
Abstract
Background:
Despite the suggestion of a relationship between development or progression of myofascial pain syndrome (MPS) and psychological stress, few studies have reported its proportion or association with treatment efficacy.
Objective:
We aimed to investigate the proportion of MPS with psychological stress among cancer patients and to compare the efficacy of trigger point injection (TPI) in the same patients with/without psychological stress.
Design:
This was a prospective observational study.
Setting/Patients:
Participants were 205 patients with cancer who received TPIs for MPS at a hospital in Japan.
Results:
The proportion of patients with MPS and psychological stress was 0.57 (95% confidence interval [CI] 0.50–0.64). The TPI efficacy rate at seven days after treatment was 0.55 (95% CI 0.46–0.64) for patients with MPS and psychological stress and 0.82 (95% CI 0.74–0.90) for their counterparts without psychological stress (p < 0.004). The odds ratio for TPI efficacy seven days after treatment with psychological stress versus without psychological stress was 0.25 (95% CI 0.13–0.49).
Conclusions:
MPS was a clinical symptom of psychosomatic disorder in approximately half of our patients. The TPI efficacy for patients with MPS who had psychological stress was lower than for their counterparts without psychological stress. Trial registration: UMIN000041210. Registered 27 July 2020 (retrospectively registered).
Introduction
According to the U.S. Centers for Disease Control and Prevention, the three main conditions that cause daily life disability are heart disease, arthritis, and chronic back pain. 1 Of patients with cancer, 31% to 45% complain of chronic back pain and experience myofascial pain syndrome (MPS).2,3 MPS is diagnosed according to the following criteria: (1) a tender spot found on palpation, with or without referral of pain; (2) recognition of pain symptoms by the patient on palpation of a tender spot; and at least three of the following; (3) muscle stiffness or spasm; (4) limited range of motion of an associated joint; (5) pain that worsens with stress; and (6) palpation of a taut band and/or nodule associated with a tender spot. 4 It is known that physical and psychological stress are associated with chronic back pain, but the causal relationship, mechanisms, and mediators of this association have not been elucidated.5,6
The relationship between physical stress and MPS is characterized by continuous muscle tension owing to limited body posture or remaining in the same position, and muscle overload owing to repetitive motions.7–9 In one study, 64% of advanced cancer patients had cancer pain together with MPS at the pain site of chief complaint, suggesting a relationship between muscle load and flight response from pain. 2 Another study reported MPS caused by physical stress at the breast cancer postoperative site. 10
The relationship between psychological stress and MPS has been investigated in vivo using a preclinical model, which identified aspects of psychological stress-induced pain exacerbation. 5 Rivers et al. include criterion (5) mentioned above (pain worsens with stress) as an MPS diagnostic criterion. 4 Few clinical reports on MPS have examined its relationship with psychological stress and emotional distress.11,12 There is evidence that 32.0% of individuals with MPS have psychological stress owing to temporomandibular disorders. In one study, the mean distress thermometer value was 4.7 (standard deviation [SD] 2.9) in the MPS group and 2.7 (SD 2.7) in the control group. MPS is associated with psychological factors, such as anger, anxiety, disturbed sleep, and depression.11–14
Patients with cancer experience a high frequency and severity of psychological stress and emotional distress across many cancer stages.15–18 There is no consistent definition and measure of psychological stress, but is has been described in terms of self-reported stress, psychosocial stress, major life events, depression, and mental disorders.11,18–20 Emotional distress is poorly differentiated from psychological stress and often assessed using validated rapid-screening instruments (e.g., the distress thermometer) in cancer patients.15–17,21
Psychological stress affects cancer patients' immune response and cancer progression19,22 and is associated with neuroendocrine alterations, which can upregulate inflammation and downregulate cell-mediated immunity. Immune cells that have undergone such changes may not control cancer cells effectively. 19 Autonomic innervation of tumors regulates breast cancer progression, suggesting that stress-induced sympathetic nervous tension may promote cancer. 22 However, to the best of our knowledge, no studies have investigated the association between MPS, psychological stress, emotional distress, and other psychological factors in cancer patients. It is important to determine the relationship between MPS and psychological stress in these patients.
The standard treatment of medication for MPS remains controversial. 23 There are no reports demonstrating the efficacy of analgesic medication, such as opioids, for MPS. Administration of opioids for MPS in cancer patients can lead to effects like delirium. 24 Topical MPS treatments include trigger point injection (TPI), needling, sprays, stretching, and massage.25,26 Of the invasive therapies, TPI is the most commonly used technique. 27 The effects of TPI have been demonstrated at a molecular level. 28 Our previous study indicated a TPI efficacy rate of 59% the day after TPI treatment for MPS in cancer patients. 2 The factor most closely related to TPI efficacy was MPS of the upper back (odds ratio [OR] 6.45, confidence interval [CI] 1.98–21.0), suggesting a relationship with physical stress. No reports have elucidated the relationship between TPI efficacy for MPS in cancer patients with psychological stress. Therefore, we examined the relationship between TPI efficacy and psychological stress. The findings may help to improve the efficacy of TPI treatment for MPS in cancer patients.
Methods
Objective
We aimed to investigate the proportion of cancer patients with MPS who also had psychological stress, and to calculate the ORs of TPI efficacy for patients with/without psychological stress.
Study design
This was a prospective observational study conducted in Osaka, western Japan. The following demographic information was obtained: gender, age, primary cancer site, medical treatments, Eastern Cooperative Oncology Group performance status (ECOG PS), MPS site, number of MPS sites, analgesic drug use, presence of MPS with and without psychological stress, and measures of pain intensity immediately before and one, three, and seven days after TPI treatment. Two doctors specializing in palliative care with more than 15 years experience diagnosed MPS and performed TPI. We defined the upper back as the region below the neck and above the costal margin, following a previous study that defined the lower back (including the buttocks) as the region below the costal margin and above the inferior gluteal folds. 29 This study was conducted in accordance with the Declaration of Helsinki and received approval from the Medical Ethics Committee of Kansai Medical University (Reference No.: 2018123).
Outcomes
The primary endpoint was the OR of TPI efficacy seven days after TPI treatment in cancer patients, with/without psychological stress. The secondary endpoint was the proportion of cancer patients with MPS who also had psychological stress.
Study participants
This study was conducted from 2018 to 2020 at the Kansai Medical University Hospital. During this period, 1176 patients with cancer who visited the palliative care department were continuously enrolled in the study. Of these, 394 had MPS (33.5%) and 231 received TPI for MPS. Of these 231, 205 were selected as participants, after excluding 26 patients who met the following exclusion criteria: (1) younger than age 20 years (n = 3) and (2) any comorbidity related to psychiatric diseases or conditions that made communication difficult, such as cognitive impairment or delirium (n = 23).
Criteria for diagnosis of MPS with/without psychological stress
MPS was diagnosed according to the reference diagnostic criteria of Rivers et al. 4 The determination of trigger points requires careful manual examination, which is considered highly reliable. 30 Palpation of MPS was not routinely performed, except on the day of diagnosis. We determined the presence or absence of MPS with psychological stress according to whether or not criterion (5) as above (pain worsens with stress) was met. 4 The doctors determined this by asking, “Does your MPS pain worsen with stress?”
Assessment of pain intensity
The average pain intensity during the previous 24 hours was determined using a numerical rating scale (NRS) ranging from 0 (no pain) to 10 (worst possible pain). 31 Participants completed a questionnaire with an NRS immediately before and one, three, and seven days after TPI treatment. The reliability and validity of this scale have been established. 32 For multiple MPS with different NRS scores, the average NRS score was used.
TPI efficacy rate
The TPI efficacy rate was calculated as the rate of patients with ≥33% improvement in NRS scores after TPI treatment. 33 TPI was applied to all MPS observed. For the TPI treatment, 1 mL of 1% lidocaine was injected into each pain site using a 27 G, 19 mm needle.
Sample size calculation
The sample size required to detect a minimum TPI efficacy rate difference of 0.15 (SD 0.10) between the two groups was 186, estimated according to published data. As there are no data on TPI efficacy at seven days after TPI treatment for cancer patients, data for one day after TPI treatment were used (2). The significance was set at 0.05 and the power set at 80%.
Statistical analysis
Data were reported as mean with SD, median with 95% CI, or frequency (%), as appropriate. We estimated the proportion of cancer patients with MPS and psychological stress among all patients with MPS who received TPI, as well as the TPI efficacy rate, using the exact 95% CI based on the binomial distribution.
Participants were classified into two groups: patients with MPS and psychological stress and patients with MPS without psychological stress. We used unpaired t-tests to compare the following dependent variables among patients with/without psychological stress: age, number of MPS sites, and NRS score (treatment day: day 0). We used Pearson's chi-square tests to analyze the dependent variables' gender, medical treatments, ECOG PS, MPS site, and analgesic drug use.
We determined the ORs of TPI efficacy seven days after TPI treatment in patients with/without psychological stress. We analyzed changes in average NRS score (days 0, 1, 3, and 7) using one-way repeated measures analysis of variance (ANOVA) for each group. To conduct between-group comparisons, we used time course as the within-patient factor and group as the between-patient factor in two-way repeated measures ANOVA. In the ANOVA, multiple comparisons were corrected using the Bonferroni method. When a participant withdrew from the study, the average NRS after withdrawal was substituted with the score immediately before withdrawal. Analgesic drug changes during the period were considered withdrawal from the study.
Spearman's rank correlation coefficients were calculated to assess associations between TPI efficacy seven days after TPI treatment and age, medical treatments, ECOG PS, MPS site, number of MPS sites, NRS score (day 0), analgesic drug use, and MPS with psychological stress. In addition, multivariable logistic regression analysis was performed with the dependent variable of TPI efficacy seven days after TPI treatment and six independent variables: age, MPS site (lower back), number of MPS sites, NRS score (day 0), analgesic drug use, and MPS with psychological stress.
A p < 0.05 was considered statistically significant. We used IBM SPSS version 25.0 for Macintosh (IBM Corp., Armonk, NY) for statistical analysis.
Results
Of patients with MPS, the proportion who had psychological stress was 0.57 (95% CI 0.50–0.64). Based on the diagnostic criteria for MPS with/without psychological stress, participants were classified into a psychological stress group (n = 117) and control group (n = 88). Table 1 shows the demographic and clinical characteristics of both groups. The mean (SD) for age and NRS score (day 0) were 67.6 (12.1) years and 6.1 (2.4) points, respectively. Figure 1 shows the MPS site (dots). Analgesic drug changes during the period were observed in 11 (5.4%) participants.

The MPS site (dots). MPS, myofascial pain syndrome.
Comparison of Clinical Characteristics in Patients with Myofascial Pain Syndrome with and without Psychological Stress
Dose of opioids is expressed as oral dose level of morphine (mg/dL). For conversion: parenteral morphine: oral morphine = 1:2, parenteral, oxycodone: oral morphine = 1:2, oral oxycodone: oral morphine = 2:3, fentanyl: morphine = 1:100, oral methadone: oral morphine = 1:8.
BSC, best supportive care; ECOG, Eastern Cooperative Oncology Group; IQR, interquartile range; MPS, myofascial pain syndrome; NRS, numerical rating scale; PS, performance status; SD, standard deviation.
NRS scores in both groups were significantly lower at one, three, and seven days after TPI treatment compared with baseline (p < 0.001). A between-group comparison of NRS scores showed a significant interaction between time course and group (p = 0.012). There was also a significant between-group difference in time course (day 0, p = 0.186; day 1, p < 0.001; day 3, p < 0.001; and day 7, p < 0.001) (Fig. 2). The TPI efficacy rate at seven days after treatment was 0.66 (95% CI 0.60–0.72). The TPI efficacy rate seven days after treatment was 0.55 (95% CI 0.46–0.64) in the group with MPS and psychological stress and 0.82 (95% CI 0.74–0.90) in the group with MPS without psychological stress (p < 0.004). No adverse events occurred during any TPI treatments performed throughout the evaluation period.
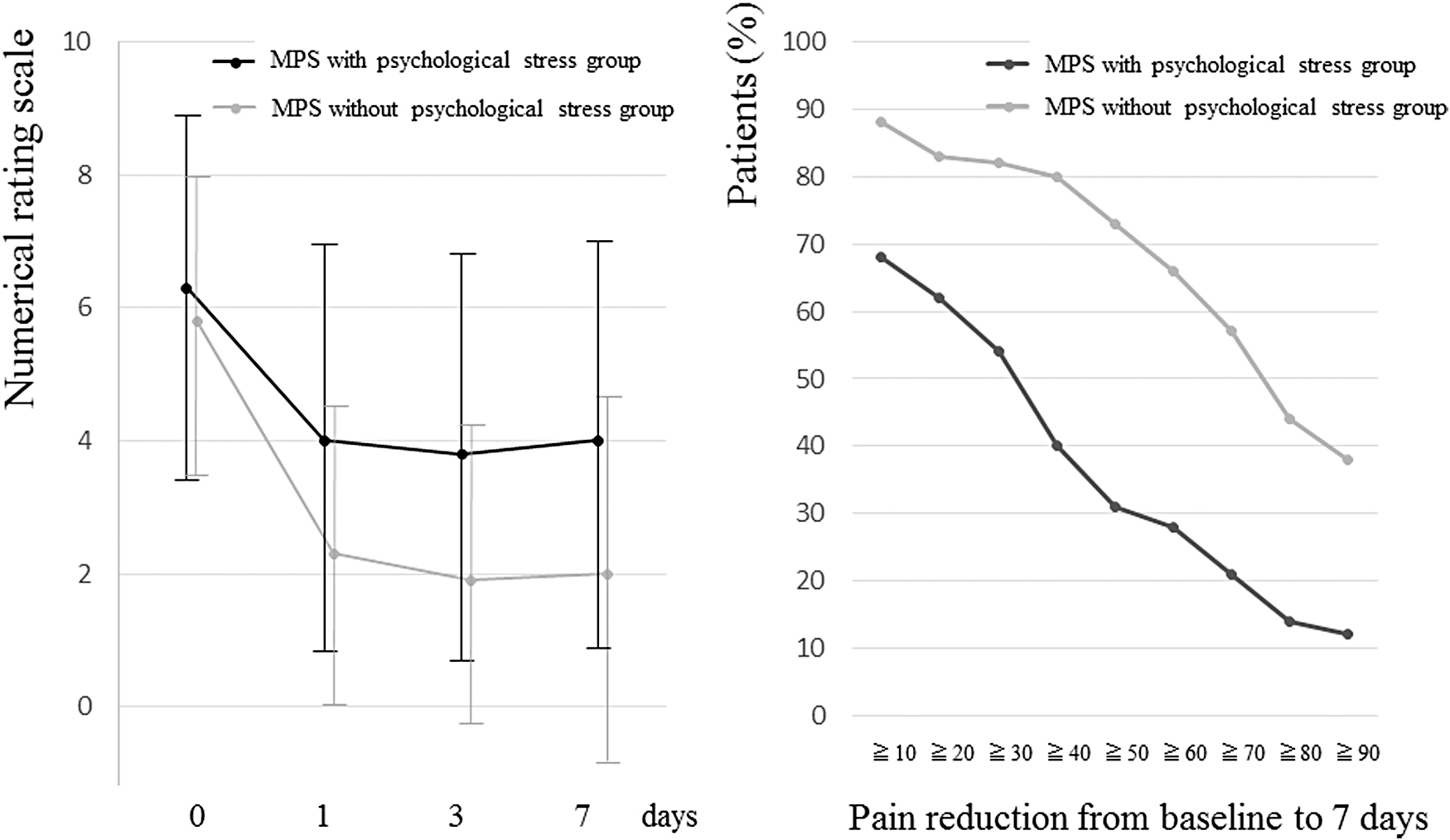
Average NRS scores of patients with myofascial pain syndrome and percentage of patients with pain reduction before and after trigger point injection treatment. CI, confidence interval; NRS, numerical rating scale; OR, odds ratio; SE, standard error.
Table 2 shows the Pearson's correlations between the following variables: medical treatments, ECOG PS, MPS site, number of MPS sites, NRS score (day 0), analgesic drug use, MPS with psychological stress, and TPI efficacy seven days after treatment. MPS with psychological stress was not significantly correlated with any variables except TPI efficacy.
Correlation Coefficient between Trigger Point Injection Efficacy and Other Variables
p < 0.05.
p < 0.01.
p < 0.001.
TPI, trigger point injection.
The multivariable logistic regression analysis identified two factors associated with TPI efficacy seven days after treatment: MPS with psychological stress (OR: 0.25, 95% CI 0.13–0.49) and lower back MPS site (OR: 0.37, 95% CI 0.19–0.72) (Table 3).
Factors Associated with Trigger Point Injection Efficacy 7 Days after Treatment
CI, confidence interval; OR, odds ratio; SE, standard error.
Discussion
This is the first report on the proportion of cancer patients who have MPS together with psychological stress, and the relationship between psychological stress and TPI efficacy. The upper back was a common MPS site, and PS tended to be 0 to 2 in the upper back. Reported pain severity was moderate among cancer patients 34 (average NRS score: 6.1). MPS was observed in 33.5% of our patients, approximately the same percentage as reported in previous studies.2,3 Despite a comparatively high TPI efficacy rate seven days after TPI treatment (0.66), we were unable to compare our results with previous findings owing to a lack of related studies of cancer patients. The efficacy rate one day after TPI treatment was 0.60, similar to the 0.59 reported in a previous study. 2
We began by determining the proportion of cancer patients who had MPS and psychological stress among all our patients with MPS. Although there are a few reports of coexisting MPS and psychological stress,11,12 none has evaluated the effect of psychological stress on MPS pain intensity. A psychosomatic disease is defined as any physical condition with organic or functional factors that is affected by psychological factors during its onset or development. 35 MPS, which is a functional disorder, was a clinical symptom of psychosomatic disorder in more than half of our patients. Patients with cancer experience a high frequency and severity of psychological stress.15,16 In cases where stress produces increased pain, only psychological factors tend to be considered. This highlights the importance of medical practitioners assessing both functional and psychological factors when MPS as a clinical symptom of psychosomatic disorder is suspected upon clinical examination of a cancer patient with increased pain owing to stress.
Some patients with psychosomatic disorders show alexithymia, a condition involving difficulty with awareness of emotions and bodily sensations.36,37 Alexithymia can increase somatic symptoms, such as cancer pain, in cancer patients38,39 and is correlated with MPS and latent trigger points.12,40 One study found a negative correlation between subjective physical tension and objective physiological indices of stress in patients with psychosomatic disorders. 41 A constant strong feeling of tension leads to inhibited awareness of a feeling of relaxation. This dissociation indicates that patients with psychosomatic disorders have difficulty with awareness of their bodily feelings. 41 We suggest that difficulty with body awareness tends to lead to inhibited awareness of myofascial hypertonia as a danger signal in cancer patients, which can result in trigger point formation and aggravation.
We secondarily identified a relationship between TPI efficacy for MPS in cancer patients and psychological stress. The OR of MPS with psychological stress was lowest among those factors affecting TPI efficacy at seven days after treatment. Compared with TPI for MPS without psychological stress, the probability of TPI efficacy for MPS with psychological stress was low (OR 0.25). The OR for lower back site of MPS was also low, suggesting a relationship with physical stress; this finding is in line with that of our previous study. 2
One placebo-controlled study showed no clear effect of TPI for chronic nonmalignant MPS. 25 In the present study, a large and significant difference was observed in TPI efficacy rate at seven days after treatment between MPS cases with and without psychological stress (0.55 and 0.82, respectively). In patients with MPS without psychological stress, a placebo-controlled study is more likely to detect a significant effect of TPI on functional factors, which are the main factors. However, the precise mechanism by which TPI inactivates MPS remains unknown. It is difficult to ascertain this from the present findings alone, because the TPI effect may also be affected by etiologies other than psychological stress, such as molecular effects and MPS history.
An approach that considers both functional and psychological factors is needed in patients with MPS who have psychological stress. TPI treatment is indicated to address functional factors in these patients. NRS scores of the group with MPS and psychological stress reduced by 2 points or more at seven days post-treatment. A 2-point change is generally regarded as the minimal clinically important difference in chronic pain. 42 Psychosocial approaches to pain in cancer patients, such as behavioral psychosomatic medicine approaches (e.g., biofeedback therapy, mindfulness meditation, relaxation), are recommended. 43 One randomized controlled trial indicated the efficacy of biofeedback therapy for MPS in cancer patients. 44
Our study has several limitations. First, patient selection was biased. Participants were cancer patients who visited the palliative care department; therefore, our findings are not generalizable to all cancer patients. There was also evaluation bias, because this was not a blinded trial. Second, because this was an observational study, the history of MPS and psychological stress was not investigated, and the interaction and causal relationship between them remain unknown. Third, the existence of MPS with psychological stress was determined using self-reported assessment of whether pain worsened with stress, without observation of time-dependent changes in stress and distress. However, a precise subjective assessment may have been difficult because of the presence of alexithymia.36,37 Finally, as participants were cancer patients who visited the palliative care department, only acute efficacy up to seven days after TPI treatment was evaluated and long-term effects were not assessed.
Conclusions
MPS was identified as a clinical symptom of psychosomatic disorder in approximately half of our cancer patients. TPI efficacy in patients with MPS who had psychological stress was lower compared with their counterparts without psychological stress. An approach that considers both functional and psychological factors is needed for patients with both MPS and psychological stress. We plan to conduct a prospective cohort study to follow the course of MPS development in patients with psychological stress and/or alexithymia.
Footnotes
Acknowledgments
Funding Information
The work was not supported by any external funding.
Author Disclosure Statement
No competing financial interests exist.