
Abstract
Background:
Health professionals who care for patients and their families at the end of life (EOL) may experience gratitude, and enhanced spirituality and meaning in life, yet they are also at increased risk of psychological distress, compassion fatigue, and occupational burnout given the stressors they encounter in their work.
Objectives:
This research evaluated the feasibility and acceptability of a novel six-week mindfulness-based compassion training intervention, which was tailored to health professionals involved in EOL care (“MBCT4HP”), and explored its impact on levels of psychological distress, compassion fatigue, compassion satisfaction, occupational burnout, self-compassion, and mindfulness.
Design:
We adopted an observational, repeated measures pilot study.
Setting/Subjects:
Thirty-one health professionals participated. The intervention comprised six, weekly sessions (totaling seven hours) designed to foster compassion for self and others, including formal and informal compassion and mindfulness practices, daily home practice, and a reflective experiential pedagogy.
Measurements:
Validated outcome measures for anxiety, depression, and stress; compassion satisfaction, compassion fatigue (burnout, secondary traumatic stress); occupational burnout (emotional exhaustion, personal accomplishment, and depersonalization), self-compassion, and mindfulness were administered at baseline, end of intervention, and eight weeks postintervention. The feasibility and acceptability of the intervention was assessed using attendance records, home practice logs, and self-report satisfaction items. Descriptive statistics and Generalized Linear Mixed Models were used to analyze the data.
Results:
Participants reported that the sessions were useful, relevant, easy to understand, and that they gave them sufficient knowledge to implement the strategies learned. Levels of anxiety, compassion fatigue (burnout only), and emotional exhaustion decreased over time with some decay in effects at follow up, and levels of compassion satisfaction and self-compassion increased with time.
Conclusions:
The intervention was feasible and acceptable to health professionals involved in EOL care and had a positive impact on levels of anxiety, compassion fatigue (burnout), emotional exhaustion, compassion satisfaction, and self-compassion.
Introduction
Health professionals involved in providing palliative and end-of-life (EOL) care report enhanced spirituality and meaning, 1 and feelings of satisfaction and gratitude. 2 They also confront significant challenges and stressors, including frequent exposure to the suffering of others around death and dying. 3 In a recent survey of palliative care clinicians in the United States, 38.7% reported at least one symptom of burnout. 4 Burnout results from extreme occupational stress. 5 It includes increased mental distance from one's work or feelings of cynicism (depersonalization), a reduced sense of professional accomplishment, and emotional exhaustion, resulting in poorer well-being and compromised patient care.5,6 While compassion fatigue is more difficult to define, it commonly refers to distress, which arises from care providers' exposure to the suffering and trauma of others. 7 “Empathic distress fatigue” has been proposed as a more accurate term for this phenomenon.8,9 For the purposes of this research, however, we retain the more widely used term “compassion fatigue.”
Compassion refers to feelings of warmth, concern, and care for self or another who is suffering, with a commitment to try and alleviate it. 10 Compassionate care, in turn, is a relational activity where people recognize others' suffering, resulting in an emotional response and prosocial actions. 11 Health professionals' capacity to provide quality, compassionate patient care is enhanced through practicing compassion for themselves. 12 Self-compassion is an essential component of self-care, 13 particularly for palliative care professionals who are constantly exposed to death and the suffering and emotional distress of patients and families at EOL. 14
In the last two decades, attention has focused on the role of mindfulness-based programs to support health professionals' well-being 15 and programs to cultivate compassion for self and others. 16 Mindfulness is “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment”.17,p.145 Compassion and mindfulness are related but different constructs16,18; mindfulness is a nonreactive presence applicable to all experience, whereas compassion is an orientation to the alleviation of suffering. 16 Among health professionals, high levels of compassion fatigue are associated with lower levels of mindfulness. 19 In oncology health professionals, mindfulness is associated with lower disengagement, lower emotional exhaustion, higher compassion satisfaction, lower secondary traumatic stress, and lower compassion burnout. 20 Lower levels of compassion fatigue and higher levels of compassion satisfaction both predict lower levels of burnout, including lower emotional exhaustion and depersonalization in frontline health care professionals. 21 A consistent finding is that higher self-compassion is associated with lower levels of psychopathology, including lower levels of depression, anxiety, and stress.22,23 Self-compassion also appears to be protective against burnout and compassion fatigue among trainee health professionals 24 and health professionals working in emotionally demanding areas, including bereavement 25 and mental health. 26
Mindfulness-based stress reduction (MBSR) interventions, 27 compassion cultivation training (CCT), 28 mindful self-compassion (MSC) training, 29 and other compassion-focused training have been utilized to foster compassion among health professionals30–32 with positive effects on levels of empathy, self-compassion,33–35 distress,36–38 compassion fatigue, and burnout.31,39,40 For example, an 8-week MSC intervention (2.5 hours/week) piloted among nurses was associated with increases in self-compassion, mindfulness, and compassion satisfaction, and decreases in compassion fatigue. 35 In the palliative setting, a pilot evaluation of a 10-week “on-the-job” mindfulness intervention, comprising cultivation of mindful awareness, loving kindness, and tong-len meditations resulted in significant reductions in stress, anxiety, and burnout. 41
The intentional cultivation of both mindfulness and compassion among health professionals involved in palliative and EOL care is a rapidly developing area of research. 42 Previous qualitative research assessing health professionals' experiences of mindfulness training highlighted the need to align the scheduling and content of interventions with participants' demanding work schedules, and the importance of providing them with an evidence base for the practices. 43 These recommendations were incorporated in the development of the current intervention. Additionally, the health professionals and hospital executive we consulted viewed a 10-week “on-the job” program as unfeasible in the Australian acute health care setting and in other settings where health resources are constrained.
The goal of the current research was twofold. First, to test the feasibility and acceptability of a shorter, six-week mindfulness-based compassion training intervention, which was developed and tailored to health professionals involved in EOL care (coined “MBCT4HP”). Second, to explore its impact on levels of psychological distress (depression, anxiety, and stress), occupational burnout (emotional exhaustion, depersonalization, and personal accomplishment), compassion fatigue (burnout and secondary traumatic stress), self-compassion, and mindfulness.
It was hypothesized that MBCT4HP would be associated with:
Lower levels of depression, anxiety, and stress; Lower levels of compassion fatigue (secondary traumatic stress and burnout), emotional exhaustion, and depersonalization; Higher levels of self-compassion, mindfulness, compassion satisfaction, and personal accomplishment.
Methods
Design
An observational pre/post pilot study with outcome measures administered immediately before (Time 1), after the intervention (Time 2), and eight weeks postintervention (Time 3).
Intervention
The concept for the intervention emerged from an expert reference group that comprised palliative care physicians, nurses, educators, and researchers. The goal was to develop and test the effects of an intervention tailored to health professionals involved in EOL care, incorporating both mindfulness and compassion training. Existing programs (e.g., MBSR and MSC) are time-intensive programs usually involving up to eight, weekly, 2.5-hour sessions with 45–60 minutes of daily home practice. The reference group agreed that commitment would not be attractive to busy health professionals because in Australian health care settings, self-care activities are viewed as an individual responsibility with the expectation that they will be conducted outside work hours. 44 The factors that led to the development of the current tailored program were the reference group's remit to:
Identify a face-to-face and daily home practice commitment that were attractive to health professionals held either during work hours or at the end of their working day;
Incorporate both mindfulness and compassion training, with a focus on the cultivation of self-compassion, given documented positive correlations between mindfulness and self-compassion with measures of wellbeing23,45;
Ensure that the evidence base of the intervention and practices was communicated.
The reference group consensus was that six sessions would be acceptable to health professionals. The intervention was developed and facilitated by Kathryn Choules, an experienced mindfulness- and compassion-based program facilitator. The structure and content of the intervention drew upon existing interventions: MBSR, 27 CCT,28,46 and MSC. 29 The theoretical framework was informed by Gilbert's evolutionary, motivational model of compassion, which incorporates the three directional flows of compassion (toward others, from others, and self-compassion). 47 Gilbert conceptualizes compassion as an evolved and adaptive human capacity, which is underpinned by two different psychologies—engagement and action. 47 The pedagogy was reflective, interactive, and experiential. Formal and informal mindfulness and compassion practices were included for home practice. Formal practices included mindfulness and compassion meditations (e.g., body scan with affection). Informal practices included activities such as incorporating mindfulness into activities of daily living (e.g., mindful eating) and recording daily acts of kindness. Individuals committed to attending at least five sessions and to practicing the mindfulness and compassion meditations (15 minutes/day).
The intervention comprised six, weekly sessions, totaling seven hours, and included the following themes: Week 1: Introducing mindfulness and compassion; week 2: Exploring mindfulness and compassion; week 3: Receiving compassion: week 4: Self-compassion; week 5: Compassion for others, and week 6: Establishing a compassionate self. The format for the sessions generally was as follows (see Table 1 for detailed content):
Content of the Mindfulness-Based Compassion Training Intervention for Health Professionals Involved in End-of-Life Care
Optional videos and readings were available on the facilitator's website.
Opening meditation practice (e.g., body scan with affection);
Debrief of in-session practices and of home practice (mindful communication);
Mixed interactive and didactic presentation of core session principles (e.g., “compassion vs. empathy,” “three flows of compassion,” “common humanity”);
Group practice introducing new skill (e.g., loving kindness meditation);
Close.
The first and the last session were 90 minutes, with an additional 30 minutes for participants to complete the pre- and postquestionnaires, and sessions 1 to 4 were each 1 hour. Participants were provided with a home practice manual outlining the theory and research into mindfulness and compassion training in the health care context 48 and guided practices (web based). The intervention was delivered in October/November 2018 and in May/June 2019 to attract a range of health professionals.
Setting and participants
The inclusion criteria were health professionals involved in providing EOL care in a hospital (inpatient) or community setting (e.g., residential aged care facility; rehabilitation facility). Two screening questions were included to ensure that those who enrolled were involved in EOL care to some degree. Participants who indicated that they provided EOL care for any proportion of their time were eligible to enroll for the program.
Procedure
Health professionals enrolled through internal staff and professional networks of a public hospital and a not-for-profit (NFP) organization in Perth, Western Australia. The intervention was held: mid-afternoon on the hospital campus to coincide with the nursing shift changes and late afternoon at the NFP facility to coincide with the end of a standard work day. The questionnaires were distributed at the beginning of the first session and at the end of the final session. The final questionnaire was sent to participants in an e-mail attachment eight weeks postintervention. Ethics approval was obtained (HRE2018-0405).
Measures
The following scales were used to measure occupational burnout, compassion satisfaction, compassion fatigue, psychological distress, mindfulness, and self-compassion. These scales have been used previously among palliative care providers.4,49–53 See Table 4 for Cronbach's alpha for each subscale at Time 1.
The 22-item Maslach Burnout Inventory-Human Services Survey (MBI-HSS) 54 has 3 subscales that measure occupational burnout, including emotional exhaustion, depersonalization, and personal accomplishment. A total score is calculated for each scale. Higher scores for emotional exhaustion and depersonalization, and lower scores for personal accomplishment indicate higher levels of burnout. Internal reliability for the MBI-HSS scales is good with Cronbach's alpha at 0.90 for emotional exhaustion, 0.79 for depersonalization, and 0.71 for personal accomplishment. 54
The 30-item Professional Quality of Life Scale–Version 5 (ProQOL-5) 55 measures the quality of one's work as a “helper.” Three scales include compassion satisfaction, which is the pleasure one derives from doing one's work well, and the two components of compassion fatigue: secondary traumatic stress and burnout. A total score is calculated for each scale. Higher scores on secondary traumatic stress and burnout are suggestive of compassion fatigue. The instrument has been tested extensively with good reliability and validity. Cronbach's alphas are 0.88 for compassion satisfaction, 0.75 for burnout, and 0.81 for secondary traumatic stress. 55
The 21 items of the Depression, Anxiety, and Stress Scale (DASS-21) 56 are rated on a 4-point Likert scale with 3 subscales: depression, anxiety, and stress. The items within each subscale are summed and multiplied by 2 (given that the full scale has 42 items). Higher scores indicate greater distress. DASS-21 is a reliable and valid measure of the three constructs with high Cronbach's alphas at 0.94 for depression, 0.87 for anxiety, and 0.91 for stress. 57
The 12-item Self-Compassion Scale-Short Form (SCS-SF) 58 was developed from the longer 26-item SCS. 23 The internal consistency of the SCS-SF is high with Cronbach's alpha at 0.86, and the total score correlates strongly with the SCS total score (r ≥ 0.97). 58 The structure of the SCS-SF is identical to that of the SCS with a higher order self-compassion factor, and six subscales, corresponding to the six components of self-compassion 59 : self-kindness, common humanity, and mindfulness (positive) and self-judgment, isolation, and overidentification (negative). Participants respond to 12 statements using a 5-point scale ranging from 1 to 5 (“almost never” to “almost always”). The items are summed and a total mean is calculated (range = 1–5). A higher mean indicates greater self-compassion. 23
The 15-item Mindful Attention Awareness Scale (MAAS) 45 assesses dispositional mindfulness. Respondents are asked to indicate how frequently or infrequently they have experienced situations in daily life using a 6-point Likert scale ranging from 1 (almost always) to 6 (almost never). The scores are summed and a mean score is calculated, with higher scores reflecting higher levels of trait mindfulness. The scale is a reliable and valid measure of the construct of mindfulness with a Cronbach's alpha of 0.87. 45
Feasibility and acceptability of the workshop were assessed through:
Attendance: Participants signed in to each session;
Practice: Participants were asked to log the days they practiced the mindfulness/compassion meditation(s);
Satisfaction: Participants completed 16 items adapted from a previous feasibility trial. 60 For example: The content of the sessions was relevant to me. Responses were on a 5-point Likert scale (1—Not at all to 5—Very much). Three open questions assessed skills learned and areas for improvement.
Demographic information included: gender, country of birth, employment status, current position, duration in discipline, duration in current position, and prior training in mindfulness or compassion.
Analysis
The General Linear Mixed Model was used to analyze change over time. There were multiple comparisons for psychological distress, compassion fatigue, and occupational burnout. Therefore, the main effect for these outcomes was evaluated at the adjusted alpha level of 0.017 (0.05/3). Mean total scores were utilized for self-compassion and mindfulness, hence an alpha level of 0.05 was appropriate. Frequencies are reported for the feasibility and acceptability items. Responses to open questions were categorized by the main concepts represented. An a priori per-test alpha-level of 0.05, with a sample size of 31, provides sufficient power for an 80% chance of capturing a “moderate to large” (f = 0.24) time effect; meaning small changes across time may fail to reach statistical significance. However, a previous study utilizing MSC training among nurses from a hospital setting showed significant decreases in nurses' levels of compassion fatigue and increases in self-compassion and mindfulness postintervention, with large effect sizes. 31
Results
Sample characteristics
Thirty-one participants enrolled: 10 in the first intervention (9 females, 1 male) and 21 in the second (all female). The mean age of participants was 42.3 years (SD = 13.1). Mean time in discipline was 11.5 years (SD = 10.4) and mean time in current position was 4.9 years (SD = 3.8). Eighty-four percent of participants were employed in a hospital setting and 32% of participants reported spending at least half of their time involved in EOL care. All participants completed the Time 1 measures, and 26 participants (84%) completed the remaining questionnaires. Data for all participants who enrolled were analyzed (Table 2).
Sample Characteristics (N = 31)
Data for all participants who enrolled in the intervention are presented.
Feasibility and acceptability
Attendance and practice
Seventy-seven percent of participants completed five or more sessions. Five participants (16%) completed three or fewer sessions. Twenty-three participants (74%) returned a completed practice log with their questionnaire at Time 2.
Satisfaction
The majority of participants agreed “much or very much” with statements that the sessions were useful, relevant, easy to understand, met their needs, and gave them sufficient knowledge to implement the strategies introduced (Table 3). All participants reported that learning about the benefits of compassion, and how to cultivate it, was helpful.
Frequencies for the Items Assessing the Feasibility and Acceptability of the Six Sessions (N = 26)
Of the participants who responded to the open-ended items on the questionnaire (n = 24), the top 3 skills they reported they would use from the sessions were:
Compassion techniques, especially fostering self-compassion (71%);
Guided meditations and mindfulness techniques, for example, body scan, practicing being in the present moment, awareness of self, pausing to check in with the body, and nonjudgmental stance (63%);
The concept of common humanity (25%).
Several potential improvements for the sessions were identified:
More time in each session (29%);
Ongoing compassion training sessions for other hospital staff (13%);
Use a location with better acoustics; include EOL case examples; receive instruction on how to teach others mindfulness techniques, and audiorecord the sessions (17%).
Significant effects at pre, post, and follow-up
Table 4 presents the descriptive and inferential statistics for the outcome variables. There was a significant main effect for time for: anxiety (Fig. 1), compassion fatigue [burnout only] (Fig. 2), compassion satisfaction (Fig. 3), emotional exhaustion (Fig. 4), and self-compassion (Fig. 5).
Cronbach's Alpha, Means, Standard Deviations, Confidence Intervals, F Values and Degrees of Freedom for the Outcome Variables
CI, confidence interval; DASS, Depression, Anxiety, and Stress Scale; MAAS, Mindful Attention Awareness Scale; MBI-HSS, Maslach Burnout Inventory–Human Services Survey for Medical Personnel; ProQOL, Professional Quality-of-Life Scale Version 5; SCS-Short, Self-Compassion Scale (Short); SD, standard deviation. *p < 0.05; **p < 0.017 (adjusted); ***p < 0.001.
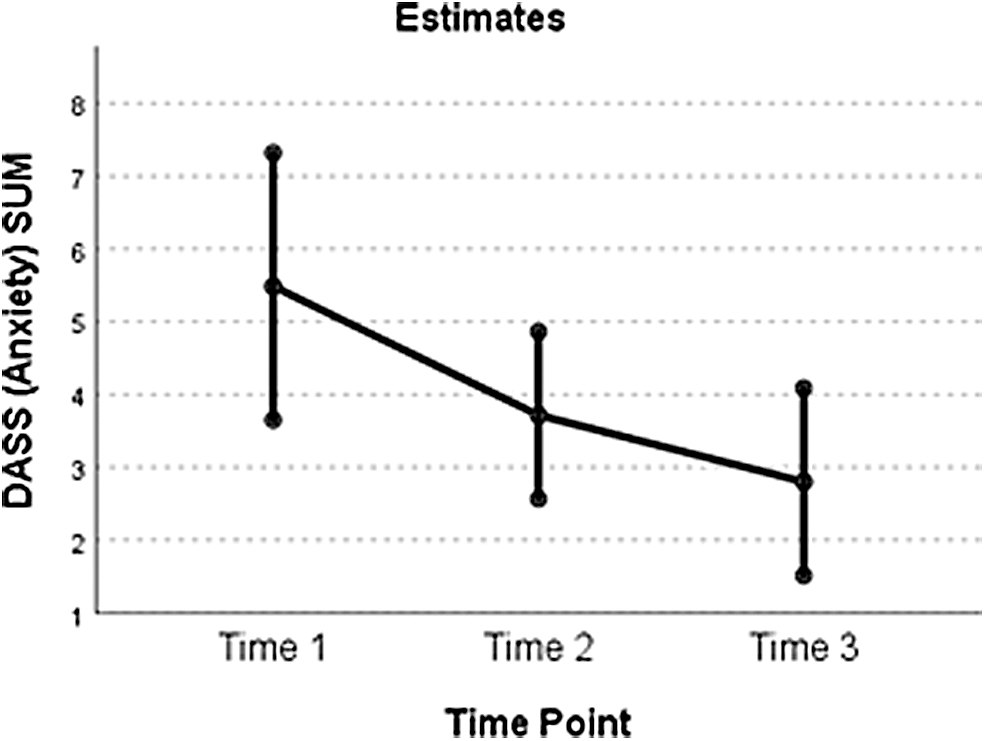
A plot of the main effect of time for anxiety.
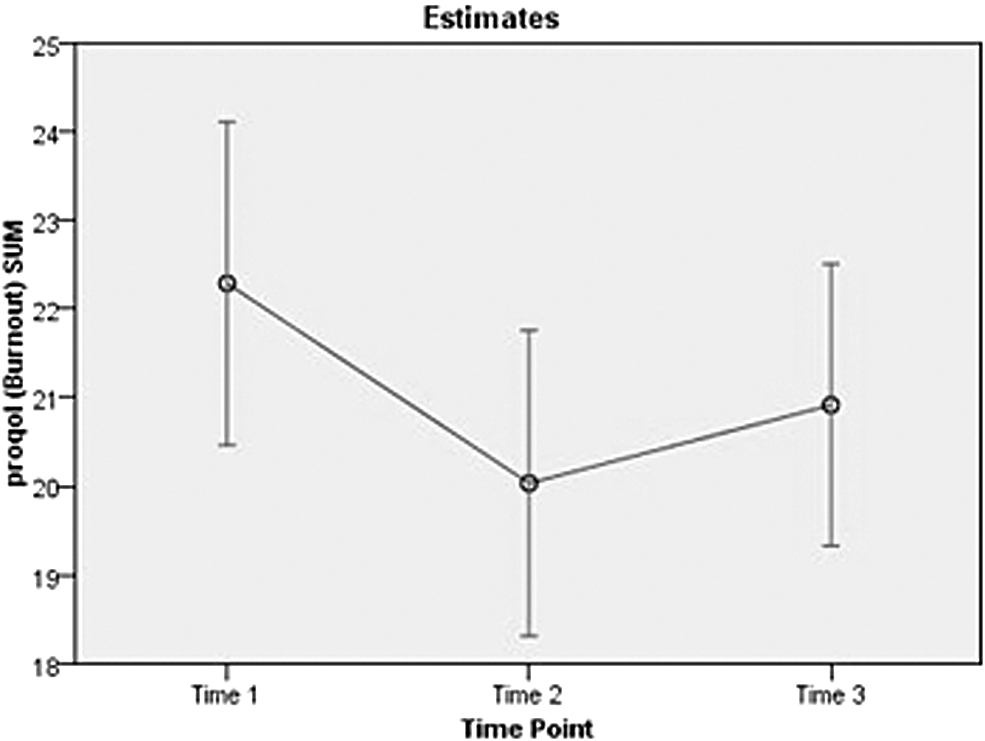
A plot of the main effect of time for compassion fatigue (burnout).

A plot of the main effect of time for compassion satisfaction.
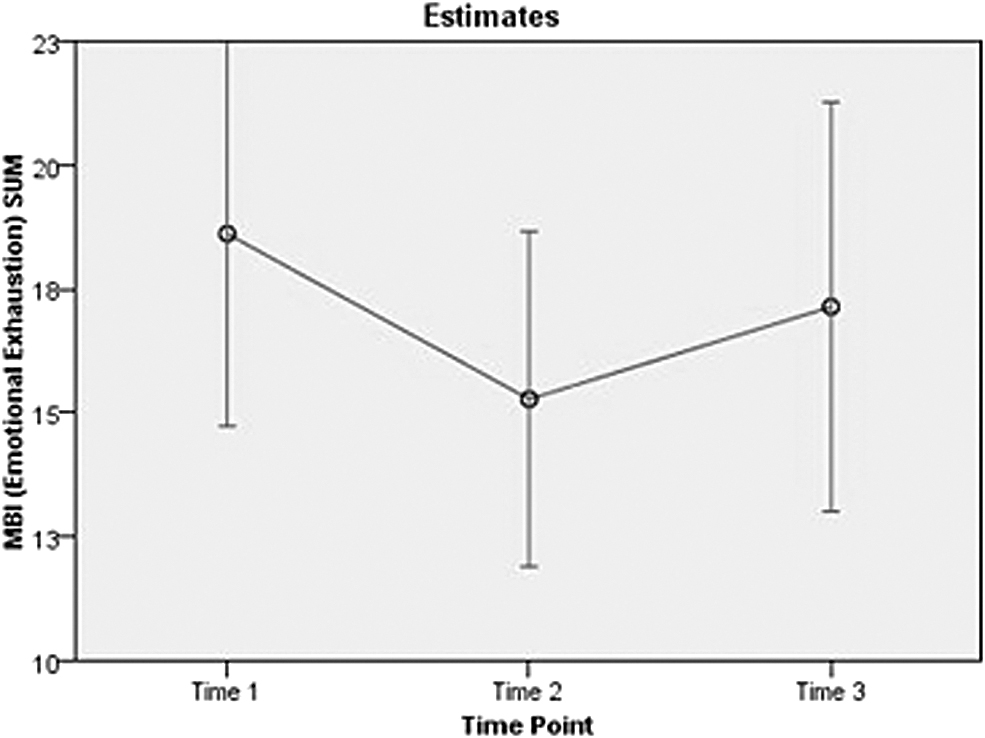
A plot of the main effect of time for emotional exhaustion.
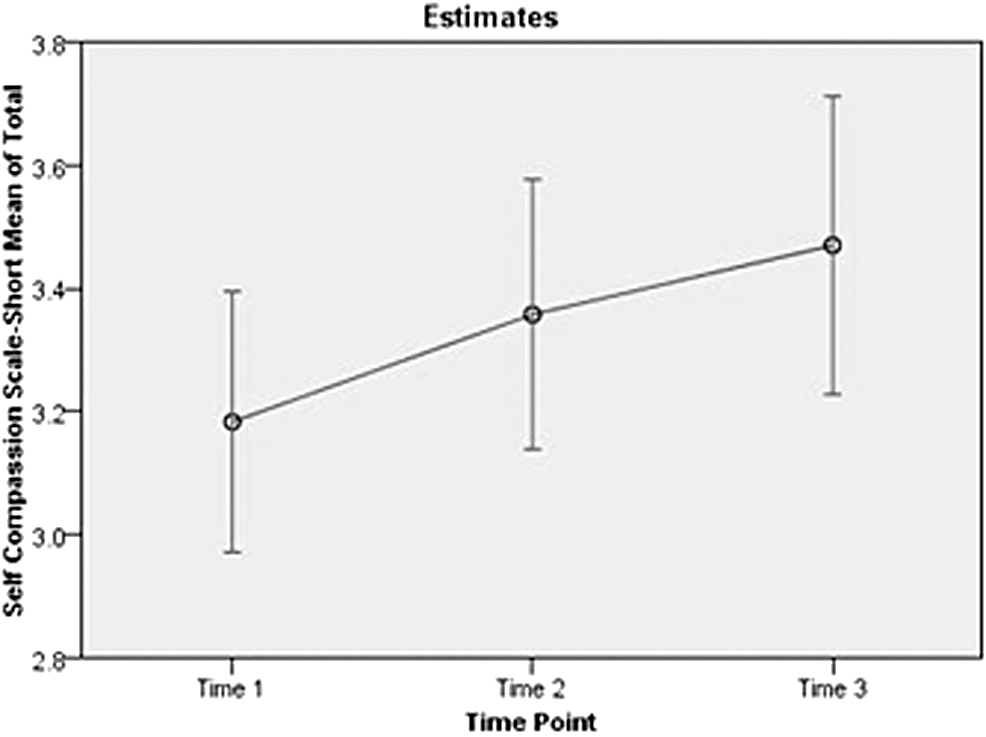
A plot of the main effect of time for self-compassion.
Anxiety
Least significant difference (LSD) comparisons indicated a significant decrease between Time 1 and Time 3 (t[80] = 3.31, p = 0.001), but no significant change between Time 1 and Time 2 (t[80] = 1.76, p = 0.083), and between Time 2 and Time 3 (t[80] = 1.42, p = 0.161).
Compassion fatigue (burnout)
LSD comparisons indicated a significant decrease between Time 1 and Time 2 (t[80] = 3.89, p < 0.001), and between Time 1 and Time 3 (t[80] = 2.21, p = 0.030). There was a significant increase between Time 2 and Time 3 (t[80] = 2.20, p = 0.031).
Compassion satisfaction
LSD comparisons indicated a significant increase between Time 1 and Time 2 (t[80] = 3.40, p = 0.001), and between Time 1 and Time 3 (t[80] = 2.04, p = 0.045). There was no significant change between Time 2 and Time 3 (t[80] = 0.84, p = 0.404).
Emotional exhaustion
LSD comparisons indicated a significant decrease between Time 1 and Time 2 (t[80] = 2.82, p = 0.006), and a significant increase between Time 2 and Time 3 (t[80] = 2.16, p = 0.034). There was no significant change between Time 1 and Time 3 (t[80] = 1.14, p = 0.256).
Self-compassion
LSD comparisons indicated a significant increase between Time 1 and Time 3 (t[80] = 2.61, p = 0.011), but no significant change between Time 1 and Time 2 (t[80] = 1.53, p = 0.129) or between Time 2 and Time 3 (t[80] = 1.56, p = 0.126).
Nonsignificant effects at pre, post, and follow-up
The main effect for time was not significant for: depression, stress, compassion fatigue (secondary traumatic stress), depersonalization, personal accomplishment, or mindfulness.
Discussion
This pilot study tested the feasibility and acceptability of a novel six-week mindfulness-based compassion intervention designed to foster mindfulness, and compassion for self and others. 48 The intervention's impact upon psychological distress, occupational burnout, compassion fatigue, compassion satisfaction, self-compassion, and mindfulness among health professionals involved in EOL care was measured.
Participants highly valued the compassion and mindfulness skills and knowledge learned, which likely supported ongoing participation. Previous research has acknowledged the time pressures faced by health professionals 61 and the challenges involved in committing to weekly interventions. 33 It is noteworthy that 77% of health professionals completed five or more sessions of the MBCT4HP, which is comparable to attendance or compliance rates (70%–88%) for health care workers attending other mindfulness-based interventions.40,41 However, approximately half of the participants reported it was challenging to attend all six sessions and to do the daily practice. MBCT4HP has recently been adapted to provide the option of online completion, and preliminary reports suggest high levels of acceptability for this format especially among a subgroup of health care providers such as specialist consultants with very limited time. Questions have been raised about the minimum effective dose for mindfulness-based compassion interventions.33,62 In this pilot, the six weeks duration produced positive results.
As hypothesized, levels of self-compassion increased. This finding is consistent with studies in which levels of self-compassion among nurses and other health professionals increased significantly following compassion-focused therapy 32 and a MSC intervention. 31 Higher levels of self-compassion are associated with lower levels of depression, anxiety, and stress. 22 Also, cultivating a kind, nonjudgmental, and respectful attitude toward oneself facilitates one's capacity to have this attitude toward others, 59 thus enhancing the likelihood of health professionals' engaging in compassionate care. 63 There was a nonsignificant trend for mindfulness levels to increase postintervention and at follow-up.
Levels of compassion fatigue (burnout) decreased (but with an increase between Time 2 and Time 3) and levels of compassion satisfaction increased postintervention. This pattern of findings is consistent with decreases in compassion fatigue among nurses following an MSC program. 31 Levels of secondary traumatic stress, which is distress that arises due to exposure to others' trauma and suffering, 55 decreased following MBCT4HP, but this did not reach significance. Levels of this variable were low at Time 1, so floor effects may have operated or the study may not have had sufficient power to detect a small effect. Levels of compassion satisfaction increased significantly postintervention; this is the pleasure one derives from doing one's work well. 55 MBCT4HP was designed to foster compassion, including self-compassion. The key elements of self-compassion (self-kindness, mindfulness, and common humanity) 23 are positively correlated with compassion satisfaction 64 and negatively associated with compassion fatigue. Self-compassion, which includes a reduced tendency toward harsh self-judgments and self-criticism,23,32 may facilitate mental spaciousness and assist health professionals to experience more pleasure and satisfaction in their work, thus functioning as a protective factor against compassion fatigue.31,64
The current sample scored above average on the personal accomplishment scale at baseline, which was comparable to the levels reported previously for doctors involved in providing palliative care, 65 making it difficult to observe a change from a brief intervention. The initial decrease in level of emotional exhaustion and in level of compassion fatigue (burnout) were not sustained at follow-up. The decay in these effects may have arisen because some participants may not have continued their daily practice beyond the intervention, and this is likely to be necessary for effects to be sustained. Moreover, in a previous study of occupational burnout among hospital and palliative care clinicians, a substantially larger proportion experienced high emotional exhaustion compared with high depersonalization (34.8% vs. 8.8%). Significant predictors of burnout in that sample were being in a nonphysician clinical role (e.g., a registered nurse or a social worker), working more than 50 hours per week, working weekends, and working with fewer colleagues. 4 Similarly, higher hours of patient contact per week is positively associated with secondary traumatic stress. 20
Overall, participants at preintervention scored in the low-to-normal range on the measures of psychological distress, compassion fatigue, and occupational burnout, and the absence of significant changes for some of the subscales postintervention may relate to floor effects. 35 Given increasing pressures on health care and health professionals and scarce health resources, future research may need to target MBCT4HP to health professionals at elevated risk of burnout and psychological distress. Targeting MBCT4HP to at-risk health professionals could form part of health care workplace strategies to build employee resilience and wellbeing. 66 For example, in their call for action on clinician burnout, the United States National Academy of Medicine highlights that health professionals' wellbeing is not solely the responsibility of the individual, and it calls for a systems-level approach. 67 This requires a positive organizational culture that prioritizes the wellbeing and safety of health care workers, including listening to clinicians' needs, adequately resourcing the workforce, and providing wellness programs and leadership that promote clinicians' wellbeing, safety, and resilience. 68 Optimally, programs such as MBCT4HP would be provided or sponsored by health care workplaces with the overarching goal of supporting health professionals' wellbeing, 66 and so that the burden of fostering self-care practices among health professionals is a shared responsibility between the workplace and the individual. 66
Future Research
A randomized controlled trial (RCT) testing the impact of MBCT4HP with a wait-list control group is warranted, including testing for potential mechanisms of impact (e.g., the role of self-compassion and mindfulness as mediators of emotion regulation and worry 69 ). Any RCT of MBCT4HP should include a longer follow-up and examine whether participants continue their compassion techniques postintervention and how this influences impact. Screening health professionals for compassion fatigue, occupational burnout, and high patient contact hours, and then targeting MBCT4HP as a preventative measure to those at-risk 70 will optimize use of scarce health resources.
Limitations
This was a pilot study with a small sample, and power to detect small effects may have been insufficient. Self-report measures are subject to response bias. However, reliable objective measures in this field are difficult to find. 41 Self-selected individuals interested in compassion may have been more likely to enroll. The sample was predominantly female, also limiting generalizability. However, females are typically overrepresented in the palliative care workforce.4,41 The participants were engaged, in varying degrees, in EOL, and palliative care. Results may be different for health professionals whose roles are wholly within palliative care. We assessed acceptability and feasibility using behavioral measures and self-report satisfaction items, which are widely used methods for assessing acceptability. However, we did not specify a threshold criterion, 71 for example, defining the proportion of participants needed to complete at least five sessions for the intervention to be considered acceptable. Future research should consider including such a threshold.
Conclusions
The findings suggest that the six weekly sessions were acceptable, feasible, and valued by health professionals involved in EOL care, with positive effects on anxiety, self-compassion, compassion satisfaction, and compassion fatigue.
Footnotes
Acknowledgments
The researchers are grateful for the commitment and participation of the health professionals in this program. The authors thank Rachel Cappeau and Jacky Woods for their excellent administrative support and efforts throughout recruitment and during data collection.
Funding Information
This project was funded by a grant from the Royal Perth Hospital Medical Research Foundation on which Kevin Yuen was the Chief Investigator, and coauthors Moira O'Connor, Claire E. Johnson, Lauren J. Breen, and Claire Doyle were Associate Investigators. Author Kathryn Choules developed and facilitated MBCT4HP and Grace Buchanan is a director at the not-for-profit organization referred to in the article.
Author Disclosure Statement
No competing financial interests exist.