
Abstract
Background:
There is paucity of data on the potential value of early palliative home care for patients with hematologic malignancies.
Objective:
To compare costs, use of resources, and clinical outcomes between an early palliative home care program and standard hospital care for active-advanced or terminal phase patients.
Patients and Methods:
In this real-life, nonrandomized comparative study, the allocation of advanced/terminal phase patients to either home or hospital was based on pragmatic considerations. Analysis focused on resources use, events requiring blood unit transfusions or parenteral therapy, patient-reported symptom burden, mean weekly cost of care (MWC), cost-minimization difference, and incremental cost-effectiveness ratio (ICER).
Results:
Of 119 patients, 59 patients cared at home were more debilitated and had a shorter survival than the 60 in hospital group (p = 0.001). Nevertheless, symptom burden was similar in both groups. At home the mean weekly number of transfusions (1.45) was lower than that at hospital (2.77). Higher rate of infections occurred at hospital (54%) versus home (21%; <0.001). MWC for hospitalization was significantly higher in a 3:1 ratio versus home care. Compared with hospital, domiciliary assistance produced a weekly saving of € 2314.9 for the health provider, with a charge of € 85.9 for the family, and was cost-effective by an ICER of € −7013.9 of prevented days of care for avoided infections.
Conclusions:
Current findings suggest that costs of early palliative home care for patients with hematologic malignancies are lower than standard hospital care costs. Domiciliary assistance may also be cost-effective by reducing the number of days to treat infections.
Introduction
Home care may be associated with a number of advantages over hospital care across various medical conditions. In particular, cost and cost-effectiveness studies have suggested that home care may be an efficient service by reducing both the inappropriate use of available hospital beds and the unit cost of care provision, when compared with conventional medical beds, both for patients in the terminal phase of their cancer disease and during active anticancer treatment.1–5
Malignant hematology represents a clinical setting in which home care assistance may play an important role in patients' care, during different phases of their clinical history.5,6
Critical aspects of early palliative home care program for hematologic patients include symptom control, psychosocial care, serious illness conversations, and an individualized management plan appropriate for optimizing patients' quality of life (QoL) and reducing caregivers' burden. The importance of developing a comprehensive care approach toward the multiple needs of patients, not just focused at the end of the illness trajectory but also at a broader period concerning “still-active” anticancer therapies, has been pointed out by several authors.7,8
In addition, the financial constraints conditioning the national health systems require an accurate evaluation of the economic advantage of the home care compared with the established hospital setting. In particular, since the treatment of hematologic diseases (including use of life-prolonging anticancer therapies, transfusion requirements, antibiotic therapies, etc.) requires specialized home care services, specific cost drivers contributing to final home care costs should be considered.5,6
At our institution, a specific program of domiciliary provision of supportive and early palliative care has been developed and is carried out by a hospital-based multiprofessional team.9–11
We aimed to compare this home care program with standard care in the hospital with regard to costs of care, use of resources, and clinical outcomes.
Patients and Methods
Study design and population
This was a nonrandomized comparative study conducted at two Italian centers enrolling patients receiving either early palliative simultaneous care at home or standard care in the hospital.
Inclusion criteria were as follows: adult (>18 years) patients with a diagnosis of leukemia, lymphoma, multiple myeloma, or other hematologic malignancies, Karnofsky performance status score of no more than 60, need for skilled nursing, and written informed consent. Also, all patients had to be in clinically stabilized conditions, characterized by the absence of any of the following features: (1) fever persistence >38°C during previous 96 hours or with new onset fever after a period without it; (2) arterial systolic blood pressure <90 mmHg; (3) arterial oxygen saturation <90% or mean arterial pressure <60 torr; (4) major active hemorrhage (>1 World Health Organization scale); (5) altered mental status; (6) hydroelectrolytic imbalance, hypercalcemia; (7) uncontrolled dyspnea, or diarrhea or pain. Exclusion criteria were as follows: being fully self-sufficient according to activities of daily living (ADLs) scores and previous participation in the home care program. The ethics committees of participating centers approved the study protocol, and all patients provided informed consent.
Home care versus hospital care group assignments
Allocation to either of the two care groups was based on pragmatic considerations, including (1) the caregiver availability, (2) distance/travel time to the hospital <60 minutes, (3) psychosocial situation and home environment suitable for home care program.
Criteria for entering patients in the home care program were carefully assessed during an initial interview with the patient and the designated caregiver. The availability of an adult caregiver at home was the main inclusion criterion to allow patients entering the home care program. Patients who did not meet these criteria were assigned to the standard hospital care group.
The home care program included a multidisciplinary team of physicians, nurses, psychologists, and social workers who were trained in hematology, supportive care, and palliative care; details about the home care program, including packed erythrocyte units (PEUs), packed platelet units (PPUs) transfusion, and its structure, have been described elsewhere. 5 To guarantee continuity of care, a doctor and a nurse of the home care team was available 24 hours a day. Patients participated in the home care program until death, or return to the ambulatory or hospital setting.
For descriptive purposes, and regardless of the setting of care, all patients were categorized as being in (1) active-advanced phase, treated with life-prolonging intent chemotherapy regimens but in need of early palliative care for symptom control and the management of anticancer treatment-related complications; (2) terminal phase, if judged by the physician with a life expectancy of less than three months, in need of end-of-life care.
Clinical outcome assessment
Clinical endpoints were the rate of new infections, the rate of new hemorrhages, and the mean weekly number of PEU/PPU transfusions across the study interval. Patient-reported symptom burden was evaluated at prespecified time points, including at baseline (i.e., study entry) and at one, two, and four weeks, with the validated M.D. Anderson Symptom Inventory (MDASI). 12
Health economic analysis
During hospitalization, any patient-related cost (human resources, drugs, transfusions, tests, hoteling) is covered by the local health authority through the standard disease-related group reimbursement system.
The home care program for patients with hematologic diseases is funded by a charity organization, the Associazione Italiana contro le leucemie linfomi e mieloma, Sezione di Roma (ROMAIL “Vanessa Verdecchia” Onlus) and by the public trust. For home care, a mixed system of financing is implemented: the public hospital or the local public health care credit bears the costs of health professionals, the transfused units, the diagnostic tests, and the refundable drugs. In addition, the charity organization “AIL” supports the home care program by paying a part of the costs of additional health professionals and their transport. Finally, the patient's family uses its own financial resources for bearing direct and indirect disease-related costs, not being provided by any economic public voucher.
With the aim of determining the economic burden according to one of the two settings of care, the costs have been calculated either from the point of view of local health authority and “AIL” charity or from the client's point of view, including the direct costs incurred by the family.
From the health provider perspective, a patient's mean weekly cost (MWC) of care at the hospital or at home was built by direct medical cost drivers: fees of drugs, diagnostic tests, blood transfusions, cost of health care professionals (doctors, nurses and other providers), and other overall costs of the services required by these patients. The costs of hospital staff have been calculated on the basis of professional salaries (for categories, not individual), divided on the basis of professional time (hours, minutes, days, weeks) dedicated to the patient, detected for each activity requested, according to an activity-based costing analysis. The same method was used in the evaluation of the cost of back office activities, then reported as the average value to the entire population. Costs of “hoteling” ward maintenance care (food, laundry, etc.), assessed in hospital care, were obtained from the hospital administration.
MWC for the patient's family was related to the following variables—formal caregivers, food costs/cleansing agents, transportation costs, parking, and costs of family visits. The latter three variables were accounted for costs sustained by relatives visiting the hospitalized patients. Indirect cost items, such as social costs and the impact of the sickness on the patients' or a family member's capacity to work, were not considered.
From an economic standpoint, home care and hospital care were evaluated through two different health economic analyses: cost-minimization analysis (CMA) and cost-effectiveness analysis (CEA). CMA evaluates which setting of care could be considered cost-saving by subtracting costs related to hospital care to home care ones, while CEA relates the resource consumption (i.e., the days of care costs) to an efficacy endpoint resulting in a significant difference between the two groups of care (i.e., hemorrhages or new infections avoided) through the following formula:
Incremental cost-effectiveness ratio (ICER) = (home care costs − hospital care costs)/(% of avoided infections at home − % of avoided infections at hospital). 13
The efficacy endpoint was obtained for each setting by calculating the percentage of avoided new infections with the following formula: % of avoided infections = 1 − incidence (rate) of infections treated with intravenous antibiotic therapy. Since infections are one of the main issues in hospital care setting, they were considered the main output that could magnify differences between the two care settings. Finally, because of the considerable number of deaths or reversion to ambulatory care occurred before the end of the eight-week time study interval, the cost analysis of the model of care has been performed in respect to a global time horizon of three weeks: in this way, it was possible to establish a three-week trend of expenditure, which esteemed the evolution of costs in the individual subpopulations.
Statistical analysis
Group comparisons of baseline characteristics were done with Fisher’ exact test for binary variables, with chi-square tests for other categorical variables, and with the Wilcoxon rank tests for metric, non-normally distributed variables (incl. treatment costs). Survival plots were created for descriptive purposes only. Patient-reported outcomes were analyzed with a repeated-measures analysis of variance including a group-by-time interaction term to compare change over time between the two study arms. The level of statistical significance was alpha = 0.05. All analyses were done using SAS Proc Mixed software, version 9.4 (SAS Institute, Cary, NC).
Results
Sample characteristics
Between February 2016 and March 2017, 120 patients were recruited for the study, of which 119 were included in the analysis (one patient in the home care group moved to another city during the study period). Mean patient age of patients was 66.1 years and 52.1% were men (Table 1).
Sociodemographic and Clinical Patient Characteristics at Study Entry
P-value given for pairwise comparison of patients in home care and hospital care.
ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; ANC, absolute neutrophil count; Hb, hemoglobin; MDASI, M.D. Anderson Symptom Inventory; MDS, myelodysplastic syndrome; PLTS, platelets; WBC, white blood cell.
Compared with patients in home care, patients in the hospital were younger (p < 0.001), had a higher ADL score (p < 0.001), higher Karnofsky performance status (p = 0.001), higher Hb levels (p = 0.001), and a lower MDASI symptom interference score (p = 0.033) at baseline. Also, patients at home had a significantly worse median overall survival (2.75 months) as compared with those in hospital (8.39 months; p = 0.001; Fig. 1).
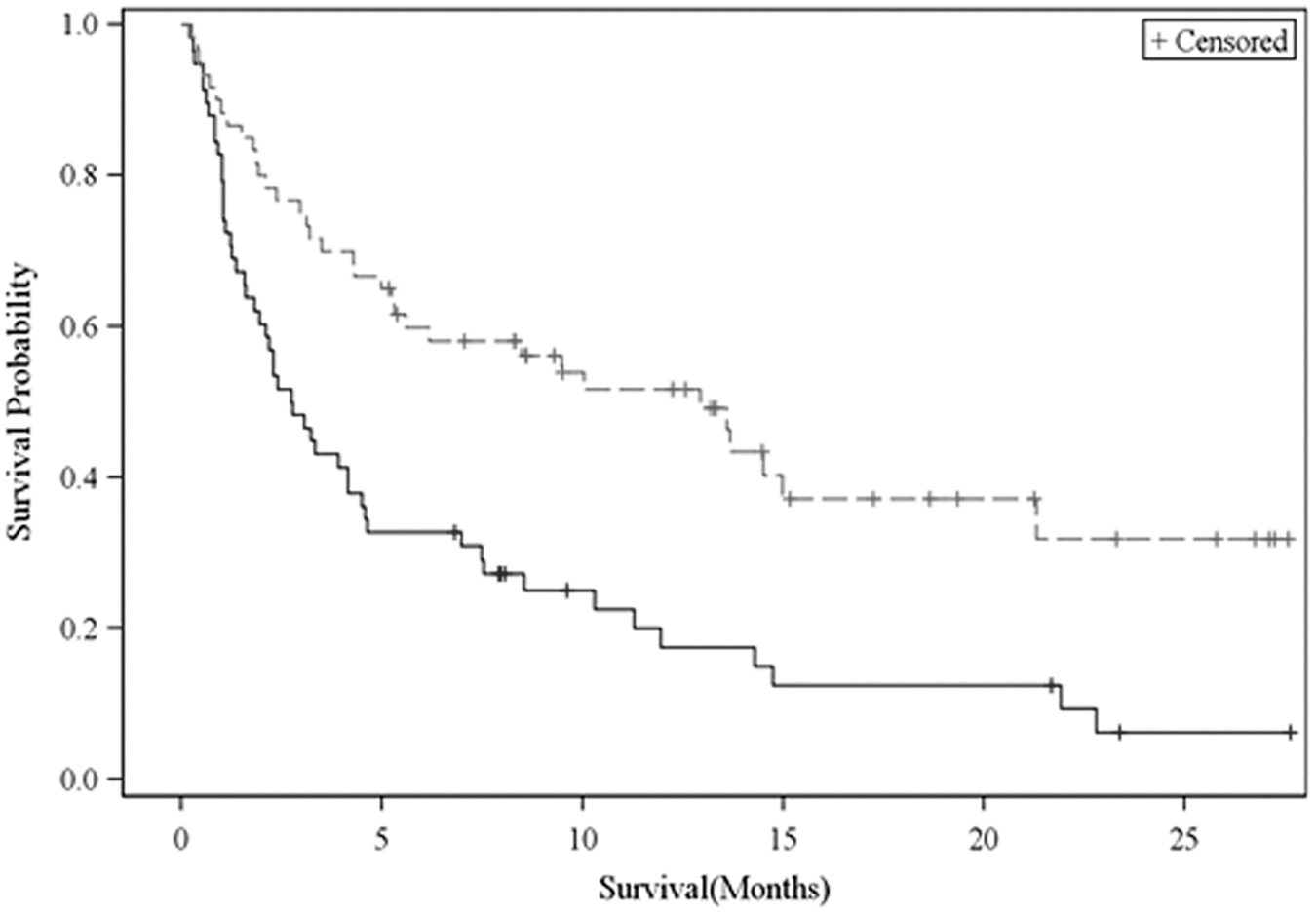
Overall survival curve for patients receiving care at home and in the hospital. Patients receiving care at home (solid line) and patients receiving care in the hospital (dashed line).
The median duration (i.e., length of stay) of patients in the study program was 16 days in the hospital group (range: 7–37) and 31 days in the home care group (range: 5–56 days). Moreover, 39 patients in home care (66%) were still on the study on week 4, as compared with 10 of those hospitalized (17%).
The main reasons for study discontinuation were death (home care: 29 patients, hospital: 3 patients; hospitalization: 4 in home care group; ward discharge: 53 patients in hospital group, only).
Clinical outcomes
As shown in Table 2, patients at home and at the hospital did not differ statistically significantly with regard to the mean weekly number of PEU/PPU transfusions received, although the mean weekly number delivered at home (1.45) was lower than that at hospital (2.77; p > 0.05); or with regard to the number of new hemorrhages (home care 8.5% vs. hospital care 11.7%, p = 0.563). Among those patients who had no fever at study enrollment, the infections requiring a new parenteral antimicrobial therapy occurred more frequently at hospital (53.8%) than at home (21.2%; p < 0.001). At home, of 11 new infections requiring intravenous therapy, 2 proved to be fevers of unexplained origin (FUO), 3 catheter-related bloodstream infections (1 Coagulase Negative Staphylococcus, 1 Escherichia coli, 1 Enterococcus faecium), 3 lower respiratory tract infections, 2 cutaneous cellulitis, and 1 Aspergillus fumigatus sinusitis. At hospital, 29 new infections occurred: 7 were FUO, 13 pneumonia, 3 catheter-related bloodstream infections, 2 proctitis, 4 Citomegalovirus infections; a pathogen agent was identified in 19 of them (bacteriemias were constituted of Klebsiella pneumoniae in 4 cases 5 E. coli extended spectrum beta-lactamases (ESBL)+ in 5, E. faecium in 5, Coagulase Negative Staphylococcus in 5).
Clinical Outcomes
P-value given for pairwise comparison of patients in home care and hospital care.
Erythrocytes transfusions and/or platelet units.
In patients with no fever at enrollment.
No statistically significant differences between the two groups of care were found for mean change over time for MDASI symptom severity (p = 0.139) and MDASI symptom interference (p = 0.284) (Table 2).
Resource use and cost analysis
The mean weekly time (in minutes) per patient dedicated by physician and nurse, comprehensive of front office and back office activity, was, respectively, 340′ and 600′ at hospital and 270′ and 235′ at home (p < 0.05).
The combination of the four cost drivers (health care professionals, materials and drugs, transfusion support, laboratory) and their relative weight in the cost-building of the mean weekly cost differed according to the site of care and phase of disease. As shown in Figure 2, regardless of the phase of disease, out of the whole cost of care, the costs related to health care professionals at home (by ∼60%) were significantly higher compared with hospital care (by ∼20%; p < 0.05); whereas at hospital the costs for drugs were higher (by ∼45%) compared with home (∼20%; p < 0.05), as well as costs for transfusions, especially for patients in advanced phase (30% vs. 17%). There is a ∼1:3 ratio between spending on home care and spending on hospital care. Indeed, the average of the first three weeks MWC of care at home (€ 1219.7) was significantly lower than that for care at hospital (€ 3534.3; p < 0.05). The 1:3 ratio between home care and hospital spending was confirmed both in active-advanced phase (€ 1253.3 vs. € 3493.0) and in terminal phase of disease (€ 1170.6 vs. € 3638.9), respectively (Table 3).
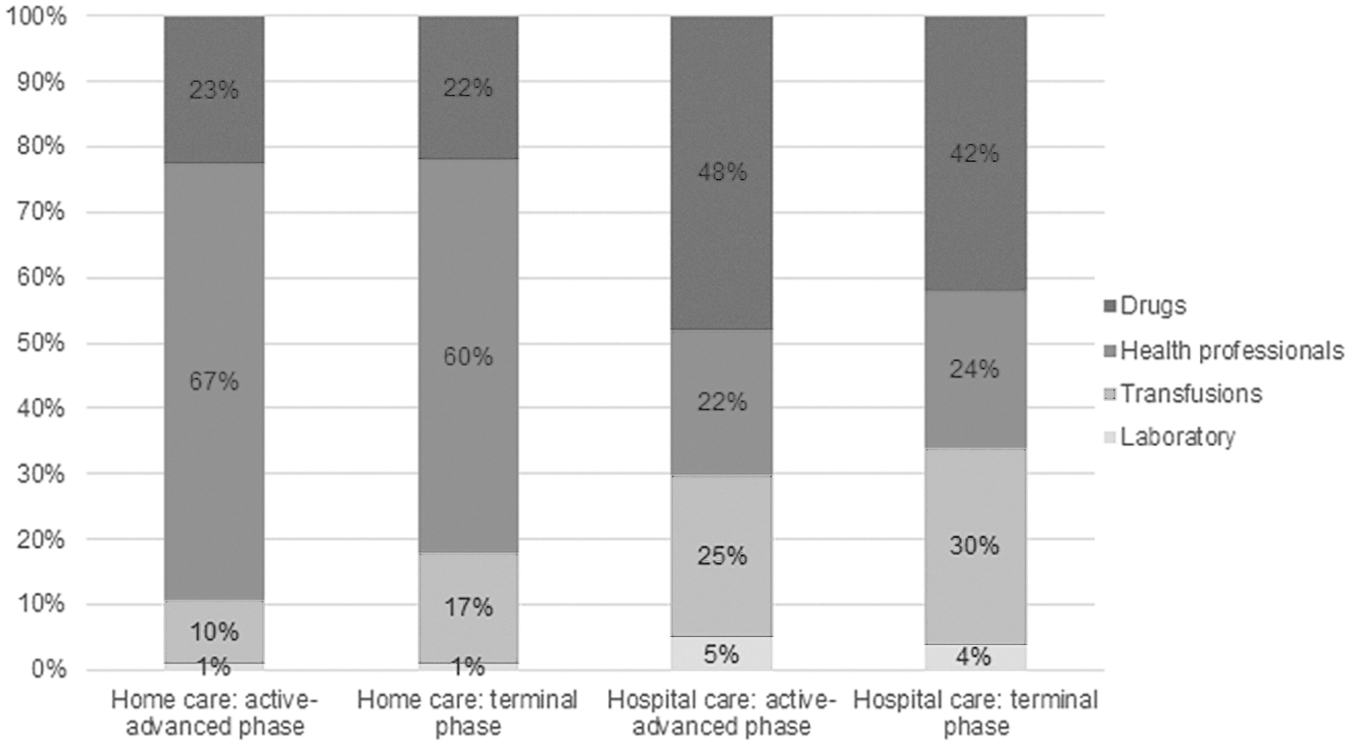
Cost drivers of mean weekly cost according to setting of care and phase of disease.
Cost Analysis According to Site of Care and to Disease Phase
CMA = hospital care mean cost − home care mean cost.
ICER = (home care costs − hospital care costs) / (% of avoided infections at home − % of avoided infections at hospital).
CMA cost-minimization analysis; ICER, incremental cost-effectiveness ratio; Ph., phase of disease.
Regarding the out-of-pocket expenses for the families, the MWC for caring home patients was higher (€ 162.6) than that sustained from the families with hospitalized patients (€ 76.7) (p < 0.05), especially for patients in terminal phase being € 182.0 and € 56.0, respectively.
On a three-week CMA, the home care produced for the health care provider a mean weekly cost saving of € 2314.0 versus the hospital care, independently from the phase of disease; whereas at home the patients' families suffered an extraweekly charge of € 85.9, even higher for patients in terminal phase (€ 126.1).
The CEA performed to link costs and outcomes showed a negative value for the ICER, of −7013.9, indicating a worse cost-efficacy ratio for the hospital setting, as compared with the home one, in terms of days of care for avoided infections. Even when detailed for both advanced and terminal phase groups of patients, CEA showed as a negative value (respectively, −5208.6 and −12,341.5) as seen overall.
Discussion
Our findings suggest that home care produced for the health care provider a mean weekly cost saving of €2314.0 versus the hospital care, independently from the phase of disease. Considering the real-life setting of our study, treatment allocation in the two groups was based on eligibility of individual patients for the home care program in terms of caregiver availability, travel time to the hospital, psychosocial situation, and home environment. Hence, this selection process obviously resulted in various differences between patient groups. The most notable difference was the median survival, which was higher in patients treated in the hospital compared with those treated at home. Also, there was a different proportion of patients in terminal phase between study groups, being 41% and 28% for patients treated at home and in the hospital, respectively.
While all these aspects should be considered when interpreting our findings, we also observe that the advantage in terms of cost saving for early palliative home care was found both for patients in active-advanced phase (€ −2239.7) and for those in terminal phase (€ −2468.3).
Although the overall average cost at home was one-third lower than at hospital, in this study the activity-based analysis showed a higher impact of the costs for professionals at domicile, probably explained by scale economy reasons. At a hospital ward, the ratio between a single professional and the number of patients assisted is in fact lower than that estimated at home.
With regard to clinical outcomes, the number of new hemorrhages was similar in both groups of care, whereas, although not statistically different, the weekly mean number of PEU/PPU transfused at home was lower than that at hospital. New infections requiring a treatment were substantially more frequent in the hospital group compared with the home care group. Accordingly, CEA showed an overall advantage for home care, with an ICER € −7013.9 of prevented days of care for infection, as well as for the two prognostic groups of patients.
Patient-reported symptom burden did not show a significant difference between home and hospital care with regard to change over time, suggesting that symptom control at home care was not worse than the one that could be achieved in the hospital. This is an important finding also considering that patients in the home care group consisted of more fragile, older patients with a worse prognosis than those cared in the hospital.
The results of this real-life prospective study in the hematologic setting are broadly in line with those reported in some retrospective studies focused on the general oncologic population. 14 Jones et al. reported a cost analysis comparing hospital admission and home care, showing that hospital at home was significantly cheaper and the cost difference was sustained even when analyzed at three months. 2 A French analysis suggested that the average costs for home care were significantly lower than that reported for hospitalization considering palliative care group, whereas no differences were identified for active treatment group. 3 Gomes et al. 15 performed a Cochrane analysis to estimate effectiveness and CEA of home palliative care services. They identified 23 studies, and the meta-analysis identified increased odds of dying at home, reducing symptom burden for patients, no effect on caregiver grief, but no conclusive data about cost-effectiveness.
Patients with hematologic malignancies in advanced and terminal phases of disease, especially with diagnoses of acute leukemia, have difficulty in accessing palliative care programs,16,17 and are more likely to spend the last period of their lives within hematology wards, emergency room, intensive therapies, or accessing with high-frequency day hospital units.18,19 This type of assistance implicates a loss in terms of QoL for patients, and also can translate into an increased health expenditure and a disadvantageous resource allocation. 20 The efficacy and need of a simultaneous model of care for cancer patients have been emphasized since many years, capable of integrating active treatment with palliative approaches, to intercept and address specific needs other than just the “chemocure,” all over any phase of the disease trajectory, even at the beginning of the treatment pathway. 21
Our study has several limitations. These include the relatively small sample size and the nonrandomized study design, which accounted for a number of differences between study groups, including, for example, with regard to the phase of the disease. Also, we observe the lack of details about colonization and primary antimicrobial prophylaxis undertaken. Finally, the study was carried out in two centers where an institutional home care program, with dedicated trained personnel, was available. Therefore, findings cannot be generalized to those hospitals for which such logistic is not available.
Conclusion
In conclusion, our results suggest that costs of home care are lower than standard hospital care costs regardless of the phase of disease and further larger, and controlled studies are needed to confirm the benefits of this working model. Domiciliary assistance may also be cost-effective by reducing the number of days to treat infections.
Footnotes
Funding Information
This study was supported by the Associazione Italiana contro le leucemie linfomi e mieloma, Sezione di Roma (ROMAIL “Vanessa Verdecchia” Onlus).
Author Disclosure Statement
No competing financial interests exist.