
Abstract
Background:
An often-stated concern is that dying persons receive too much aggressive medical care.
Objective:
Examine next-of-kin perceptions of the amount of medical care received in the last month of life.
Design:
Mixed-methods study with 623 survey responses and in-depth interviews with a subsample of 17 respondents.
Subjects:
Nontraumatic deaths 18 years and older in San Francisco Bay area.
Measure:
The survey asked: “During the last month of your family member's life, did he or she receive too little, the right amount, or too much medical care?” Additionally, surveys examined 18 measures of quality of care in the last month of life, reporting concerns or unmet needs with staff communication, symptom management, emotional support, physician communication, treating the patient with dignity, respecting a person's culture, spiritual support, and providing timely help after hours.
Results:
Of the 623 survey respondents, 16.9% reported their loved one received “too little” care while only 1.4% reported “too much.” Likelihood of reporting too little medical care did not differ by age, gender, or being insured by Medicaid only. Respondents who reported “too little” compared with those that stated the “right amount” reported higher unmet needs for symptom palliation, physician communication concerns, with other important opportunities to improve the quality of care. Among the 17 in-depth interviews of those indicating “too little” care on the structured survey, the predominant concern (n = 10) was inadequate symptom management.
Conclusion:
While the majority of respondents indicated their loved one received the right amount of medical care at the end of life, a notable minority (one in six) indicated that their loved one received too little care.
Introduction
The lay press often states in fear provoking headlines that Americans are receiving “too much” aggressive care at the end of life with headlines, such as “The U.S. still gives too many patients too much end-of-life care.” 1 A debate has occurred over the “high costs of dying” 2 with some noting that dying is often marred by costly intensive care unit (ICU) and hospital care that represents “waste in the present system.” 3 These judgments that persons receive “too much” care are based on retrospective studies of decedents of health care utilization.4,5 The use of retrospective cohort studies of health care utilization has been debated.6,7 Evidence from both randomized clinical trials and observational studies suggests that palliative care can reduce health care costs. 8 Yet, no study to date has asked next of kin, usually a close family member or close friend, whether they believed that their loved one received “too much” versus “too little” care in the last months of life.
Three national demonstration programs9–11 that are either in progress or soon beginning are aimed at testing new payment models and benefits to improve the quality of care and reduce health care costs at the end of life. Key to each of these models is enhanced shared decision making and advance care planning, which can result in dying persons and their family receiving palliative care at an earlier time point. This may help in avoiding expensive terminal hospitalizations and ICU care in the last month of life. Under traditional Medicare or “fee-for-service,” financial incentives may result in persons receiving hospitalizations, ICU stays, and invasive mechanical ventilation that may be contrary to patients' informed preferences and their likely outcomes of care.
Payment policy that focuses on value-based incentives may result in improved person- and family-centered medical care at the close of life that either is cost neutral or saves money. A fundamental premise of these payment policy changes is that persons receive “too much” aggressive care in the last month of life. In this study, a mortality follow-back survey was conducted in a market with high Medicare Advantage (MA) penetration to examine bereaved family members' or friends' perceptions of the amount and quality of medical care that their family member or friend received in the last months of life
Materials and Methods
Design
A mortality follow-back survey was conducted in the nine counties surrounding San Francisco as part of an effort to document opportunities to improve care at the close of life. Our goal was to sample deaths of chronic progressive illnesses; therefore, persons who died from accidents, suicide, or murder, whose manner of death was undetermined, and those who were pregnant at the time of death, or under the age of 18 were excluded.
Surveys were mailed to the next of kin or informant listed on the death certificate. If an informant did not respond after a second mailing, initially, attempts were made to contact the person listed as the informant through phone. However, as most informants did not have listed phone numbers, telephone follow-up was suspended and a second survey was mailed to all nonresponders. The survey was available in English, Spanish, and Chinese (a translation understandable to both Mandarin and Cantonese speakers). For decedents of Chinese or Hispanic ethnicity, and whose informant lived in zip codes with high rates of Spanish- or Chinese-speaking individuals, surveys were mailed in English and Spanish or Chinese, respectively.
Twenty respondents were excluded from the analysis because they stated that they were “not at all” familiar with the decedent's condition in the last month of life. Surveys were conducted about 9 months after the patient's death (ranging from 139 to 459 days with a median of 291 days after the death of the family member or close friend).
The final item in the survey asked if respondents would be willing to participate in an additional in-depth interview by phone. Among persons who indicated they would be willing to participate in this interview, respondents were sampled by place of death (home, nursing home, and hospital) and by those who stated that medical care was not consistent with the dying person's wishes for care. Of those surveyed, 43.5% indicated that they would be willing to be interviewed. Among those respondents who indicated they were willing to be contacted, 92 cases were sampled. Four cases were eliminated because their survey responses indicated that they were not involved in the decedent's medical care.
At the time of completing the fielding of in-depth interviews, 8 persons refused participation in the in-depth interviews when we approached them to schedule an interview (despite stating on the survey they were willing to participate), 3 were unable to be located, and 28 cases were still in process. A total of 49 in-depth interviews were completed to learn more about the end-of-life experiences of the decedent and the decedent's family. Of the completed interviews, 17 interviewees had indicated on the survey that their family member or close friend received “too little” care. The research project was approved by both the RAND Institutional Review Board (IRB) and the State of California IRB.
The overall survey response rate among eligible respondents was 21%. Response rates were lowest among next of kin of decedents who died in hospitals, and highest for the informants of decedents who died in a nursing home or long-term care facility (18.2% vs. 26.1%, p < 0.05). The response rate for those dying at home was 22.2%; the response rate for those dying in other locations was 23.0%. Informants of white decedents were more likely to respond than informants of black and Asian decedents (25.3% vs. 15.4% and 16.9%, respectively; p ≤ 0.05). Response rates were lower among those for whom the death certificate noted were of Hispanic heritage as compared with white non-Hispanic decedents (15.1% vs. 27.5%, p ≤ 0.05). Response rates were higher when the decedent was older (90+ response rate of 28.4% compared with 13.4% for those younger than 65, p ≤ 0.05). There was no difference in response rate by gender of the decedent.
Main outcome measure and survey content
The focus of this analysis was on a survey item that asked: “During the last month of your family member's life, did he or she receive too little, the right amount, or too much medical care?” The survey was divided into items that focused on the last month of life overall, and the quality of care during a stay in a hospital, nursing home, assisted living facility, or while receiving hospice services or home health, in which the decedent received two or more days of care. In this analysis, we focused on survey items from prevalent places of care (i.e., hospital and nursing home) and use of hospice services. Survey items were based on Teno et al.'s conceptualization of high-quality person- and family-centered care, 12 as well as items from the Consumer Assessment of Health Providers and Systems (CAHPS) Hospice Survey. 13
Survey items were aligned with the palliative care domains of the National Consensus Project Guidelines for Quality Palliative Care. In this article, we focused on quality care domains of staff communication and symptom management. A first domain focused on physician communication regarding prognosis and whether there was a problem understanding a physician's explanation of treatment, while three items in a second domain focused on whether the decedent received their desired level of physical comfort and emotional support. For persons who experienced pain, dyspnea, or emotional distress, an unmet need was defined as the respondent reporting that the decedent did not receive as much help as needed with that symptom.
A third domain focused on staff communication and whether the staff listened carefully and how often the staff kept the respondent informed about the patient's condition. Survey items in the last month focused on respecting cultural and religious/spiritual traditions, getting needed help on the weekend and after hours, being educated on what to expect while the patient was dying, treating the patient with dignity and respect, and emotional support before and after the death of their family member or close friend. For each of these items, we followed the top-box scoring convention of the CAHPS Hospice Survey. In addition to these quality measures, the survey collected sociodemographic information about the decedent and respondent. Cause of death and site of death were abstracted from the death certificates.
In-depth interviews
For 49 persons, an in-depth interview was conducted to gather next-of-kin perceptions around the decedent's last month of life with questions, including: (1) What went well in the last months of life? and (2) What could have been improved? Probes focused on communication and decision making with health care providers, emotional support, health care transitions, and palliation of symptoms, such as pain, shortness of breath, and anxiety, in the last months of life. In this study, we examined the narratives of 17 respondents who reported on the survey that the decedent received “too little” care.
Analyses
Analyses of survey response data were performed with Stata 15.0 using weights to account for the complex sampling design. Chi-square tests were used to examine the associations of sociodemographic characteristics of the decedent and respondent's report of receiving “too little” medical care in the last months of life. A multivariate model predicting the response of “too little” medical care examined the association with age, gender, race, education of the respondent, cause of death, place of death, and functional status measured by mobility in the last month of life.
Two analyses were undertaken to understand the respondents' concerns when they said “too little” medical care. First, we examined the univariate association of the five key quality measures of the survey with the survey response of receiving “too little” medical care compared with persons who stated the decedent received the right amount of medical care. Second, a qualitative content analysis was conducted on the 17 narratives to identify the main concern of narratives where the respondents stated they received “too little” medical care. Two reviewers (J.M.T., J.N.B.) reviewed transcripts of each narrative for the main concerns based on responses to the interview on what could have been improved in the last month of life.
Results
Out of 623 respondents, 100 (weighted percentage 16.9%) believed the decedent received “too little” care, with 81.7% stating their loved one received the “right amount” of medical care. Only 13 respondents stated they received “too much” medical care (1.4%). Table 1 describes the overall sample and respondents who reported “too little” or “right amount.” A multivariate model examined whether there were sociodemographic differences by race, gender, relationship of the respondent to decedent, causes of death, site of death, insurance, and functional trajectory measured by mobility loss in the last year of life. While there were some differences by cause of death and education of the respondent, there were no differences by age, gender, site of death, insurance type, or by functional trajectory in the last year of life with the perception of receiving too little care in the last month of life (Table 1).
Characteristics of “Too Little” versus “Right Amount of Care”
Significantly different at the univariate level.
The “other” cause of death category included diseases like chronic kidney or liver disease, primary hypertension, type 2 diabetes, hyperlipidemia, and other diseases that were too low in frequency to report based on the data use agreement to use death certificate data.
CHF, congestive heart failure; CI, confidence interval; NH, nursing home.
Two exploratory analyses were conducted to better understand the response of “too little” medical care. First, we examined the association of quality measures with the response “too little” and “right amount.” Table 2 presents the rate of unmet needs and concerns with the quality of care for those who indicated that the decedent received “too little” care and those who indicated that the decedent received the “right amount” of care. While the rate of unmet needs for symptom palliation was high even among respondents who stated their family member or close friend received the right amount of care, the proportion of unmet needs was substantially higher among those respondents who reported “too little” medical care. Even among those receiving hospice services, 80.0% of those reporting “too little” care reported unmet needs for pain management compared with 18.8% among those respondents who reported the “right amount” of care.
Staff Communication and Unmet Needs for Symptom Management
p ≤ 0.05 for the comparison of response “too little” medical care vs. “right amount” medical care by setting of care.
For decedents that were hospitalized, the proportion of concerns with physician communication about prognosis and medical treatment was nearly double that reported by respondents who stated they had the “right amount” of care (Fig. 1). Table 3 examines concerns in the last month of life, contrasting those that stated “too little” versus “right amount” of medical care. Respondents noted concerns with religious/spiritual beliefs not always being respected (53.4% vs. 19.1%, p ≤ 0.05) and cultural transitions not always being respected (57.6% vs. 19.1%, p ≤ 0.05). In addition to these two areas of concern, there was a similar pattern of reported concerns being significantly higher in respondents who stated they received “too little” care, which indicates important opportunities to improve medical care in the last month of life.
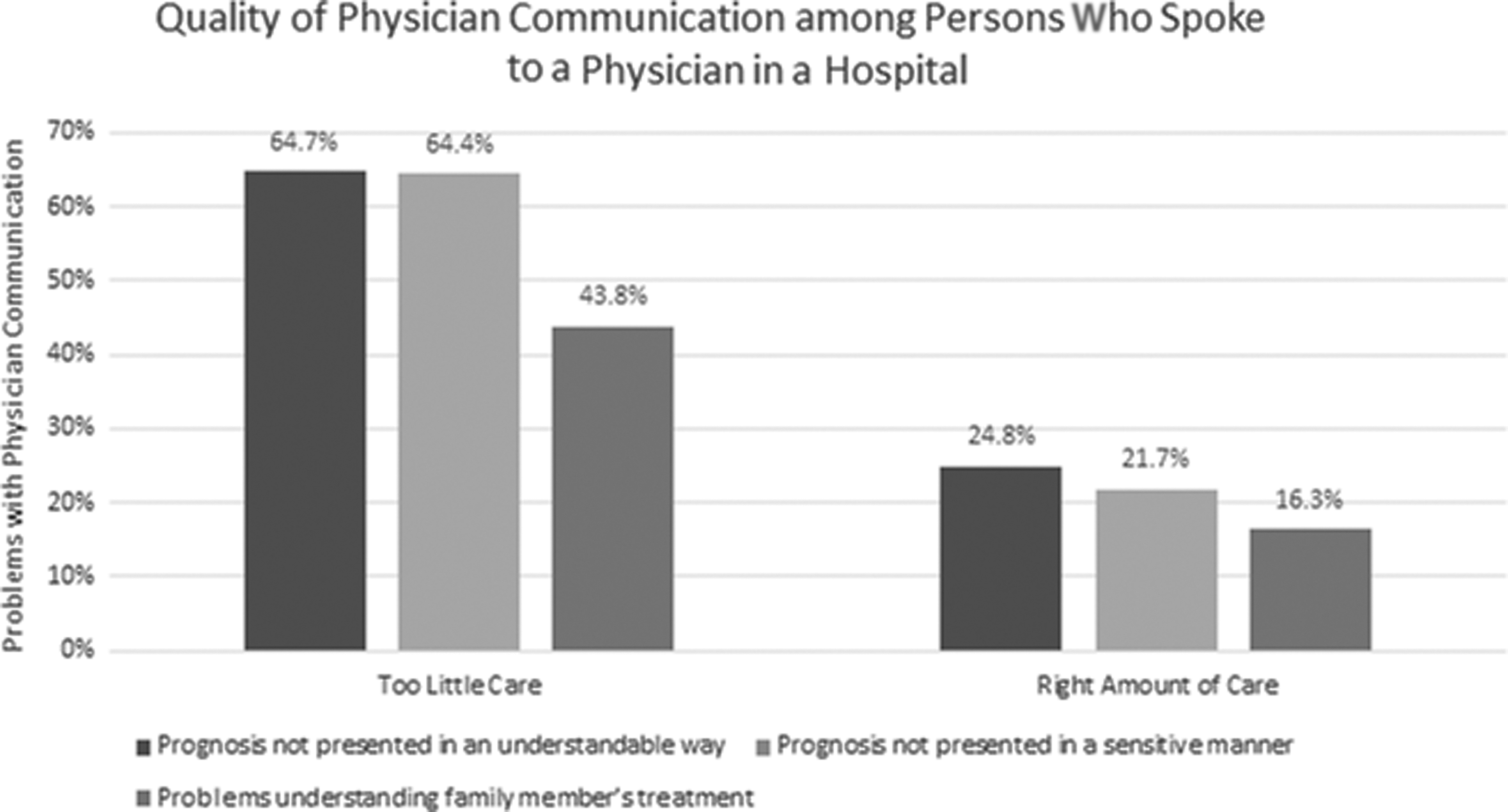
Reports the concerns for communication about prognosis and medical treatment among the 87.1% of hospitalized decedents whose family member or close friend reported “too little” medical care and spoke with a physician compared with 93.5% of respondents who reported the “right amount” of medical care. All differences significant at p ≤ 0.05.
Quality of Care in the Last Month among Respondents That Stated “Too Little” or “Right Amount” of Medical Care
p ≤ 0.05.
Out of 49 in-depth interviews, a second exploratory analysis examined 17 narratives of persons who stated in the structured interview that their loved one received “too little” care. These results are presented in Table 4. In 10 of these 17 cases of “too little” care, the main concern was symptom palliation. For example, interviewees described concerns with timely delivery of opiates from the pharmacy and difficulty getting an opiate prescription filled for chronic pain. The following narrative reported the failure of medical technicians at an assisted living facility to administer opiates as prescribed to an 85-year-old dementia patient:
Narratives of Respondents Who Stated Their Family Member Received “Too Little” Care
ALF, assisted living facility; ER, emergency room; ESRD, end stage renal disease; NH, nursing home; POLST, Physician Orders for Life-Sustaining Treatment; UTI, urinary tract infection.
And the worst part is that they [medical technicians] come with their religious beliefs … They controlled it (i.e., morphine) in their pharmacy dispensary so we couldn't ever take control of that. But somebody having to be on duty, if it was in the middle of the night and my mother needed morphine. And they disagreed. They said “you're basically killing your mother, you're taking your mother's life.”
In two cases, the concern was monitoring and administration of medications for the management of congestive heart failure. Both of these cases involved persons residing in an assisted living facility that used medical technicians to administer medications. An 85-year-old male was transferred from an assisted living facility to the hospital because of the failure to administer treatment for his congestive heart failure.
… And she said, no, they had not been giving him the extra lasix. And this is eight days into when they should have been giving him the extra lasix, right. And I was like, are you kidding me?
Bereaved family members' narratives demonstrated unmet needs around pain control in the last month of life (even among decedents who had been on hospice), with several family members noting that their loved ones suffered in pain as a result of not enough attention to or management for their pain as well as other related symptoms, including shortness of breath and anxiety.
Discussion
An assumption often stated in the lay press is that Americans are getting “too much” care at the end of life and that care received does not reflect their preferences for care. Contrary to expectations, nearly one in six respondents stated that their family member or close friend received “too little” medical care. This is not “too little” ICU care or hospitalizations, but rather “too little” in that their family member or close friend did not receive their desired symptom palliation or enough communication. Only 1.4% reported they received “too much” medical care. Among respondents who stated they received “too little” medical care, the overwhelming concern was adequate symptom palliation, even among those who received hospice care.
The focus of this study was on deaths that occurred in the nine counties surrounding San Francisco as part of a baseline audit for a private foundation. Unlike the rest of the United States, the penetration of MA in this area is high. In 2015, 43% of decedents in these nine counties were cared for by a MA plan compared with a national rate of 23%. MA plans have more flexibility to provide high-quality care to seriously ill populations. 14 Even in a region with high MA penetration, opportunities to improve quality of end-of-life care exist. Current U.S. payment policy is transitioning from fee-for-service to paying for value. Innovation is needed, such as current efforts of the Center for Medicare and Medicaid services to carve hospice into MA plans as planned under the demonstration program, “Value-Based Insurance Design demonstration for Medicare Advantage.” 11
Important limitations should be acknowledged. Even with mixed-mode survey administration, the response rate was only 21%. It is possible that a biased set of respondents with greater concerns chose to complete the survey. While this could potentially result in an overestimation of the proportions of persons with unmet needs or concerns, the narratives attest to the suffering of decedents and that the family or close friend's last memories of the death were marred by health care that did not provide high-quality care. Furthermore, this is a retrospective study with the respondent knowing that the person died, which could bias the respondent's memory of events. However, there are important advantages of this retrospective approach, including a clearly defined denominator. Persons listed as the next of kin or informant on the death certificate were interviewed at varying times after the death. However, previous research found moderate-to-high stability of response, even among those with changes in grief. 15 Respondents in some survey items act as a proxy for the patient and, for other items, report on their own experience; the World Health Organization notes that palliative care involves the care for the dying person as well as their family or significant others. Furthermore, a review of the literature found that family respondents accurately report on many quality-of-care domains. Lastly, there are important limitations to this observational study owing to its nonexperimental design that only allows the reporting of associations, not causation.
Conclusion
A 2004 JAMA 16 article found important opportunities to improve the U.S. experience of dying, concluding: “With the baby boom generation starting to reach retirement age, there is urgent need for improving end-of-life care in the United States.” This current study, completed nearly two decades after the 2004 JAMA study of person- and family-centered care at the last place of care, attests to the continued need for multifaceted and sustained interventions to improve the quality of care in the last month of life. New challenges since 2004 include the growth of assisted living facilities, as demonstrated by three narratives where respondents detail their concerns on the quality of care in those facilities (Table 4). Persistent poor quality of care of dying persons who spend time in nursing homes in the last month of life is reported as found in the 2004 study.
Between 2000 and 2020, there has been striking growth of hospital-based palliative care teams and use of hospice services, although too often, these are only used in the last seven days of life. The words of next of kin describing the death of a middle age man from cancer is a resonate call for action:
… [He was} lying on the floor, writhing in pain. There was no connection there, the hospital or the doctor, or whoever. The doctors were not following up with this …
Footnotes
Acknowledgments
The authors thank the interviewers and staff of the RAND Corporation.
Funding Information
Funding for this survey was made by the Stupski Foundation.
Author Disclosure Statement
No competing financial interests exist.