
Abstract
Background:
In the United States, the percentage of hospitals over 50 beds with palliative care programs has risen substantially from 7% of hospitals in 2001 to 72% in 2017. Yet the dynamic nature of program adoption and closure over time is not known.
Objective:
To examine the rate of palliative care program adoption and closure and associated hospital and geographic characteristics in a national sample of U.S. hospitals.
Design:
Adoption and closure rates were calculated for 3696 U.S. hospitals between 2009 and 2017. We used multivariable logistic regression models to examine the association between adoption and closure status and hospital, geographic, and community characteristics.
Setting/Subjects:
All nonfederal general medical and surgical, cancer, heart, and obstetric or gynecological hospitals, of all sizes, in the United States in operation in both 2009 and 2017.
Results:
By 2017, 34.9% (812/2327) of the hospitals without palliative care in 2009 had adopted palliative care programs, and 15.0% (205/1369) of the hospitals with programs had closed them. In multivariable models, hospitals in metropolitan areas, nonprofit and public hospitals (compared to for-profit hospitals), and those with residency training approval by the Accreditation Council for Graduate Medical Education were significantly more likely to adopt and significantly less likely to close palliative care programs during the study period.
Conclusions:
This study indicates that palliative care is not equitably adopted nor sustained by hospitals in the United States. Federal and state interventions may be required to ensure that high-quality care is available to our nation's sickest patients.
Introduction
Palliative care is specialized medical care for people living with a serious illness. 1 Provided by a specially trained team of doctors, nurses, and other specialists, palliative care teams focus on providing relief from the symptoms and stress of a serious illness. A growing body of literature shows that palliative care improves quality of life and reduces symptom distress, 2 health care utilization, and costs. 3
The availability of palliative care is essential to the millions of people living with serious illness, who are more likely to be hospitalized than the general population 4 and often receive low-value care that results in adverse emotional, psychological, financial, and health impacts. 5 Given projected growth in the number of older adults living with serious illness, 6 investment in palliative care is a quality imperative to meet patient and family needs.
U.S. hospital palliative care programs have grown from 7% of hospitals with 50 or more beds providing palliative care in 2001 to 72% in 2017. 7 This growth has occurred as a result of individual hospital or health system decisions and is not uniform across different regional and industry sectors. For example, cross-sectional studies find that for-profit hospitals, hospitals in the South, nonteaching hospitals, and smaller hospitals are those least likely to have palliative care programs.8–12
Data are lacking on the longitudinal growth patterns of hospital palliative care. In this study, we sought to supplement cross-sectional analyses7–12 on the availability of hospital palliative care with an understanding of longitudinal national trends. We used 2009–2017 data from the American Hospital Association (AHA), the National Palliative Care Registry™, Dartmouth Atlas of Care, U.S. Census Bureau, and the Centers for Medicare & Medicaid Services (CMS) to gain insight into the factors associated with palliative care program adoption and closure across hospitals nationwide.
Methods
Data sources and sample
We obtained information on hospital characteristics and services from the AHA Annual Survey Database™ for fiscal years 2009 and 2017. The AHA annual survey is distributed to 6500 hospitals and achieves an 80% response rate making it the most comprehensive and authoritative source of U.S. hospital data. Data on hospital characteristics are self-reported to the AHA annual survey and unusual changes in data over time are validated by the AHA. 13 For the ∼20% of hospitals that did not respond to the 2009 or 2017 AHA survey, we supplemented using their 2008 or 2016 AHA responses, respectively.
Hospitals were included in our sample if the majority of annual inpatient admissions were for general medical-surgical, obstetrics/gynecology, cancer, or cardiac care indications. We excluded rehabilitation hospitals, psychiatric hospitals, subacute and chronic care facilities, hospitals within institutions like prisons, and eye, ear, nose, and throat hospitals. We excluded hospitals owned by the federal government, hospitals located outside of the 50 states and the District of Columbia, and hospitals that did not exist in both 2009 and 2017. Hospitals of all sizes were included in the analyses.
Geographic-based data, including demographic and socioeconomic characteristics of the fee-for-service Medicare population, were obtained from the Geographic Variation Public Use File from the CMS and matched by hospital referral region (HRR). Data on Medicare and hospice reimbursement per enrollee and physician capacity were obtained from the Dartmouth Atlas of Care and matched by the hospital service area (HSA). 14 The AHA dataset incorporates geographic data, including census region and core-based statistical area from the U.S. Census Bureau.
Measures
Our two primary outcome measures were (1) palliative care program “adoption,” defined as a hospital that did not have a palliative care program in 2009, but did in 2017, and (2) palliative care program “closure,” defined as a hospital that had a palliative care program in 2009, but no longer had one in 2017. For both outcomes, the hospital must have remained in operation for the full study period.
In the AHA Annual Survey, hospitals self-identify if they have palliative care, defined as either
Palliative care: An organized program providing specialized medical care, drugs, or therapies for the management of acute or chronic pain and/or the control of symptoms administered by specially trained physicians and other clinicians; and supportive care services, such as counseling on advanced directives, spiritual care, and social services, to patients with advanced disease and their families.
Inpatient palliative care unit: An inpatient palliative care ward is a physically discreet, inpatient nursing unit where the focus is palliative care. The patient care focus is on symptom relief for complex patients who may be continuing to undergo primary treatment. Care is delivered by palliative medicine specialists.
For hospitals with more than 50 beds, we corroborated palliative care program status in both the 2009 and 2017 AHA surveys through comparisons with the National Palliative Care Registry, state directories of palliative care programs, web searches, and phone conversations with hospital staff. A 10% false-positive and a 4% false-negative response error for self-reported palliative care status were identified, and data corrected accordingly (Supplementary Table 1).
Characteristics of Hospitals by Palliative Care Program Adoption and Closure Status, 2009–2017
The numbers of hospitals with palliative care in this study differ from the 2019 State-by-State Report Card 7 due to the inclusion of hospitals with less than 50 beds.
Residency training approval by the ACGME.
Member of COTH.
Cancer program approved by the ACS.
ACGME, Accreditation Council for Graduate Medical Education; ACS, American College of Surgeons; COTH, Council of Teaching Hospital of the Association of American Medical Colleges; HRR, hospital referral region; HSA, hospital service area; SD, standard deviation.
Hospital ownership was categorized as follows: (1) public, defined as government and nonfederal controlled by the state, county, city, city-county, or hospital district; (2) for-profit, defined as investor owned by individuals, partnerships, or corporations; and (3) nonprofit, defined as nongovernment not-for-profit operated by a church or other not-for-profit. Hospital size was defined by the total number of beds set up and staffed for use, less the number of nursing home beds, if applicable, and categorized as follows: (1) fewer than 50 beds; (2) 50 to 149 beds; (3) 150–299 beds; and (4) 300 or more beds.
Models include demographic data on the Medicare population in the HRR (percent of the population who are non-Hispanic white, percent eligible for Medicaid, and average age), as well as data on physician capacity (total physicians, specialist physicians, and hospital-based physicians per 10,000 residents), and average Medicare and hospice reimbursements per enrollee in the HSA.
Statistical analyses
We analyzed bivariate associations between hospital and regional characteristics and the closure and adoption of hospital palliative care programs utilizing χ 2 analysis, ANOVA, and t-tests, as appropriate. We used two separate multivariable logistic regression models to examine the adjusted associations between hospital and geographic characteristics and the likelihood of (1) palliative care program adoption and (2) palliative care program closure. All analyses held hospital characteristics at their 2009 values. We performed analyses using STATA 16.
Results
Our sample included 3696 hospitals in the United States (Table 1). In 2009, 37.0% (1369/3696) of hospitals of all sizes reported palliative care. By 2017, the percentage of hospitals with palliative care had increased to 53.5% (1976/3696).
Between 2009 and 2017, the overall adoption rate of palliative care programs in hospitals was 34.9%. That is, of the 2327 hospitals without palliative care in 2009, 812 had started programs by 2017. This is an average of 101.5 new hospital palliative care programs opening per year. The overall closure rate of palliative care programs was 15% (205/1369), an average of 25.6 closures per year. Furthermore, 85.0% (1164/1369) of hospital palliative care programs that existed in 2009 remained open in 2017, and 65.1% (1515/2327) of hospitals without palliative care in 2009 still did not have palliative care eight years later (Fig. 1).
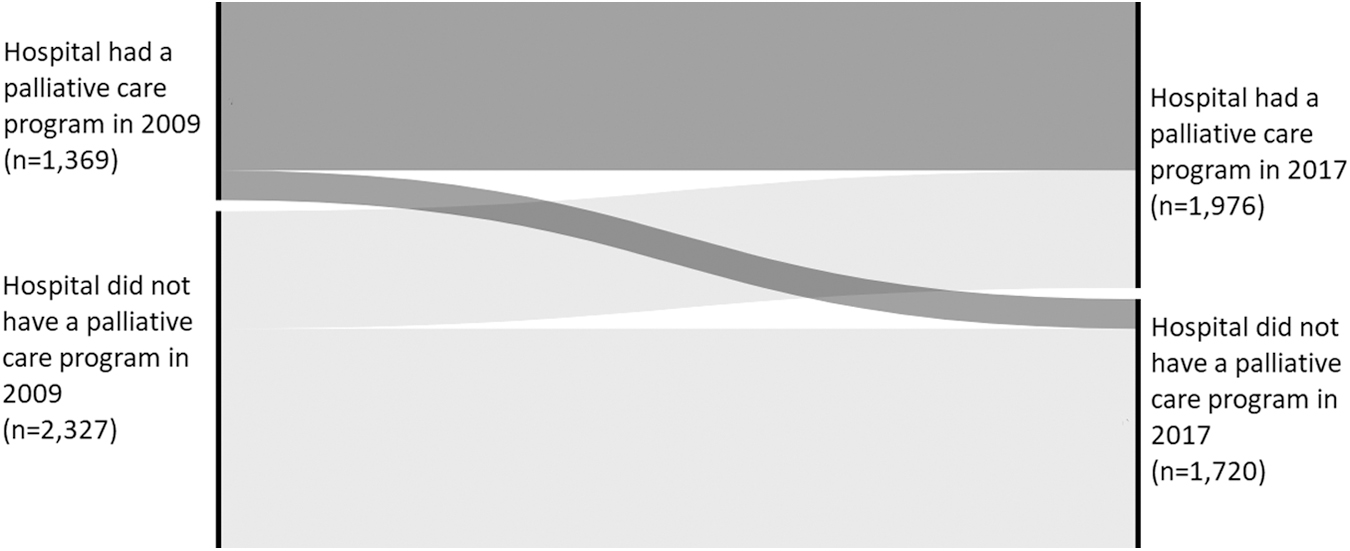
Hospital palliative care program adoption and closure trajectory, 2009–2017. This Alluvial diagram displays the hospital palliative care status in 2009 (on the left) with the 2017 palliative care status on the right. The height of the black bars (nodes) indicates the proportion of hospitals in each group. We defined palliative care program “adoption” as a hospital that did not have a palliative care program in 2009, but did in 2017, and palliative care program “closure,” as a hospital that did have a palliative care program in 2009, but no longer had one in 2017. The dark sliver that travels from the upper left diagonally to the lower right are the hospitals that closed their palliative care programs during the study period.
Factors associated with palliative care program adoption
The 812 hospitals that adopted palliative care since 2009 appeared different from the 1515 hospitals that did not adopt palliative care during the same period (Table 1). Between 2009 and 2017, most adoptions occurred in nonprofit hospitals, with 586 hospitals creating new programs.
Rates of palliative care program adoption also varied by hospital and geographic characteristics (Fig. 2). For-profit hospitals experienced the lowest rates of adoption, with only 17% of hospitals without palliative care in 2009 adopting programs by 2017. Other segments with adoption rates below 25% include public, sole community providers, rural, and hospitals in the South Central United States. Comparatively, hospitals with an American College of Surgeons cancer program had the highest adoption rate (71%), followed by hospitals with 300 or more beds, hospitals with residency training approval by the Accreditation Council for Graduate Medical Education (ACGME), and those in New England (all over 60%).
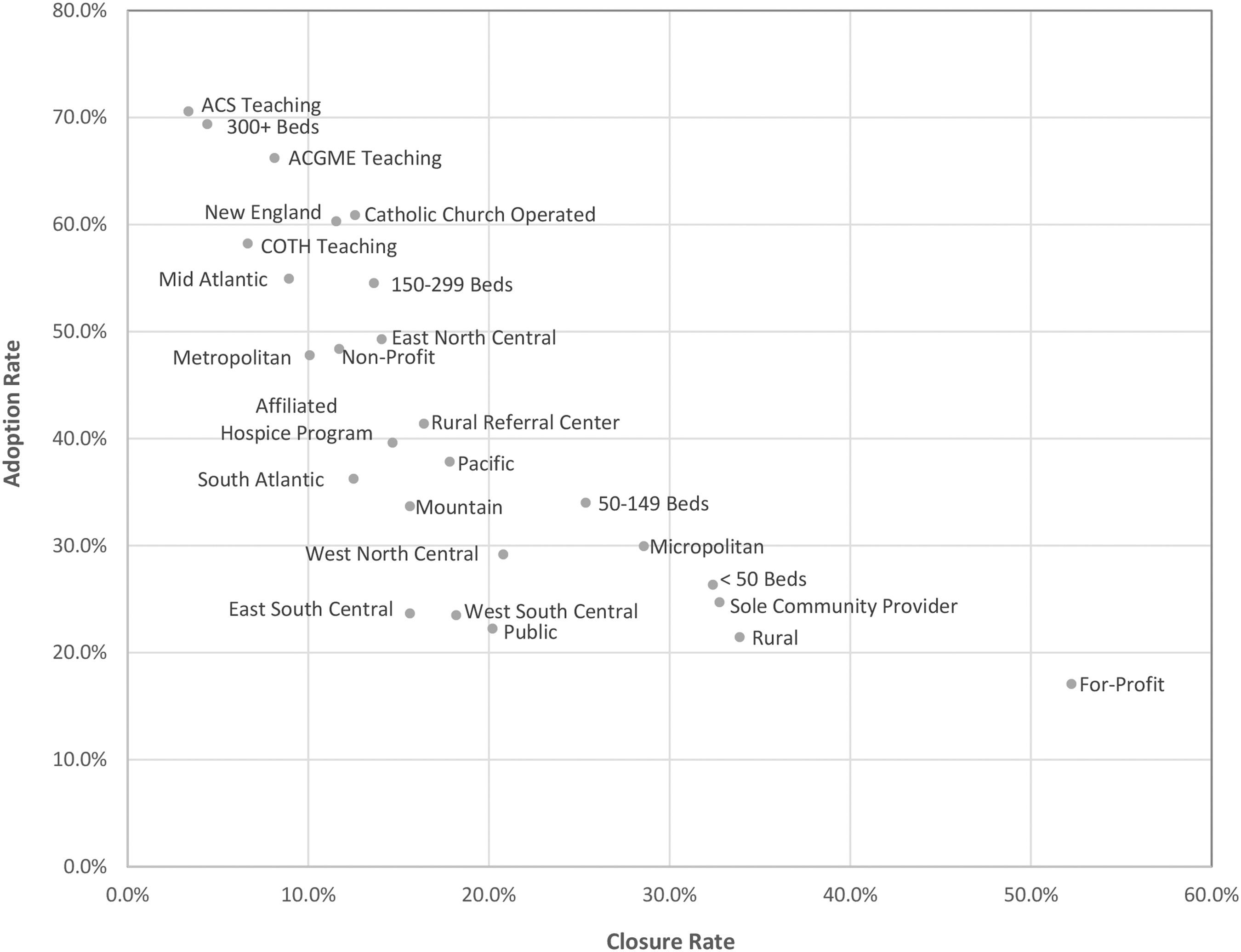
Adoption and closure rates of hospital palliative care programs by hospital characteristic, 2009–2017. Adoption rate is the percent of hospitals that did not report palliative care in 2009, but did in 2017. Closure rate is the percent of hospitals that reported palliative care in 2009, but no longer did in 2017. Teaching hospitals are represented with acronyms: Residency training approval by the ACGME, Member of COTH, and Cancer program approved by the ACS. ACGME, Accreditation Council for Graduate Medical Education; ACS, American College of Surgeons; COTH, Council of Teaching Hospital of the Association of American Medical Colleges.
In the multivariable model, hospitals with 300 or more beds (compared to hospitals with fewer than 50 beds), nonprofit and public hospitals (compared to for-profit hospitals), teaching hospitals, and Catholic Church-operated hospitals were significantly more likely to adopt a palliative care program during the study period (Table 2). Geographically, hospitals in metropolitan and micropolitan areas were associated with a significantly higher likelihood of palliative care adoption (compared to rural).
Association between Hospital Palliative Care Program Adoption or Closure and Hospital and Geographic Characteristics, 2009 and 2017
Adoption Model: Hospitals without palliative care in 2009 that have adopted versus hospitals without palliative care in 2009 that have never adopted.
Closure Model: Hospitals with palliative care in 2009 that have closed programs versus hospitals with palliative care in 2009 that have kept their programs.
Residency training approval by the ACGME.
Member of COTH.
Cancer program approved by the ACS.
p < 0.05, **p < 0.01, ***p < 0.001.
Factors associated with palliative care program closure
The 205 hospitals that closed palliative care programs since 2009 appear to differ from the 1164 that remained open (Table 1). During the study period, the greatest absolute number of program closures occurred in nonprofit hospitals, in which 128 nonprofit hospitals closed their palliative care programs between 2009 and 2017.
The highest closure rates were in for-profit hospitals, where 52% of for-profit hospitals with palliative care in 2009 closed their programs by 2017 (Fig. 2). This closure rate exceeded the adoption rate (17%) in for-profit hospitals, resulting in the loss of 35 palliative care programs. Similar patterns existed for rural hospitals, small hospitals (<50 beds), and sole-provider hospitals. Comparatively, hospitals with 300 or more beds, teaching hospitals, and hospitals in the Mid-Atlantic had closure rates below 10%.
In the multivariable closure model, sole community provider status, hospitals without ACGME residency training programs, and for-profit hospitals (compared to nonprofit and public hospitals) were significantly more likely to close a palliative care program during the study period (Table 2). Hospitals in the East South Central United States and rural areas also had a significantly higher likelihood of palliative care closure.
Discussion
Our national study of longitudinal changes in hospital palliative care programs highlights significant shifts in the field. Between 2009 and 2017, 35% of hospitals without palliative care opened a new program, while 15% of hospitals with palliative care closed their programs during the same period. This amounts to a net gain of 607 palliative care programs between 2009 and 2017, or for every 1 hospital that closed a program, an average of 4 hospitals added palliative care programs. Controlling for hospital and geographic characteristics, hospitals exhibiting high rates of palliative care program closure were more likely to be for-profit, nonteaching, rural, or sole community providers.
Prior research has demonstrated that for-profit hospitals consistently have lower palliative care prevalence rates than other ownership types. 12 This study suggests that not only are for-profit hospitals less likely to initiate a palliative care program but also are less likely to maintain one once started. Prior research has shown that tax status influences operations. 15 Specifically, for-profit companies need to demonstrate short-term profitability to maintain shareholder interest/investment and market price. The pressure to consistently demonstrate profitability for shareholders may shift institutional priorities to more visible high-revenue services, such as surgery, and away from services like palliative care 16 whose contributions to a hospital's bottom line and value are more difficult to demonstrate and explain to investors and leadership. 3 Specifically, while the revenue generated by complex procedures and high-margin diagnoses (i.e., cancer) is relatively easy to capture through hospital cost-accounting systems, the cost-savings attributable to palliative care are derived from unnecessary tests not performed or expensive medications not administered, which are considerably more challenging to quantify and explain. 3 We hypothesize that these factors contribute to the low adoption rate and higher closure rate of palliative care programs in for-profit hospitals.
Our finding regarding high closure rates at rural and sole community provider hospitals is concerning. Designated by CMS, sole community hospitals are isolated due to location, weather, or travel conditions, or absence of other hospitals and, in some parts of the country, are the sole source of inpatient care available. In addition, rural hospitals have faced significant hospital closures over the past decade, with even more rural hospitals at risk of closure. 17 Access to both primary care providers and specialists for rural residents is linked to lower preventable hospitalization rates and lower mortality rates. 18 Smaller hospital sizes and fewer seriously ill patients may be the reason that these hospitals are unable to support palliative care teams. Ensuring that specialty palliative care remains available in vulnerable areas requires particular attention. Mounting evidence regarding the potential of alternative palliative care delivery models, such as telehealth, provides a potential solution for hospitals that cannot support a full specialty palliative care team.19,20
Finally, this study sets a foundation for future research directions. Studies that identify the reasons for palliative care program closures, the specific motivators behind hospital adoption of programs, and further exploration as to why hospital ownership influences the development of palliative care are needed. In addition, although we anticipated a relationship between hospitals with affiliated hospice programs and the adoption of palliative care, we did not find one likely due to the strong relationship between hospice and hospital ownership. Greater understanding of hospice and palliative care program collaborations within hospital settings is needed.
Similarly, further studies are needed to identify organizational and operational challenges faced by existing programs to preserve and enhance the services they provide to seriously ill persons and their families. Two studies on hospital palliative care in California identified limited or uncertain funding and limited staffing as the two biggest challenges for keeping programs open.21,22 Without federal and state policy interventions to ensure access to palliative care for people living with serious illness (e.g., through accreditation requirements), including investment in an adequate specialty palliative care workforce and sustainable financing for palliative care clinical services, future access to this high-value care will remain variable and inequitable. Promoting public and clinician awareness of palliative care and its benefits may further drive program adoption through the generation of patient demand for the highest quality care during serious illness. 23
Limitations
Our study had several limitations. We were not able to measure the quality of the care provided or the capacity of the programs studied, which are known to vary significantly across palliative care programs. 24 We held hospital characteristics at their 2009 values and thus were not able to examine how simultaneous changes in hospital size, ownership, or teaching status affect palliative care program adoption and closure rates. We further did not have information on when a hospital established a palliative care program and, therefore, could not determine how long programs were in operation before closing. We did not corroborate the AHA self-reported responses for palliative care program status in hospitals with fewer than 50 beds and, therefore, may have overestimated or underestimated the palliative care program prevalence in this group.
Conclusions
Our study indicates that palliative care is not equitably adopted or sustained by hospitals in the United States. Rural, for-profit, sole-community, and non-ACGME hospitals have experienced the highest rates of closure when controlling for hospital and geographic characteristics. Large, nonprofit, public, teaching, Catholic Church-operated, and hospitals in micropolitan and metropolitan areas were associated with a higher likelihood of palliative care adoption. Federal and state interventions may be required to ensure that high-quality care is available to our nation's sickest patients, regardless of where they live and the tax status of the hospital in which they receive care.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.