
Abstract
Discussing difficult and personal topics is not new to those practicing palliative care. Specialty-level consultation is often sought to facilitate complex and uncomfortable conversations on death and dying. Palliative care (PC) providers focus on patient and family needs through the lens of whole-person care. Sexuality is an important component of every person's identity, yet providers often avoid this topic. Avoiding conversations about sexuality is especially strong when the patient has a serious illness. PC providers are recognized communication experts, although current curricula offer little training on how to incorporate discussions regarding this important aspect of personhood. Using case discussions, we offer strategies for examining sexuality and incorporating sex-positive interventions into practice. By highlighting how sexuality and PC intersect, we hope to foster a community of interdisciplinary PC providers who practice what we have termed sex-positive palliative care.
Introduction
Palliative care (PC) clinicians discuss culturally taboo topics, such as death and dying, with skill and ease. In her seminal piece, On Death and Dying, Dr. Kübler-Ross emphasized that health care professionals willing to embrace the awkward by initiating discussions relating to death are more likely to come across patients willing to do the same. 1 This sentiment applies for matters related to sexuality. PC professionals often overlook sexuality as an important aspect of life for those with serious illnesses.2–5 Failure to embrace and validate the sexuality of people with serious illness hinders recognition of their holistic human experience.6–8
Humans are complex beings with varied definitions of sexuality. Discussing this subject requires shared definitions of terms. Sex positivity embraces sexuality as a natural part of life that manifests differently for each person. 9 Those who are sex positive have a nonjudgmental approach to consensual sexual behaviors. PC professionals are often death positive; they accept death as a natural part of life, while acknowledging the experience of death is different for every individual. 10 See Table 1 for all expanded definitions.
Definitions
SPPC, sex-positive palliative care; PC, palliative care; LGBTQ, lesbian, gay, bisexual, transgender, and queer.
Practitioners who embrace both sex and death positivity strive to center that which is most important to the individual. To achieve this, PC professionals can make comfortable the uncomfortable and open the door for patients to share their preferences regarding both their sexuality and end-of-life journeys. PC professionals then can meet the individual where they are, better understand their priorities, center the patient's right to self-determination, and thus fully embrace the individual's chosen path regarding these two significant aspects of life.
Sex-positive practice affirms one's existence as a complex sexual being. In this article, we introduce the concept of sex-positive palliative care (SPPC): the acknowledgment that sexuality is a natural part of every life, including individuals coping with a serious illness. Holistic and sex-positive PC require discussions of sexuality during initial assessments, goals of care conversations, symptom management consultations, and psychosocial support visits.
The United States' cultural coital imperative (Table 1), narrowly defining sexuality in terms of penile-vaginal intercourse, contributes to discomfort discussing sexuality with seriously ill patients.11–13 This leads to invalidation of diverse sexual lives regarding sexual orientation, gender identity (Table 1), body diversity, disability, and sexual preference, and for those with serious illnesses. Health care professionals providing holistic and inclusive care can adopt expanded definitions of sexuality and find ways to incorporate this concept into clinical practice.
Dr. Dennis Dailey's Circles of Sexuality model (Fig. 1), introduced in 1981, provides a comprehensive understanding of sexuality. 14 This is a useful tool to teach both those with serious illnesses and those caring for them about sexuality and how it is impacted by disease progression.
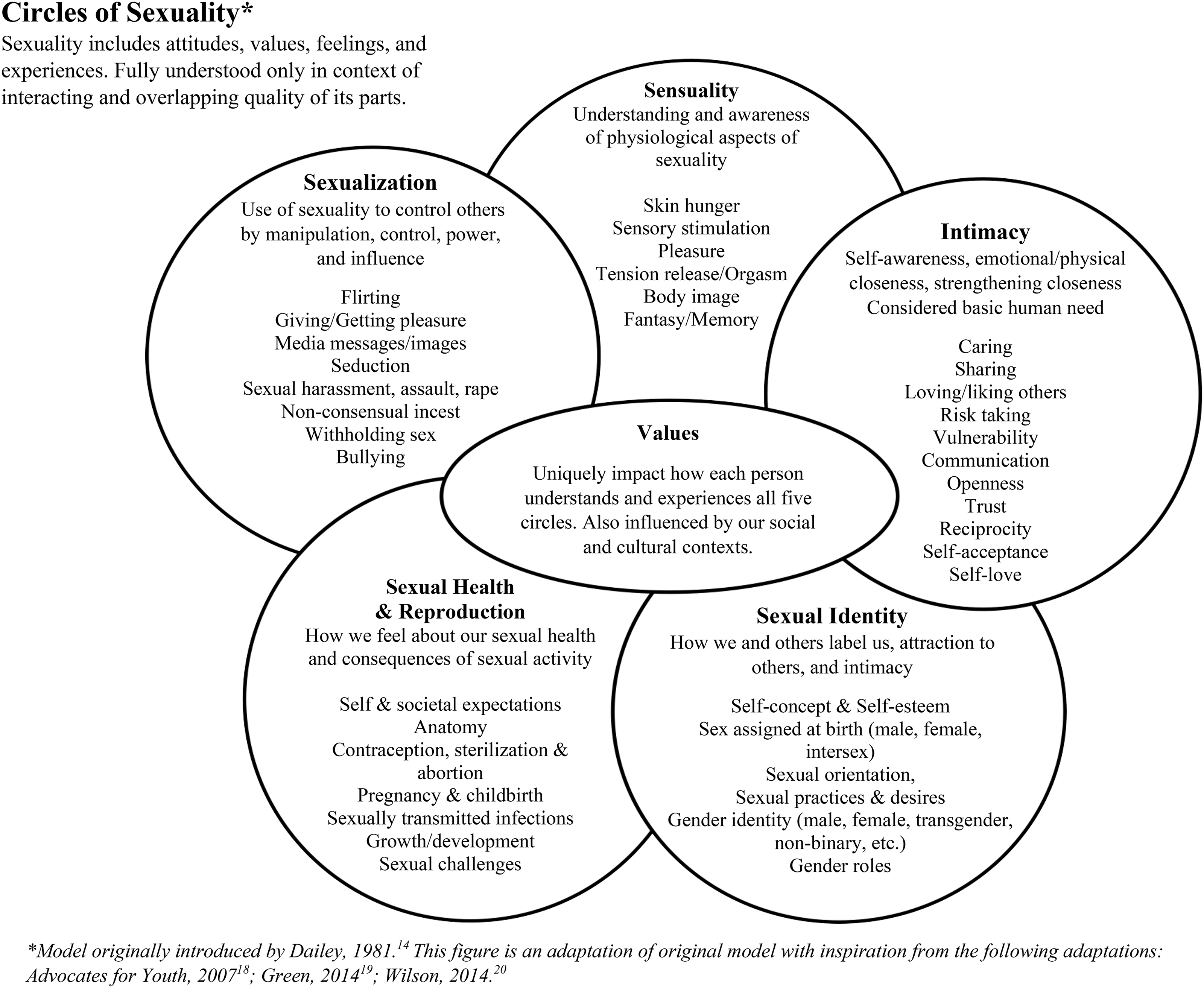
Circles of sexuality model.
The circles of sexuality
Dr. Dailey espouses that sexuality includes attitudes, values, feelings, behaviors, and experiences, all of which are influenced by social and cultural norms. He outlined five overlapping circles of sexuality: sensuality, intimacy, sexual identity, sexual health and reproduction, and sexualization. 14
Sensuality circle
Sensuality includes how we feel about our bodies, enjoy our bodies and the bodies of others, and feel and experience pleasure. A key concept for PC professionals to understand is skin hunger, defined here as the extent to which one prefers to give and receive touch.14,15 Skin hunger is an ever-evolving preference impacted by age, relationship context, culture, health, illness, and treatments.
Intimacy circle
Intrapersonal intimacy is one's degree of self-awareness, self-acceptance, and self-love. Interpersonal intimacy is the experience of being emotionally and physically close with others and how that closeness is strengthened. Communication involving intimacy is often neglected as part of formal sexuality education, leaving many individuals uncomfortable conveying sexual wants, needs, and desires. This becomes increasingly difficult for those with serious illness, who may feel body image insecurity or guilt for not being able to fulfill their roles as partner, lover, spouse, parent, and so on.
PC professionals are in a unique position to utilize preexisting skills in talking about death and dying to model how to talk about sexuality. Simply asking, “How has your illness impacted your sexuality?” displays that the PC professional is willing to engage in conversation. This question also opens the door for the individual with serious illness to talk about their sexuality if they wish.
Sexual identity circle
Sexual identity refers to the ways we label ourselves as sexual beings. It is influenced by others placing labels upon us and shaped by cultural and historical contexts. Sexual identity includes how we describe our sexual and romantic attractions, and how these attractions translate into sexual behaviors. Understanding patient's identities across gender and sexuality is key to effective goals of care discussions. This enables PC professionals to understand the patient's family of origin and family of choice (Table 1), thus recognizing who the patient may want in the room during medical discussions. This is also key to understanding an individual's priorities as illness progresses. For example, understanding the importance of one's affirming gender identity helps us to understand why a transgender (Table 1) individual may prioritize continuing hormone therapy even if it risks shortening their lifespan.
Sexual health and reproduction circle
Often medicalized, sexual health and reproduction are defined in the context of our individual experiences (self-expectations) and our societal settings (external expectations). Although formal education focuses the most on this area of sexuality, many people have limited knowledge about their own bodies, anatomy, and what physically occurs during sexual experiences. Understanding our sexual health can be more difficult as our bodies change due to disease progression and medical treatments. Sexual health education is often heteronormative 17 (Table 1) and limited to contraceptive methods and family planning, thereby perpetuating a noninclusive, pleasure-aversive view of sexuality.
Sexualization circle
This circle is often referred to as the shadow of sexuality and includes manipulation, control, power, and influence. These behaviors exist on a spectrum, the impact of which depends upon how the actions are received. For example, while an individual may feel as though their flirting is harmless, if the recipient feels negatively about the advance, then the behavior may be perceived as harassment.
For patients, past sexual trauma can increase vulnerability and the possibility of retraumatization impacting current medical care and decision making. In addition, flirting and seduction may become more challenging for individuals with serious illness as spontaneity is often lost due to having to plan sexual activities around medical appointments, disease-directed therapies, side effects/symptoms, and medications.
Case Descriptions
We present three PC cases in which sexuality was identified as a priority for the patient and/or their family. We then discuss how PC professionals can overcome potential discomfort in validating and exploring this essential part of personhood. Drawing parallels between two of the United States' most culturally taboo subjects, sex and death, we identify ways PC professionals can apply skills they have learned talking about death and dying to talking about sex and sexuality.
Patrick
Patrick is a 23-year-old heterosexual cisgender (Table 1) man with metastatic Ewing sarcoma. Originally diagnosed during his high school graduation week, Patrick is well known to the PC service. Patrick consistently verbalized a desire to prolong his life, become a father, and maintain independence. Despite multiple cancer-directed therapies, he is admitted with worsening spinal metastases and cord compression requiring discussion of a high-risk, emergent spinal surgery.
Patrick is overwhelmed. An urgent family meeting with him, his family, the neurosurgeon, PC nurse practitioner, and PC social worker takes place to explore his options. The discussion focuses on the benefits and risks of surgical intervention with emphasis placed on providing him the best chance to walk again. However, Patrick's goal becomes clear when he proclaims, “I would like the chance to feel my penis again!”
Taylor
Taylor is a 39-year-old heterosexual cisgender woman diagnosed with recurrent colorectal cancer during pregnancy. She has undergone several rounds of chemotherapy and surgical intervention, including ostomy placement. Recent imaging reveals progressive disease. Taylor is regularly seen by the PC team for pain and symptom management. Despite appearing visibly weaker with each admission, she always pushes for an expeditious discharge home to be with her family.
Taylor verbalizes two main fears: leaving her 1-year-old son without a mother and not being able to have an intimate relationship with her husband. Her reluctance to attempt intimate contact with her husband is due to pain, constant pressure from the tumor pressing on her bladder and pelvic floor, and intense anxiety that her ostomy would interfere with sexual encounters. Recognizing time is short, she conveys feeling immense guilt in avoiding intimacy with her husband. She asks the PC physician and PC social worker, “How can I be intimate with my husband when I am in so much pain?”
Evan
Evan is a 51-year-old homosexual (Table 1) cisgender man whose 56-year-old cisgender male partner, David, is dying from metastatic Kaposi sarcoma. The first PC visit focused on symptom management, David and Evan's experience with cancer, and sharing prognostic information. David remained quiet and somewhat withdrawn, while Evan described their experience living through the 1980's acquired immunodeficiency syndrome epidemic. Evan spoke with sadness about the many young friends they helped through end of life.
During the second PC visit, Evan discusses a desire to seek sexual intimacy outside of his relationship with David. He shares that he and David have not had sex in many years. Evan also shares that although he loves and is devoted to David, he is looking forward to dating again after David dies. Evan asks, “Is that okay?”
Discussion
Understanding the circles of sexuality can aid PC professionals in effectively validating sexuality-related concerns expressed by patients and their families. When PC professionals understand which aspects of sexuality are impacted by illness and disease-directed therapies, it facilitates empathizing with the individual. In this section, we identify some basic SPPC interventions to better support the patient and/or family.
SPPC interventions
Patrick
It is clear through Patrick's proclamation his priorities were not being addressed. Validation and exploration are key to supporting Patrick. Immediate acknowledgment and normalization of his declaration allow further exploration. During the meeting, the PC team validates Patrick by asking the neurosurgeon, “Will this surgery give him the chance to feel his penis again?” The neurosurgeon clarifies that surgical intervention will also provide this potential. Patrick is then able to make an informed decision based upon his priorities. To better understand Patrick's sexuality-related distress, we consider the intimacy, sensuality, sexual identity, and sexual health and reproduction circles.
Multiple aspects of Patrick's sexuality have been impacted by his serious illness. PC clinicians encouraged Patrick to further explore the impact of serious illness on his sexuality through reflection: “I've heard you say that worsening cancer has impacted your penis, made masturbation less pleasurable, and has you concerned about your ability to have sexual intercourse in the future. I can understand why this would be concerning. Would you like to talk about this more?”
Patrick eventually shared his fears of the potentially permanent loss of self-pleasure through masturbation; an activity that brings comfort, pleasure, and normalcy to his otherwise chaotic, highly medicalized life. Validating Patrick's sexual desire demonstrates the PC provider's acknowledgment of Patrick's whole personhood. It also helps to validate another significant loss in Patrick's life: the loss of his current and future sexual self. This is particularly traumatic for Patrick as he has yet to experience his sexual debut with a woman and he is in the process of anticipatorily grieving this as a permanent loss.
Patrick's heteronormative self-concept of being a man involves the ability to engage in penile-vaginal intercourse with a woman for both physical pleasure and procreation. From this, the loss of manhood and fatherhood can also be acknowledged. Along with exploration and validation, we helped reframe Patrick's hope by discussing other means of physical intimacy, self-pleasure, legacy, and family planning within the context of his illness.
Taylor
Taylor is planning for the end of her life and exhibits guilt regarding her inability to maintain physical intimacy with her husband and inability to physically hold her child. Taylor is trying to balance her symptom management needs with her desire to maintain physical intimacy. She is grieving the loss of her self-concept as a woman, wife, and mother. To better understand Taylor's sexuality-related distress, we consider the sexual identity, intimacy, and sensuality circles.
PC professionals validate psychosocial distress at the end of life and this can be extended to include sexuality-related fears and losses. PC intervention for Taylor included specifically and deliberately allowing space to share her desire to be physically intimate with her husband before she dies. It was imperative to validate her feelings and allow her to talk about the significant loss of her sexual self-concept and intimacy with her husband.
One approach to dealing with an individual whose fears are based in grief and guilt can include discussing alternatives. We worked with Taylor to brainstorm alternative intimate activities, such as cuddling and light massage, timing of intimate behaviors, positions, and use of medication before physical closeness. These interventions helped Taylor cope and allowed her to experience some degree of intimacy before her death.
Evan
Evan has been grieving the loss of various aspects of his relationship throughout David's long illness. Evan is devoted to David, committed to their monogamous relationship, and wants to ensure David receives the best medical care. Nevertheless, Evan's self-concept of being a man and his desire to seek sexual pleasure have been impacted by David's disease progression. Evan expresses feeling guilty for his desire to be with others and is looking for reassurance that this does not make him a “bad” husband or caregiver. To better understand Evan's sexuality-related distress, we consider the sexual identity, intimacy, and sensuality circles.
PC professionals are called upon to validate experiences regarding pain and suffering at end of life. However, life does not stop for partners, families, and friends who are struggling with various forms of loss. Utilizing Dailey's Circles of Sexuality to comprehend the negative impact David's illness has had on Evan's sexuality allows for validation of Evan's losses and fears and normalizes his reaction.
Without judgment, we purposefully provided Evan with space to openly discuss his loss of intimacy and desire to build new romantic and sexual relationships. We validated and normalized Evan's past and present grief, the loss of partner intimacy, and the anticipation of engaging in sexual relationships. We provided a space for Evan to grieve fully, while looking forward to life after David's death. Finally, we encouraged Evan to make plans to become more social in the local gay community, which would enable Evan to expand his dwindling chosen family, a step that may become invaluable as he grieves the loss of his current long-term partner.
Conclusion
Sexuality is a key component in conversations regarding goals of care, symptom management, and quality of life. One does not need to be an expert in sexuality to validate someone's continued and evolving existence as a sexual being. All PC professionals can be prepared to discuss these broad concepts of holistic sexuality. The Circles of Sexuality is one tool to help PC professionals understand sexuality-related distress and model open communication around person-centered, holistic sexuality. To incorporate SPCC into your practice, try adding just one door-opening question to your PC assessment: “How has serious illness impacted your sexuality?”
Footnotes
Acknowledgment
The authors thank Dr. Dennis M. Dailey for granting permission to utilize his Circles of Sexuality model.
Funding Information
No funding was received to support the development of this article.
Author Disclosure Statement
No competing financial interests exist.