, when controlling for confounding variables that were found to be significantly different between the PCC and MC groups. The rate of PII in PCC and MC groups was statistically significantly different (p = 0.001) when adjusted for TBI, age, GCS, and ICU admission. In the analysis of PII before the PCC, adjusting for the same confounding variables, there was no difference in the rate of PII (p = 0.448). The distribution of patients with PII in the PCC group is presented in Figure 3. The majority of PCC patients had all PII before a PCC, with 17.9% of patients having either a TS or a PEG before and the other PII after a PCC.
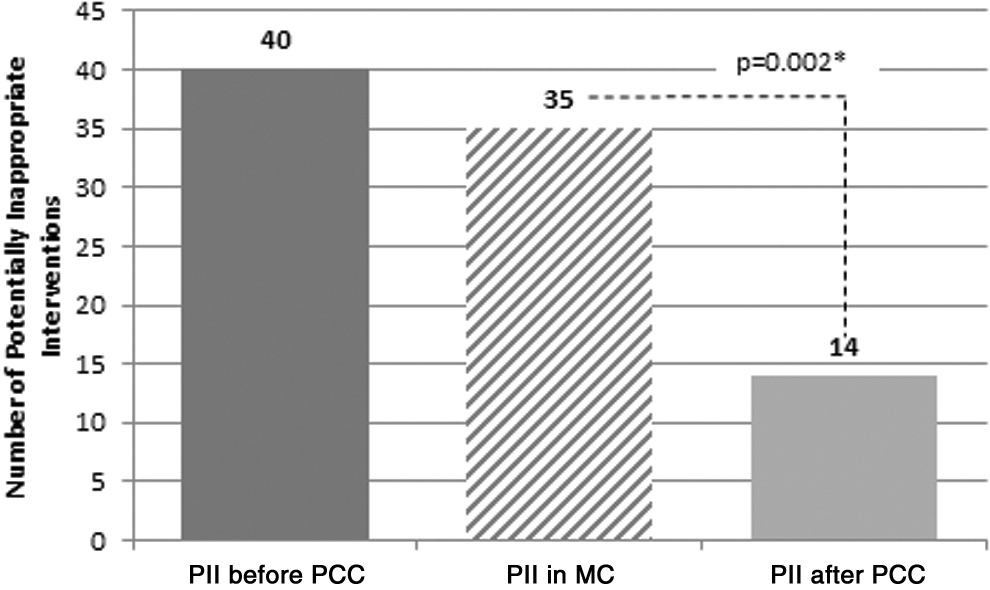
Timing of potentially inappropriate interventions in PCC and MC groups.
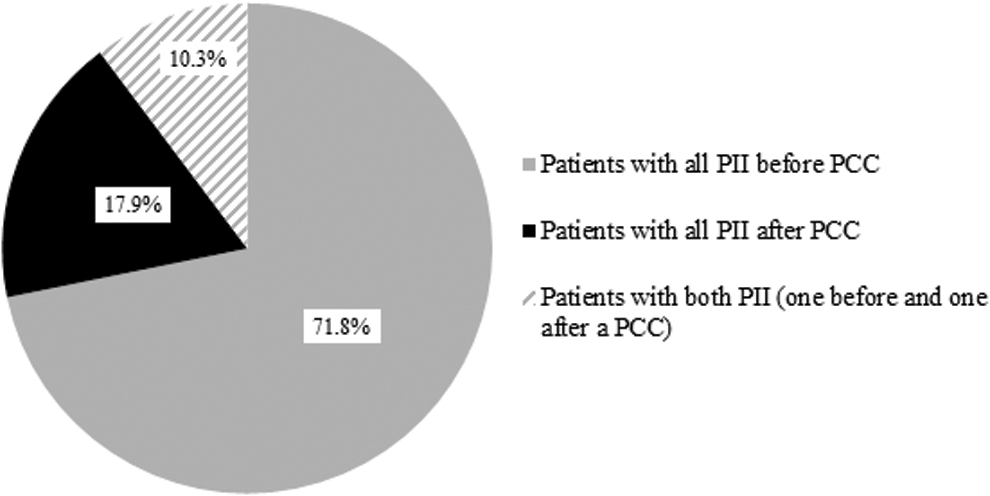
Patient distribution based on potentially inappropriate intervention timing in the PCC group.
We also found that PCC patients had a significantly higher mechanical ventilation requirement, whether it was an endotracheal intubation or TS, as well as a higher frequency of TS recommendations from a consulting attending, than MC patients (Table 2). The PCC compared with MC group also had a statistically higher assisted feeding requirement, whether via a feeding tube or a PEG, as well as a higher frequency of recommendations for PEG placement (Table 2).
Patients with Potentially Inappropriate Interventions in Palliative Care Consultation and Match-Controlled Groups
Denotes a statistically significant difference.
PEG, percutaneous endoscopic gastrostomy; TS, tracheostomy.
The DNR order analysis in patients with PII is presented in Table 3. In the PCC group, the majority of DNR orders were signed in-hospital. In four PCC patients, a PII was done despite the presence of a DNR, compared with two patients in the MC group.
Do-Not-Resuscitate Presence in Patients with Potentially Inappropriate Interventions in Palliative Care Consultation and Match-Controlled Groups
Denotes a statistically significant difference.
PII, potentially inappropriate intervention.
Discussion
Palliative specialists are becoming more engaged in the care of severely injured patients, however, there are known challenges to the implementation of PC in surgical or trauma settings related to a traditionally aggressive management approach. 12
Current consensus is that palliative medicine specialists are significantly more likely to be consulted for more injured adults, especially those who are elderly, indicating that PC is utilized more as a hospice service rather than a complementary service to trauma standard of care. 6
While the number of PCC has been steadily increasing in the past few years, from 1% of elderly trauma patients receiving them in 2007 to almost 5% in 2011, the reported numbers remain low. 1 In our study, the 4.3% rate of PCC in trauma patients was similarly low. The estimations from one study point out that 15.8% of ICU trauma admissions meet the criteria for a PCC. 3 Our 89.4% admission rate to the ICU in the PCC group is high, compared with the available literature of around 10% of ICU admissions in PCC patients. 20 These disparities in ICU admissions between the literature data and our findings can be attributed to high ISS, high rates of TBI, and accordingly lower GCS in both of our trauma patient groups. The high rate of TBI (68.5%) in our PCC population is in agreement with previously published TBI rates of 65.8%–73.4% in trauma PCC patients. 21
Our institutions use a consultative model of PC to determine if a patient is a candidate for a PCC. A special screening form that compiles a set of triggers is reviewed by a trauma surgeon, and a final decision to request a PCC is ultimately based on the attending surgeon's opinion. Therefore, the rate and timing of PCC depend on the patient's comorbidities, injuries, and the surgeon's evaluation.
In our study, time to PCC was 5.3 days, which is higher than the previously reported time to PCC of 2.9 days at another level 1 trauma center. 6 PCC patients were significantly older, and more often white race than MC patients, which is in line with research from multiple institutions, showing older age and white race as factors associated with a PCC in patients with severe TBI and as factors in end-of-life and PC decisions in trauma patients.2,22,23
Finally, in the PCC group, 87.7% of patients were discharged to hospice, with a total mortality of 90.7% within six months of discharge, and low in-hospital mortality of <5.0%. Compared with a study by Rivet et al. that showed tardy PCC implementation resulting in half of their population expiring in ICU or step down units, the high rate of hospice discharge in our PCC group demonstrates the benefits of timely PCC at our two institutions. 24 Our reported mortality rates in the PCC group are higher than the mortality rates of 31.3% and 16.2% in PCC nongeriatric and geriatric trauma patients available from other studies, however, our data also include mortality six months postdischarge. 21 Hwang et al. associated PC with decreased use of nonbeneficial life support and lower intensity of care. 23 Our high rate of discharge to hospice care also supports the benefits of PCC and a shift from nonbeneficial, high-intensity care in patients with a poor prognosis.
PCCs and Potentially Inappropriate Interventions
Additional analysis was done regarding the rates and timing of PII, as it was previously shown that PC consultations may significantly reduce mechanical ventilation and artificial nutrition in medical ICU patients. 25 Overall, <10.0% of our patients in both the PCC and MC groups had a PII, which is similar to the rate of 10.0% of trauma patients with PII described previously. 6 Although the total number of patients who received a PII was similar in both groups, it is important to notice that there was a reduction of PII after a PCC (Fig. 2). This reduction in PII, following a PCC, was further confirmed by the analysis of covariance, accounting for confounding variables, which were found to be statistically significantly different between the PCC and MC groups.
In the few cases where a PII followed a PCC, it was done at the request of the patient's family. Moreover, when we looked at the reasons for PII placement in PCC patients, 62.4% of them were placed based on family request, and against the patient's clinical condition. Published data indicate that the majority of patients and family members tend to be in agreement with the attending physicians' opinion on potentially excessive treatment and ICU interventions in cases of severely injured patients with a poor outlook, and this is reflected in our <10.0% rate of PII in both groups.26,27
Between 80% and 90% of physicians in one study reported that they would not want long-term mechanical ventilation if their own chances of recovery and survival outside of an ICU were slim, especially in cases with severe brain damage. 26 When we analyzed the timing of PII from admission and if indeed the interventions were inappropriate, we found that 92.4% of PCC patients with PII expired from their injuries, and that <50% of all PII were placed within the first week from admission.
In the PCC group, 60.4% of patients required mechanical ventilation during their hospital stay. The majority of this group had an endotracheal intubation, while only 5.8% had TS. In the MC group, 18.1% required mechanical ventilation, with 4.4% receiving TS (Table 2). The rates of TS in both our groups are low compared with the rates of 10.0%–24.7% found in other trauma populations.23,28,29 Only one study, by Toevs and Philp, on nongeriatric and geriatric trauma patients reported a TS rate of 2.9% and 1.9%. 21 The fact that TS constitutes a small portion of all mechanical ventilations is in line with other research.29,30
To further understand if a PCC had an impact on the rate of TS, we extracted TS recommendation data from the consultation reports. It is important to emphasize that the rate of TS placed to TS recommended was significantly twofold lower in the PCC than in the MC group. Holloway and Quill also noted a significant decrease in the number of TS and an increase of withdrawal of mechanical ventilation after PCC. 31 These data support a trend of reduction of PII after PCC in severely injured patients who may not benefit from such interventions. In the study by Toevs and Philp, on patients with head trauma, PCC were frequently done before TS, however, still a high 34.4% got a TS, and ultimately 13.6% expired in-hospital. 21 In another one-year retrospective study of 113,653 adult patients who underwent TS in 2006, a 19.2% in-hospital mortality was reported. 14 Such high mortality rates and poor outlook support and justify the need for increase of PCC in severely injured trauma patients before TS placement.
The requirement for assisted feeding was lower than for mechanical ventilation in both the PCC and MC groups in our study with 14.1% and 6.7% accordingly (Table 2). As in the case of TS, we calculated the rate of PEG placed to PEG recommended, and it was again significantly lower in the PCC than in the MC group. Our rates of PEG placement of 6.7% in PCC and 3.7% in MC are similar to those of 8.0% reported by others. 23
Our DNR analysis within PII patients revealed that PCC patients had a significantly higher (by 60.0%) rate of signed DNR orders than MC patients (p = 0.002). Previous studies showed that following a DNR signature, the use of advanced antibiotics, chest radiography, transfusion, surgical procedures, duration of mechanical ventilation, and TS rates significantly decreased.32,33 Within our PCC group, 4 (10.2%) of all patients who received a PII signed a DNR order before undergoing the procedure. In these cases, the decision to perform a PII, after a PCC and with a DNR order in place, was made at the family's request. In 26 MC patients who had a PII, 2 (7.7%) had a signed DNR order before the placement of a PII, and as in the PCC group, the PII was done at the family's request.
Overall, in our study, the amount of PII was reduced following a PCC; moreover, almost 50.0% of PCC patients who had a PII also had a DNR order. Early administration of PCC in severely injured patients is recommended and may aid in communicating the goals of care, as well as reduce the number of PII. Furthermore, since most of the DNR orders are signed in-hospital, a PCC should accompany the DNR discussion in severely injured patients, before the initiation of aggressive treatment that incorporates PII. It is also recommended that rather than increasing the rate of PCC, implementation of an integrated palliative care model might be more beneficial for severely injured patients. 34
Limitations
The retrospective nature of this study brings up a restriction in prerecorded data available for extraction from patient's charts. Data were extracted from only two level 1 trauma centers, which results in a relatively limited sample size. Also, the two institutions admit severely injured patients with high rates of TBI, and the demographics of our patient population are skewed toward geriatrics. By design, our study focused on only one aspect of palliative care, namely on the withdrawal of curative treatment and PII. Analyzed data included prerecorded notes and definitions, before the multisociety recommendations regarding PII. 19 The results reflect the rates of PCC based on a consultative model of PC and may differ from institutions that use an integrated model of PC, which tends to be more comprehensive and have more established guidelines. Patients who did not receive PCC may have received some elements of integrated palliative care.
Conclusions
PCC reduced the amount of PII in severely injured trauma patients by a factor of two. Due to the fact that the majority of PII in PCC patients occurred before PCC, we recommend a consistent and expedited administration of PCC. Early PCC can reduce the number of PII in a patient and save the patient from pain and financial burden. Furthermore, to streamline the goals of care, a PCC should supplement or precede a DNR discussion.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
Data included in this article were partially presented at the American Geriatrics Society Annual Scientific Meeting in May 2018.