
Abstract
Background:
Health care interprofessionals face competing obligations to their patients, employers, and themselves. When ethical conflicts ensue and competing obligations cannot be resolved, health care interprofessionals have reported experiencing symptoms of burnout, moral distress, and other types of moral suffering. Recently, moral resilience or “the capacity of an individual to sustain or restore their integrity in response to moral adversity,” has been proposed as a resource to address moral suffering while contributing to well-being.
Objectives:
Develop and validate an instrument to measure moral resilience.
Design:
Phase one: item development and expert review. Phase two: focus groups with health care interprofessionals to refine items. Phase three: psychometric testing.
Setting/Subjects:
Seven hundred twenty-three health care interprofessionals participated; inclusion criteria included being a chaplain, nurse, physician, or social worker, and having practiced at least 1 year. Participants were recruited from seven academic and community hospitals in the Eastern United States.
Results:
One hundred items were created for expert review. Following focus groups to refine items, 35 items remained for psychometric testing. Eighteen items were removed following item analysis. Exploratory factor analysis (EFA) of the remaining items suggested a four-factor solution, titled Responses to Moral Adversity, Personal Integrity, Moral Efficacy, and Relational Integrity, respectively. Overall reliability was α = 0.84. The Rushton Moral Resilience Scale (RMRS) demonstrated convergent validity with the Connor Davidson Resilience Scale-10 and criterion validity with the Maslach Burnout Inventory–Human Services Survey.
Conclusion:
The RMRS demonstrated acceptable validity and reliability. Examining the factor structure of moral resilience contributes to burgeoning moral resilience science and enables future research. Moral Resilience offers a promising pathway to support interprofessionals' integrity even when faced with ethical challenges.
Introduction and Background
It is inevitable that health care interprofessionals will face ethical challenges as they conduct their work. 1 As health care technology advances, increasing diversity ensures a plurality of values and new challenges surface, disagreement about the “right thing to do” is inevitable. 2 Daily, clinicians must balance competing obligations and commitments to patients, families, health care institutions, and themselves. These factors have only intensified in the recent COVID-19 pandemic, revealing the need to equip health care interprofessionals to face these challenges in a way that preserves their integrity and well-being.
When values clash and there is no consensus on the appropriate action to take, or competing obligations cannot be reconciled, health care interprofessionals may feel as though their integrity is threatened in response to various types of moral adversity.3–5 Moral adversity “occurs when internal or external circumstances or actions produce morally objectionable, troublesome, or unfortunate results that can imperil integrity and well-being—individually or collectively.” 6 Moral adversity may lead to various forms of moral suffering, including moral distress and injury, moral residue, and contribute to burnout.7,8 Moral distress is the most commonly studied form of moral suffering among health care interprofessionals; it is prevalent particularly among those who work in critical settings and with patients at the end of life, such as neonatal/pediatrics, oncology, and the emergency department.9,10 Palliative care professionals are also more likely to experience moral distress because of factors such as proximity to suffering, and responsibility to facilitate end-of-life decisions 11
Burnout is another concern in the health care workforce.12–17 It is estimated that 35%–45% of nurses18,19 and 40%–45% of physicians 20 experience burnout, which is a concerning statistic, but this statistic also leads to the conclusion that the majority of sampled nurses and physicians do not experience burnout. A better understanding of the constructs that lead a health care professional to develop protective behaviors and positive coping mechanisms may be instrumental in helping health care interprofessionals to meet ethical challenges with less personal and professional damage.
Recently, the concept of moral resilience has emerged as a potential pathway to health care interprofessional well-being. Moral resilience, “the capacity of an individual to sustain or restore their integrity in response to moral adversity,” has the potential to guide health care interprofessionals who seek to maintain integrity in the face of everyday ethical challenges. 6
Very little empirical research focused on moral resilience has been conducted. A concept analysis of moral resilience found the known antecedents of moral resilience include ethics education; creating meaning in life; understanding a diversity of human values; moral adversity; and reducing ethical complexity. 21 The same concept analysis also revealed the following attributes of moral resilience: enables a person to navigate morally complex situations; reduces moral distress; and supports a person to have integrity by being true to one's values and convictions. 21 Sala Defilippis et al. conceptualized moral resilience as a moral virtue, with the associated vices of faintheartedness and rigidity. 22 Furthermore, Holtz et al. 23 published six domains of moral resilience derived from qualitative analysis of interprofessionals' definitions of moral resilience (Table 1).
Descriptions of Previously Identified Domains of Moral Resilience
One of the primary hindrances to furthering the study of moral resilience is the lack of a valid and reliable instrument to measure moral resilience. Such an instrument would allow researchers to describe moral resilience among health care interprofessionals, and test interventions designed to effect moral resilience. 21
Therefore, the purpose of this study was to develop and validate a measure of moral resilience among a sample of health care interprofessionals, including chaplains, nurses, physicians, and social workers.
Materials and Methods
This study was carried out in three phases: (1) item development, (2) item refinement, and (3) psychometric testing.
Phase one: Item development
Literature review 21 informed the overall conceptualization of moral resilience. A previously published work established six constructs of moral resilience (Table 1), 23 and these constructs formed the basis for items included in the Rushton Moral Resilience Scale (RMRS). Items were created a priori, and related scales were hand-searched to ensure established themes related to resilience were represented.
To establish content validity, six experts in resilience and ethics (three philosophers, two physicians, and one nurse) reviewed the items and provided written feedback related to (1) the relevance of each item to the concept of moral resilience, (2) the wording of the items, and (3) concepts related to moral resilience that were not captured in the items of the RMRS (see Fig. 1 for recruitment diagram).
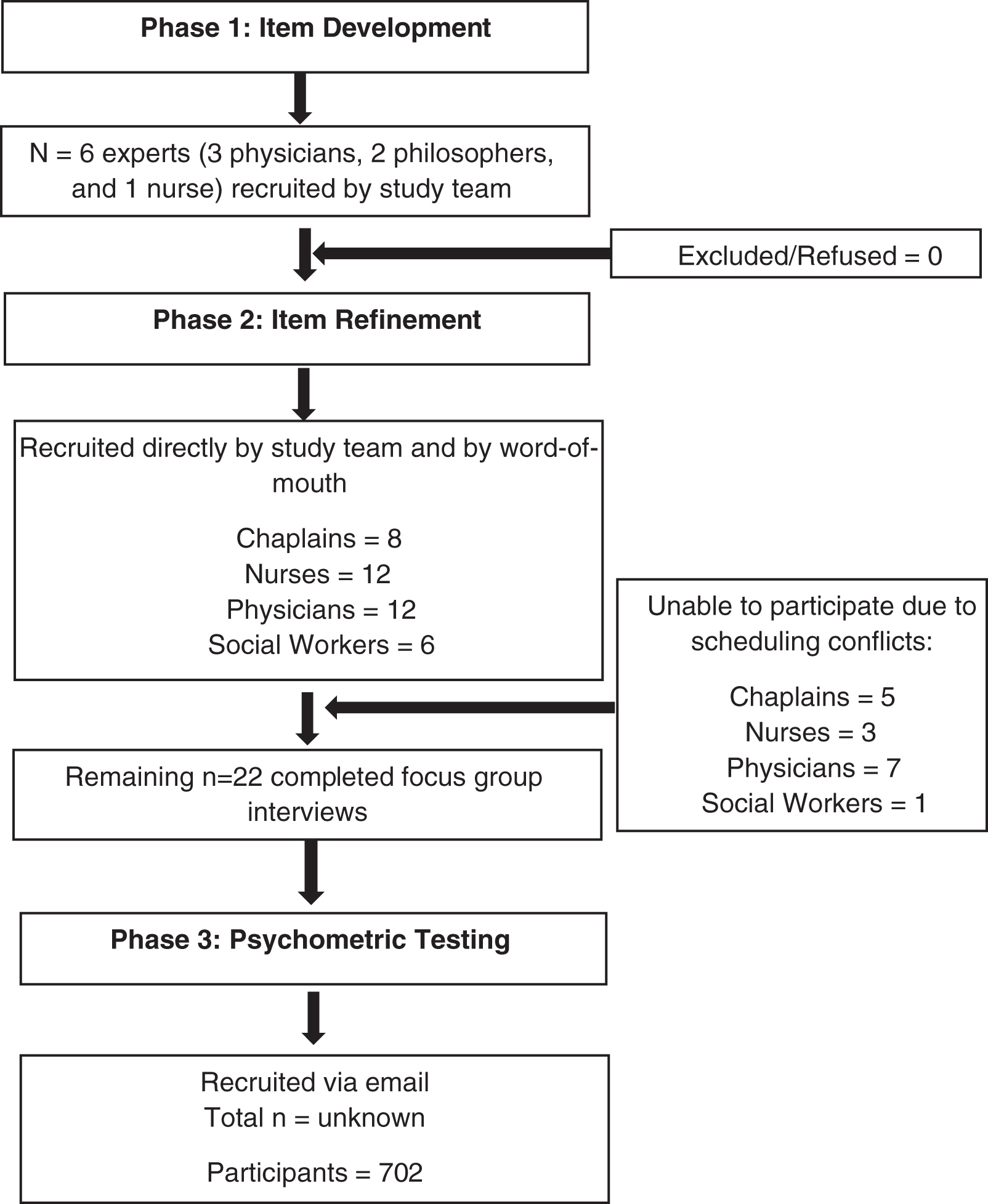
Participant flow diagram.
Phase two: Item refinement
To further refine items and strengthen content validity, practicing health care interprofessionals participated in focus groups. Study procedures were approved by the Johns Hopkins University Institutional Review Board. Participants were recruited by invitation of the study team and word-of-mouth, with the goal of including at least two of each: chaplains, nurses, physicians, and social workers. Focus groups were recorded and transcribed verbatim by a Health Insurance Portability and Accountability Act (HIPAA) compliant transcription company.
Focus group participants completed both the RMRS and demographic information, and then were invited by the interviewers (K.E.H. and C.H.R.) to comment on each question. The interviewers used cognitive interviewing techniques24,25 to help participants elucidate thought processes. Participants also identified which items they thought were the most and least clear in representing the constructs and meaning of moral resilience.
The authors read the interview transcripts and compared texts across groups to discern common themes. Items were refined and/or removed iteratively until the RMRS was finalized for psychometric testing.
Phase three: Psychometric testing
Recruitment
Practicing chaplains, nurses (registered nurses and advanced practice nurses), physicians, and social workers were recruited via email from five hospitals: Johns Hopkins All Children's Hospital (St. Petersburg, FL), Allegheny Medical Center (Pittsburgh, PA), Ann Arundel Medical Center (Annapolis, MD), Inova Health System (Falls Church, VA), and Reading Hospital–Tower Health (West Reading, PA). Allegheny Medical Center, Ann Arundel Medical Center, and Reading Hospital participated via the Johns Hopkins Clinical Research Network. Survey participation was voluntary and anonymous, but participants did have the option to enter a drawing for one of five $100 gift cards. Each study site sent the recruitment email three times. The target sample size was 340 participants (10 per RMRS item), and at least two participants from each profession.
Study measures
Participants completed the RMRS, Connor Davidson Resilience Scale-10 (CD RISC-10), Maslach Burnout Inventory–Human Services Survey (MBI–HSS), and a demographic form created by the authors.
Rushton Moral Resilience Scale
The RMRS had 34 items scored on a 4-point Likert scale (1 Disagree, 2 Somewhat Disagree, 3, Somewhat Agree, or 4 Agree). Higher scores indicate higher moral resilience. A priori the items were designed to represent the six domains of moral resilience.21,23 See Supplementary Appendix A1 for a list of RMRS items.
Connor Davidson Resilience Scale-10
The CD RISC-10 is a 10-item version of the CD RISC, which measures general resilience 26 ; items are scored on a 5-point Likert scale (0 Not true at all, 1 Rarely true, 2 Sometimes true, 3 Often true, or 4 True nearly all the time).
Maslach Burnout Inventory–Human Services Survey
The MBI–HSS is a widely used burnout scale adapted specifically for human service professionals. The MBI–HSS comprises three subscales: Emotional Exhaustion, Depersonalization, and Personal Accomplishment. 27 Responses were given on the following scale: 0 (never); 1 (a few times a year or less); 2 (once a month or less); 3 (a few times a month); 4 (once a week); 5 (a few times a week); and 6 (every day).
Analysis
Descriptive statistics were used to describe the sample. Several item analysis tools were used, including item means, item standard deviations, item-total correlations, and interitem correlations to examine the functioning of individual items. Items that had little variability or low correlations were omitted. Exploratory factor analysis with iterative principle axis factoring was used to examine the factor structure. Factors with an Eigenvalue >1 were considered for retention, and the item loading threshold was set at 0.4. Correlations between the subscales of moral resilience, resilience, and burnout were examined. Finally, one-way analysis of variances (ANOVAs) with Bonferroni follow-up tests was used to examine differences between the subscales of moral resilience by profession and practice setting.
Results
Phase one: Item development
Each of the six recruited experts agreed to provide item feedback. The authors created 100 items for review. Following expert review, 7 items were removed, 93 items were edited for content and clarity, and 2 items were added.
Phase two: Item refinement
Twenty-two health care interprofessionals attended one of seven focus groups between March 13 and April 5, 2018. After the first two focus groups, the study team met to review the transcripts. Twenty-two items were removed from the scale and the remaining 73 items were revised.
After focus group five, 27 items were removed, 2 items were added, and the remaining 48 items were revised. After focus group seven, 17 items were removed and 3 items were added, resulting in 34 items.
Phase three: Psychometric testing
A total of 702 participants were recruited for the validation study between August 30, 2018 and October 31, 2018. Average time to complete all survey measures was 57 minutes. See Table 2 for descriptions of study participants.
Demographic Characteristics
Declined to answer = 63.
OB/GYN, obstetrics and gynecology; SD, standard deviation.
The variability of each item of the RMRS was analyzed using the mean, standard deviation, frequency distribution, and bivariate correlations among items. At the preliminary subscale level, we also looked at the item total correlation and alpha if item dropped. Items were dropped if they had a standard deviation of <1, no bivariate correlations of 0.3 or greater, an item total correlation ≤0.5, or if dropping the item would notably increase alpha. Based on these criteria, 18 of the original 34 items were retained.
Factor analysis
A common factor analysis using iterative principle axis factoring was used to explore the factor structure of the remaining 18 items. Oblique rotation was used, because subscales were expected to be correlated. The analysis resulted in four factors with Eigenvalue >1, and four factors explaining at least 5% of the variability in the items, supporting a four-factor solution. In the pattern matrix, nearly all items demonstrated simple structure loading at 0.4 or above and at least 0.2 higher on one factor than the other factors. Two items had factor loadings that were below 0.4: (1) “I am reluctant to take an unpopular position,” factor loading = 0.35 and; (2) “I voice my ethical concerns in a way that others take seriously,” factor loading = 0.39. The first item was omitted because of its low factor loading and its redundancy with the other items. The second item was retained because its factor loading was nearly 0.4, and it captured a unique aspect of moral resilience that other items did not. The final factor analysis explained 41.34% of the variability.
Items that had a factor loading of 0.39 or above on one factor were interpreted as part of that factor (Table 3). The five items that loaded on factor 1 were mainly made up of items developed to measure buoyancy and self-regulation. These items had in common a person's reaction to ethical challenges, thus we named this factor Responses to Moral Adversity. The second factor was made up of three items that were intended to measure personal integrity, thus we named it Personal Integrity. The third factor included moral efficacy items, thus we named this factor Moral Efficacy. The fourth factor was made up of items from relational integrity and self-stewardship domains about compromising one's ethical values when facing conflict with others, thus we named this factor Relational Integrity.
Factor Loadings for the Four-Factor Moral Resilience Scale (N = 689; Missing = 13)
Note: (R) These items were reverse coded. All items were coded so that higher scores indicated higher moral resilience.
Convergent validity
Correlations were assessed between the subscales of the RMRS and other related scales, specifically the CD RISC-10 and MBI–HSS (Table 4). As theorized, the RMRS was positively correlated with the CD RISC-10 and negatively correlated with the MBI–HSS. The majority of the correlations were moderate, but the Personal integrity factor was weakly correlated with the CD RISC-10 and the MBI HSS. Overall, these results demonstrate the convergent validity of the RMRS.
Correlations of the Moral Resilience Scale
p < 0.01, **p < 0.001.
The Connor Davidson Resilience Scale ranged from 0 to 40 where high scores indicate greater resilience. Depersonalization ranged from 0 to 35 where higher scores indicate higher depersonalization. Emotional exhaustion ranged from 0 to 63 where higher scores indicate higher emotional exhaustion. Personal accomplishment ranged from 0 to 56 where higher scores indicate higher emotional exhaustion. Factor 1, personal integrity, moral efficacy, and factor all range from 1 to 4 where higher scores indicate greater moral resilience.
The reliability for the overall RMRS was α = 0.84. The reliability for the four factors are as follows: factor 1 α = 0.78, factor 2 α = 0.50, factor 3 α = 0.69, and factor 4 α = 0.78.
Differences by professional role and primary practice location
One-way ANOVAs with Bonferroni follow-up tests were used to examine differences in each of the moral resilience subscales by professional role and primary practice setting. Differences by professional role were found in Responses to Moral Adversity (F = 5.82, p = 0.001) and Moral Efficacy (F = 5.81, p = 0.001), but not in Personal Integrity or Relational Integrity. Specifically, chaplains scored higher in Responses to Moral Adversity than both nurses and physicians (Table 5). Nurses had lower Moral Efficacy than both chaplains and physicians. Differences by primary practice setting were found only in Personal Integrity (F = 3.14, p = 0.008); outpatient/ambulatory employees rated their personal integrity as higher than employees in inpatient-critical care.
Differences on Moral Resilience Subscales by Professional Role and Setting
Means with the same superscript letter are statistically different at the p < 0.05 level using one-way analysis of variance with Bonferroni follow-up tests.
Discussion
Main findings
To our knowledge, the RMRS is the first scale developed to measure Moral Resilience among health care interprofessionals. Because the construct of moral resilience has only recently emerged in health care literature, it was necessary to establish construct validity. To this end, we based item development on existing published literature, including a concept analysis of moral resilience 21 and a content analysis of interprofessionals' definitions of moral resilience. 23 We then sought expert input to ensure the items adequately addressed to known domains of moral resilience. Finally, we recruited end-users into a series of focus groups to test and refine the items.
Once these steps to establish construct validity were complete, 702 health care interprofessionals participated in a larger study designed for psychometric testing. Study measures included demographic information, the RMRS, CD RISC-10, and the MBI–HSS. Factor analysis suggested a solution with 17 items and 4 factors, which explained 41% of the variation. Scale items were developed using the six previously described domains of moral resilience (Personal Integrity, Relational Integrity, Buoyancy, Self-Regulation, Self-Stewardship, and Moral Efficacy), and we therefore theorized that EFA would reveal a six-factor solution. However, when we examined the four factors suggested by EFA, items from all six of the original domains were retained, which satisfied us that construct validity was intact. With further use and testing of the scale, confirmatory factor analysis and other psychometric methods will further strengthen the theoretical factor structure of the RMRS.
The RMRS had an overall reliability of α = 0.84, indicating acceptable reliability. The factors, titled Responses to Moral Adversity (five items, α = 0.78); Personal Integrity (three items, α = 0.50); Moral Efficacy (four items, α = 0.69); and Relational Integrity (five items, α = 0.78), demonstrated acceptable reliability except for Personal Integrity, which had the fewest items. Reliability may be improved by testing additional items in future studies.
As theorized, convergent validity was demonstrated with a moderate positive correlation to general resilience, and criterion validity was demonstrated with a moderate negative correlation to burnout. Taken together, we feel these psychometric tests demonstrate that the RMRS is a valid and reliable measure of moral resilience.
Chaplains scored higher on Responses to Moral Adversity than both nurses and physicians. This result is in line with other reports that chaplains as a group report high resilience, 28 and may stem from a greater repertoire of skills to handle moral adversity or from training in the chaplaincy to cultivate inner capacities. Nurses had lower Moral Efficacy than both chaplains and physicians. One possible explanation is that nurses may feel that they have less control over moral decisions as they are often subject to oversight by other members of the care team, and thus have less decisional latitude. 29 Outpatient/ambulatory employees rated their personal integrity as higher than employees did in inpatient critical care; it is possible that this finding is due to the lower acuity and higher predictability of the outpatient setting, but further research is warranted. The different patterns of results by subdomain provide further evidence that these subdomains are meaningfully distinct.
Strengths and weaknesses of the study
A multistep process was used to establish validity of the RMRS, demonstrating the rigor of the scale. The contributions of theoretical experts, methodological experts, researchers, and clinicians strengthened the RMRS, from item development to psychometric testing. Furthermore, utilizing the Johns Hopkins Clinical Research Network enabled us to recruit a large sample for psychometric testing.
Although we used a rigorous process to establish scale validity, it is possible that there are constructs related to moral resilience not included in the RMRS. Demographic information for all participants—the demographic form was placed last among the surveys, and not all participants chose to fill out the form. In addition, participants' gender and ethnicity were not assessed, which may limit the generalizability of the results. Finally, the goal of the RMRS is not to “diagnose” moral resilience, or lack thereof, but to provide insights about capacities that can be amplified and strengthened to confront inevitable ethical challenges in health care; individual moral resilience scores should not be used to determine a cutoff for adequate moral resilience.
What this study adds
This study's investigation of the factor structure of moral resilience as a construct contributes to the science of moral resilience in health care interprofessionals. The four identified factors—Responses to Moral Adversity, Personal Integrity, Moral Efficacy, and Relational Integrity—provide guidance for future scientific inquiry. This scale will enable interventional research to aid health care interprofessionals to address ethically challenging situations in their clinical practice. With the new moral challenges of COVID-19, 30 research and interventions designed to understand and promote moral resilience may be critical to support health care interprofessionals.
Finally, while this scale focuses on moral resilience at the individual level, it is of the utmost importance that interventions designed to foster individual moral resilience are accompanied by changes at the institutional level. Without institutional change, it will be nearly impossible for individuals to change health care culture from the bottom up. 6
Conclusion
The RMRS is a valid and reliable measure of moral resilience. Future studies designed to test moral resilience interventions will continue to shape the science of moral resilience.
Authors' Contributions
K.E.H. managed the three phases of the study and drafted the article; G.H. completed all statistical analyses, drafted portions of the article related to statistical analysis, and contributed to the interpretation of analysis; S.S. and H.H. contributed substantively to the design and completion of the study, and reviewed the article; C.H.R. conceptualized the study, cofacilitated focus groups, contributed to data interpretation, guided its completion, and contributed to every portion of the article.
Footnotes
Acknowledgments
Research recruitment partially completed through The Johns Hopkins Clinical Research Network, under the Johns Hopkins Institute for Clinical and Translational Research (ICTR), which is funded, in part, by Grant Number UL1 TR 001079 from the National Center for Advancing Translational Sciences (NCATS) a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research.
Disclaimer
The contents are solely the responsibility of the authors and do not necessarily represent the official view of the Johns Hopkins ICTR, JHCRN, NCATS, or NIH.
Funding Information
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Dorothy Evens Lynn Fund at the Johns Hopkins School of Nursing.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.