
Abstract
Background:
The growing trend in providing palliative care and end-of-life services has dictated that healthcare providers be adequately trained to care for people with serious illnesses, such as multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD). These progressive inflammatory diseases lead to physical, cognitive and emotional deficits and have exceptionally high care demands leading to high levels of distress. Because the impact on the delivery of patient care is influenced by the specialists' knowledge and comfort discussing end-of-life issues, it is concerning that interventions to address unmet palliative care needs in MS and NMOSD rarely include clinician-patient dyads.
Objectives:
To evaluate the neurology clinicians' knowledge and level of comfort discussing palliative care and end-of-life issues.
Design:
A cross sectional survey was conducted. The statistical analyses included frequencies, chi square statistics and logistic regression.
Setting/Subjects:
414 MS specialists answered an online anonymous survey. The survey was conducted using email distributions to MS professionals through the Consortium of MS Centers (CMSC), the International Organization of MS Nurses (IOMSN) and the UK Nurses' MS Organization.
Measurement:
The “End of Life Professional Caregiver Survey” (EPCS) was used to collect data.
Results:
The majority of the multidisciplinary professionals were female, white, nurses, and older than 40 years of age. 41% had their own advance directives and 57.6% had end-of-life basic training. There was a statistically significant association between end-of-life training or having advance directives and comfort discussing palliative care and end of life issues. Professionals that had basic end-of-life training and their own advance directives had higher comfort discussing code status, specific end-of-life issues, and advance directive planning.
Conclusions:
Basic end-of-life training and having advance directives among MS professionals were associated with better communication of palliative care and end-of-life domains with patients and their care partners.
Introduction
Neurological professionals in multiple sclerosis (MS) centers provide care for patients with neuroinflammatory demyelinating and neurodegenerative chronic illnesses, such as MS and neuromyelitis optica spectrum disorder (NMOSD). These diseases are the most common neuroinflammatory diseases of the central nervous system. MS prevalence is approximately one million in the United States and three million worldwide with a female:male ratio of 3:1.1,2 NMOSD is considered a rare disease that is overrepresented in non-European populations worldwide. A national NMOSD clinical consortium was established and reported 187 patients with a female:male ratio of 6.5:1.3,4 These are unpredictable autoimmune diseases characterized by early onset demyelination and axonal loss leading to irreversible neurological impairment and loss of function.3–7 These illnesses may lead to cognitive, emotional, and physical symptoms with exceptionally high care demands, leading to high levels of psychological and physiological distress in patients and their care partners.8–12
Although these neuroinflammatory illnesses are relapsing and progressive diseases, patients do not often assign a health care proxy or make any decisions related to their palliative care (PC) and end-of-life (EOL) wishes. 13 A primary source of patients' and care partners' psychological distress is the high incidence of unmet PC needs.14–16 Furthermore, clinicians are frequently uncomfortable and lack communication skills for PC and EOL discussions, especially with their young patients. Overall, the timing of introducing PC to patients with these neurological diseases is controversial. 17 PC assessment is being performed in Europe soon after the diagnosis of MS and, if necessary, a referral to specialized PC service is made. 18 If similar approaches are not developed in the United States, individual patients will continue to depend too much on professionals recognizing (or not) their unmet PC needs. 18
A few studies have discussed the integration of palliative and EOL care in patients with neurological diseases.16,19–21 However, most of the MS studies on PC and EOL discussions between clinicians and their patients involve patients who have severe forms of these neurological diseases and during later phases of the illness.17,22–27 Neurology and PC experts believe that introducing PC early in the disease would improve care in patients with neurological diseases; however, they identified a number of barriers, such as limited resources and clinicians' awareness. 28 Evidence showing an association between early integration of PC and improved quality of life, better symptom management, and increased care partners' satisfaction has mainly been reported in patients with cancer.28–30 The presence of additional confounding factors such as cognitive impairment and mood disorders in patients with MS may present unique challenges regarding PC and EOL issues, particularly in relation to a patient's ability to consent to treatment or to request that a treatment be stopped. While clinicians working at the intersection of neurology and oncology are well positioned to understand these challenges, neurologists and MS experts receive little formal PC training.28,29
With the rapid growth in PC across the United States, there are opportunities to improve the PC knowledge of neurology trainees and the delivery of PC to patients with neurologic disease.28–31 They highlight how PC conversations are frequently triggered by acute events resulting in the loss of a patient's capacity, thereby requiring surrogate communication and decision making. In addition, prognostic uncertainty and unfamiliarity with disease trajectories in neurology pose a challenge for palliative clinicians. Neurology experts point to the lack of PC training and education, resulting in minimal communication and referral to PC.32–36 In view of the limited training of neurology professionals in PC and EOL issues, the purpose of this study was to evaluate neurological professionals' perceived level of comfort and competence discussing these issues. The four aims of the study were to (1) investigate the association between neurological professionals' basic EOL training and their knowledge and comfort discussing PC and EOL issues; (2) investigate the association between professionals having their own advance directives and their knowledge and comfort discussing PC and EOL issues; (3) evaluate the association between professionals' personal resources (personal knowledge and experience) and basic EOL training, work resources, education, and years of experience; and (4) evaluate the odds of having basic EOL training or having advance directives and comfort discussing early PC/EOL issues with patients with MS.
Methodology
A cross-sectional anonymous survey was conducted using email distributions to 8000 MS professionals through the Consortium of MS Centers (CMSC), the International Organization of MS Nurses (IOMSN), and the UK Nurses' MS Organization. The professionals in these organizations care for patients with MS, NMOSD, and other neuroinflammatory diseases. They were asked to complete a demographic form and the EOL Professional Caregiver Survey (EPCS), 37 distributed twice to these professionals within a 12-week period through an online survey. The survey was designed and administered through the survey hero software program/application.
Institutional Review Board (IRB) approval was received through the Mount Sinai Health System, the Icahn School of Medicine in New York City. A research consent form following a template of the Mount Sinai IRB was attached to the enhanced EPCS. The consent described the voluntary nature of the survey. Participation in the survey after reading the information sheet constituted evidence of consent.
The demographic form included age, sex, race/ethnicity, profession, country, education level, years of experience with MS, whether the participant had her/his advance directives (health care proxy, living will or physician's/medical order for life-sustaining treatment), resources/training at work, and basic EOL training (basic knowledge and awareness of EOL concepts through workplace training and workshops). The EPCS, used in multiple chronic illness studies, contains 28 questions and covers all eight domains of the PC guidelines and is consistent with the PC Competence theoretical framework 38 : scientific and clinical knowledge/technical skills; communication/interpersonal skills with patients, family members, and other clinicians; spiritual and cultural issues; ethical, professional, and legal principles; organizational skills; and attitudes, values, and feelings of health care professionals. 38 The EPCS is psychometrically valid for use as a single (nondiscipline specific) scale to evaluate the educational needs of professionals. 37 In addition, correlations among the factors of the EPCS and the overall EPCS ranged from 0.80 to 0.92 (p = 0.01). 37 In the current study, the EPCS was enhanced by adding two questions (questions 29 and 30) created by the authors to address early discussion of EOL issues and specific potential future interventions with patients with MS and their care partners after their diagnosis. Each of the 30 questions had 5 answer options regarding professionals' knowledge/comfort: Not at all, A little bit, Somewhat, Quite a bit, and Very much.
Data analyses
The data were entered into SPSS IBM version 23. The statistical analyses included frequencies, chi square statistics, and logistic regression. The chi-square analyses were performed to investigate the association between each of two dichotomous variables whose data were obtained in the demographic form (having EOL basic training and having their own advance directives) and the specific PC/EOL-related questions/statements from the enhanced EPCS. For these analyses, the five answer options of the enhanced EPCS were collapsed into two levels of knowledge/comfort; not at all, a little bit, and somewhat versus quite a bit and very much. The analyses included determination of statistical significance of the chi-square statistics (p < 0.05) and effect size, as measured by Cramer's V. 39 Cramer's V is a statistic used to measure the strength of association between two nominal variables, and it takes values from 0 (weakest association) to 1 (strongest association). Weak association is a Cramer's V value of 0.1 or lower, moderate association is between 0.1 and 0.3 inclusive of 0.3, and strong association is a value higher than 0.3. 39 Two separate binomial logistic regression analyses were performed to predict the odds of having basic EOL training and having advance directives. Controlling for demographics, predictors in each of the logistic regressions were feeling comfortable discussing EOL issues and advance directives early in the MS disease course (question 29) and comfort discussing specific issues such as gastric and breathing tubes early in the MS disease course (question 30).
Results
The survey was completed by 414 of the 8000 (5%) MS professionals to whom it was distributed online. Characteristics of survey respondents are given in Table 1. The majority of the professionals were female, white, nurses, and older than 40 years (Table 1). Approximately 50% of the professionals had 21–40 years of experience and 66.5% were from the U.S. Professionals from the United States versus all other countries did not show a statistically significant difference related to basic EOL training [X 2 (1) = 0.164, p = 0.685], but having advance directives was significantly higher among professionals in the United States versus other countries [X 2 (1) = 17.899, p < 0.001] (Tables 2 and 3). Forty-one percent of the professionals had their own advance directives and 57.6% had EOL basic training in their medical or nursing education (Table 1). Missing data were excluded from the analysis because there were very few missing items (∼2%).
Characteristics of the Sample (n = 414)
EOL, end of life.
Association between Demographic Variables and Professionals Having Their Own Advance Directives
p < 0.05; **p < 0.01; ***p < 0.001.
Association between Demographic Variables and Professionals Having Basic End-of-Life Training
p < 0.05; **p < 0.01; ***p < 0.001.
There were statistically significant associations between professionals having their own advance directives and both grouped age and years of experience [X 2 (1) = 21.387, p < 0.001; X2(1) = 28.818, p = 0.001, respectively] (Table 2). Older professionals and those with more years of experience were more likely to have their own advance directives than those who were younger and those with fewer years of experience. In addition, there was a statistically significant association between professionals having their own advance directives and country of practice [X 2 (1) = 27.846, p = 0.001] (Table 2). Professionals who practiced in the United States were more likely to have their own advance directives than those from other countries. Moreover, there was a statistically significant association between EOL training and having their own advance directives (Fig. 1). Of the professionals who had EOL training, 64.8% had their own advance directives, while among professionals who did not have EOL training, only 35.2% had their own advance directives [X 2 (1) = 5.623, p = 0.018] (Fig. 1).

Association between basic end-of-life training and having own advance directives.
There was a highly statistically significant and strong association between having basic EOL training and the comfort of discussing code status (question 4) [X 2 (1) = 42.666, p < 0.001], and encouraging patients and families to complete advance care planning (question 12) [X 2 (1) = 36.493, p < 0.001] (Table 4). There was also a highly statistically significant and moderate association between having had basic EOL training and the comfort of discussing advance directives with patients with MS early in the disease process (Fig. 2) (question 29) [X 2 (1) = 49.146, p < 0.001], and discussing specific wishes of patients with MS, such as placing a gastric or a breathing tube (Fig. 3) (question 30) [X 2 (1) = 28.096, p < 0.001] (Table 3). In fact, those who had basic EOL training had a statistically significant higher comfort discussing all PC and EOL issues described in Table 3.
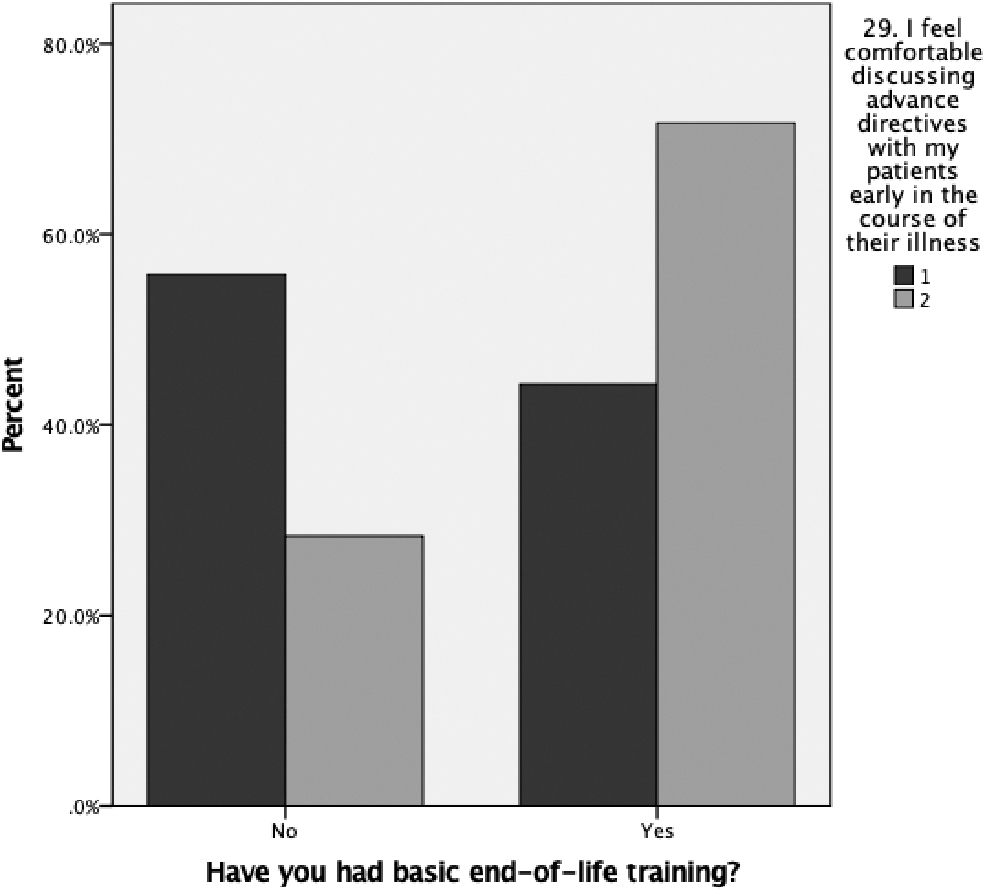
Comfort discussing advance directives with patients in early phases of MS. MS, multiple sclerosis. 1 = little comfort; 2 = very much.
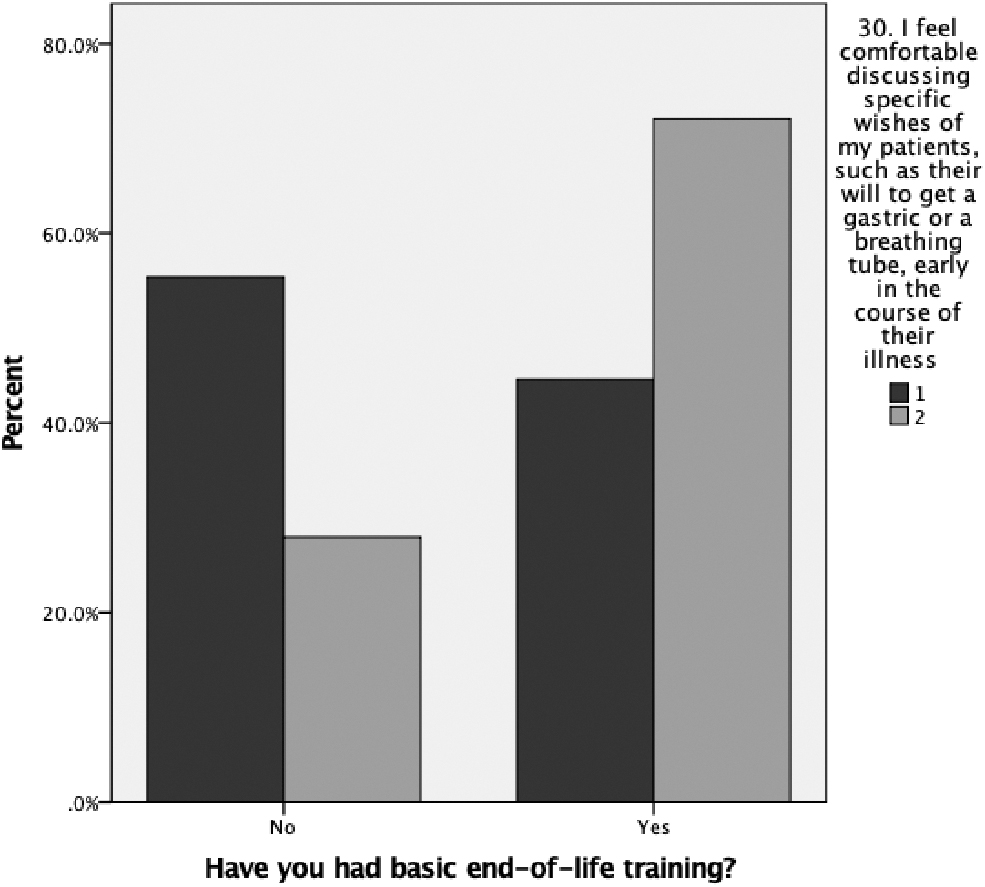
Comfort discussing specific wishes such as gastric and breathing tubes early in the course of the illness. 1 = little comfort; 2 = very much.
Association between Responding Quite a Bit/Very Much to End-of-Life Professional Caregiver Survey Questions and Having End-of-Life Basic Training
p < 0.05; **p < 0.01; ***p < 0.001.
There was a significant and moderate association between MS specialists having their own advance directives and being comfortable helping families to accept a poor prognosis (question 1) [X 2 (1) = 6.163, p = 0.021], setting goals (question 2) [X 2 (1) = 6.998, p = 0.032], and code status discussions (question 4) [X 2 (1) = 9.843, p = 0.003] (Table 5). Approximately 50% of professionals who had their own advance directives felt comfortable discussing and participating in PC and EOL discussions (Table 5). More than 50% of professionals who had their own advance directives felt comfortable and knowledgeable about being comfortable completing advance directives with patients and their care partners (question 12) [X 2 (1) = 33.052, p < 0.001], having early PC discussions with patients with MS and their care partners (question 29) [X 2 (1) = 31.330, p < 0.001], and specific discussions about gastric and breathing tubes (question 30) [X 2 (1) = 17.102, p < 0.001]. The association of these variables and others with professionals having their own advance directives was highly statistically significant and moderate (Table 5).
Association between Responding Quite a Bit/Very Much to End-of-Life Professional Caregiver Survey Questions and Having Their Own Advance Directives
p < 0.05; **p < 0.01; ***p < 0.001.
There was also a highly significant and moderate association between having basic EOL training and personal resources to meet individual needs [X 2 (1) = 12.769, p < 0.001], and a strong association between having personal resources and having work resources [X 2 (1) = 61.025, p < 0.001] (Table 6). Sixty-three percent of professionals who felt that they had personal resources, identified their workplace as a resource for PC issues (Table 6). However, there was no significant association between having personal resources and level of education when discussing EOL issues [X 2 (1) = 1.655, p = 0.647]. In addition, there was a highly statistically significant and strong association between having personal resources and years of experience as a neurological professional [X 2 (5) = 16.575, p < 0.001] (Table 6).
Association between Professionals' Personal Resources and Basic End-of-Life Training, Work Resources, Education, and Years of Experience
p < 0.01; ***p < 0.001.
Logistic regression results indicated that, controlling for demographic, the odds of professionals having basic EOL training were significantly lower for those professionals who did not feel comfortable discussing EOL issues early in the MS disease course (p = 0.009) (question 29) (Table 7). There was no statistical significance for the odds of having basic EOL training and comfort discussing specific issues such as gastric and breathing tubes early in the MS disease course (question 30) (Table 7) and no statistical significance for the odds of having advance directives and discussing EOL issues early in the MS disease course (Table 8).
Logistic Regression to Predict the Odds of Professionals Having Basic End-of-Life Training
Bold indicates statistically significant results (p < .01 or p < .05).
Logistic Regression to Predict the Odds of Professionals Having Their Own Advance Directives
Bold indicates statistically significant results (p < .01 or p < .05).
Discussion
Among 414 MS professionals from various disciplines, 57% of the respondents had received basic EOL training, and 41% had completed their own advance directives. Professionals who practiced in the United States were more likely to have their own advance directives than those from other countries. This study found that both EOL training and having advance directives were associated with increased knowledge and comfort with some aspects of EOL discussions with MS patients. Furthermore, comfort helping to resolve difficult family conflict and knowledge of nondrug therapies seem to benefit less from clinicians having their own advance directives, whereas the benefit of talking with patients and families about personal choice was higher. In addition, comfort addressing spiritual and religious aspects of care seem to benefit less from basic EOL training undertaken by respondents than encouraging patients and families to complete advance directives, which appears to yield higher benefit.
To our knowledge, advance directives and EOL issues have not been examined in research involving MS and NMOSD professionals. In the current study, 57.6% had basic EOL training, whereas 64.9% in the Scherer study and 62% in the Lazenby study had formal instruction in advance directives at their place of work.37,40 Additionally, the study by Lazenby et al. showed that having advance directives among 369 multidisciplinary professionals was significantly associated with higher scores on the EPCS instrument. In a recent systematic review, 41 there was concern over the type and quality of basic EOL training. Recently, there has been a proliferation of EOL care and communication skills training interventions. These include role play, group work, reflection and discussion, and the more traditional lectures and presentations. 41 This model would seem appropriate for MS and NMOSD centers, although the content would need to be adapted for the particular challenges and nuances of the neurology setting.
Our study found a statistically significant decreased odds of having basic EOL training among those who were less comfortable to discuss EOL and PC issues with patients with MS during the early phases of their illness. In addition, this study found a statistically significant association between basic EOL training or having advance directives and the comfort of discussing specific wishes with patients during earlier phases of the illness, and the comfort of discussing advance directives and code status. Early PC discussions were associated with improved quality of life in patients with metastatic nonsmall-cell lung cancer. 42 Unfortunately, the potential benefits of early PC discussions have not been evaluated in MS, and both MS patients and clinicians have expressed reservations regarding early PC discussions. 43 The fact that some of the respondents to our survey were comfortable initiating these early discussions further underscores the need for further research on PC/EOL in MS.
This study underscores the importance of MS professionals participating in EOL training and having advance directives, since both were associated with improved perceived comfort discussing EOL issues. However, having an advance directive is a highly personal choice driven by a number of factors, including personal experience, cultural perspectives, and values. In addition, there may be other beliefs and personality tendencies that make professionals both more likely to sign their own advance directives and more likely to better handle these crucial PC conversations and management activities. The study findings support the need for widespread education and training on EOL care for MS professionals and encouraging providers to have their own advance directives. Thus, it is a desirable goal to test the impact of low-cost, easily scalable standardized workplace educational and training workshops to MS providers and patients with MS.
Strengths and limitations of the study
The sample of neuroinflammatory experts was drawn from national and international MS organizations and physicians, and nurses/nurse practitioners were represented. The majority of the sample was older than 40 years and with many years of MS experience (21–40 years). Based on internal unpublished reports from CMSC and IOMSN, the demographic distribution of the survey responders appears reasonably consistent with the population of MS experts. Additionally, despite the small sample size, the strong correlation between having basic EOL training and comfort discussing PC/EOL care with patients is foreseeable and has strong face validity, reinforcing the value of such training for all neurologists. In addition, the use of the EPCS instrument, a valid and a reliable tool, is a strength of the study.
The design of this study (convenience sample) limits the generalizability of the results, and this limitation is amplified by the low response rate. Furthermore, there is a response selection bias in that the responders were skewed toward nurses making extrapolation to other professionals in the same field questionable. However, nurse practitioners and physicians are equally represented in this sample (62 and 53 participants, respectively). There may also be an additional sampling bias in that professionals who are interested or more confident in their provision of EOL care may have been more likely to respond to the survey, which may lead to skewed results. Furthermore, the lack of ethnic/racial diversity in the sample may have affected the survey results. Additionally, the study does not present information on the specific types of training that comprised “basic EOL training” and how varied levels/types of training may have affected the results.
Conclusions
Basic EOL training and having advance directives among MS professionals were associated with better communication of PC and EOL domains with patients and their care partners. This survey emphasizes the need and importance of EOL training and having advance directives. Future studies should include assessment surveys and PC educational programs to enhance communication between patient/professional dyads about PC and EOL domains.
Footnotes
Acknowledgments
The authors thank Dr. Shiela Strauss for her support, expertise, and assistance in writing this manuscript. They also thank all the MS experts who completed the survey.
Funding Information
No funding was received for this research.
Author Disclosure Statement
Aliza Ben-Zacharia, consultant, Biogen, Greenwich Biosciences, Genentech, and Novartis.
Francois Bethoux, consultant, GW Pharma, Helius Medical Technologies, MedRhythms, Genentech; speakers bureau, Biogen; contracted research, Adamas Pharmaceuticals; royalties, Qr8.
Angelo Volandes has a financial interest in ACP Decisions Nous, a non-profit organization developing advance care planning video decision support tools. His interests were reviewed and are managed by Massachusetts General Hospital and Partners HealthCare in accordance with their conflict of interest policies.