
Abstract
Background:
Palliative care seeks to support the physical, psycho-social and spiritual needs of patients and families who are facing life threatening diseases. Advantages of establishing a palliative care unit, or alternatively co-locating patients, include promoting optimal physical and psychological symptom management; increased family satisfaction; and facilitating resource allocation.
Objective:
To design a stand-alone hospital unit to provide end of life care during a pandemic.
Setting:
Mount Sinai Hospital (MSH), a 1,144 bed tertiary- and quaternary-care teaching facility and Brookdale Department of Geriatrics and Palliative Medicine of the Icahn School of Medicine at Mt Sinai.
Method:
Tracking key indicators signaling the need for conversion to a COVID-19 unit, and identifying factors to facilitate a successful conversion.
Result/Implementation:
Using previously identified key focused action categories as framework, we describe our successful palliative care unit (PCU) conversion into a COVID-19 care unit.
Conclusion:
We believe that these operational insights gained from transforming our unit during COVID-19 will be helpful to other programs and institutions during a pandemic, or public health emergencies.
Introduction
Palliative care seeks to support the physical, psychosocial, and spiritual needs of patients and families who are facing life-threatening diseases. The advantages of establishing a palliative care unit (PCU), or alternatively colocating patients, include promoting optimal physical and psychological symptom management, increased family satisfaction, and facilitating resource allocation by clarifying goals of care and assisting patients and families to select treatments aligned with those goals.1,2
As the coronavirus disease 2019 (COVID-19) epidemic unfolded in NYC, Mount Sinai Health System (MSHS) launched a system-wide initiative of palliative care services to assist clinical teams, and support COVID-19 patients and their families. Mount Sinai's Brookdale Department of Geriatrics and Palliative Medicine quickly developed clinical, ethical, and policy resources for the entire health system. Special emphasis was given to supporting emergency department clinicians and intensivists with guidance on symptom management and advanced care planning. In addition, Mount Sinai Hospital (MSH)'s in-patient PCU was rapidly converted to a special COVID-19 end-of-life unit. In this report we describe the conversion to assist those who may wish to create a special unit or a colocation site to provide end-of-life care during pandemic conditions.
Objective
To design, implement, and operate a stand-alone PCU, or a colocation site, to provide end-of-life care during a pandemic.
Setting
MSH is part of the MSHS, encompassing the Icahn School of Medicine at Mount Sinai, 8 hospital campuses, and 45 ambulatory practices throughout the five boroughs of New York City, as well as Westchester and Long Island.
Methods
MSHS, a major health system at the pandemic epicenter, rapidly developed the clinical infrastructure to care for thousands of COVID-19 patients, including many who required care in intensive care units (ICUs). Many patients were transferred out of ICUs for continued recovery and discharge, but the prognosis for many COVID-19 ICU patients was unfortunately poor. As the health system clinical leadership monitored the surging admissions and the sobering mortality numbers for the region and for the health system itself, Figures 1, 2, consideration was given at the peak of the New York surge to colocate patients who were approaching the end of life.
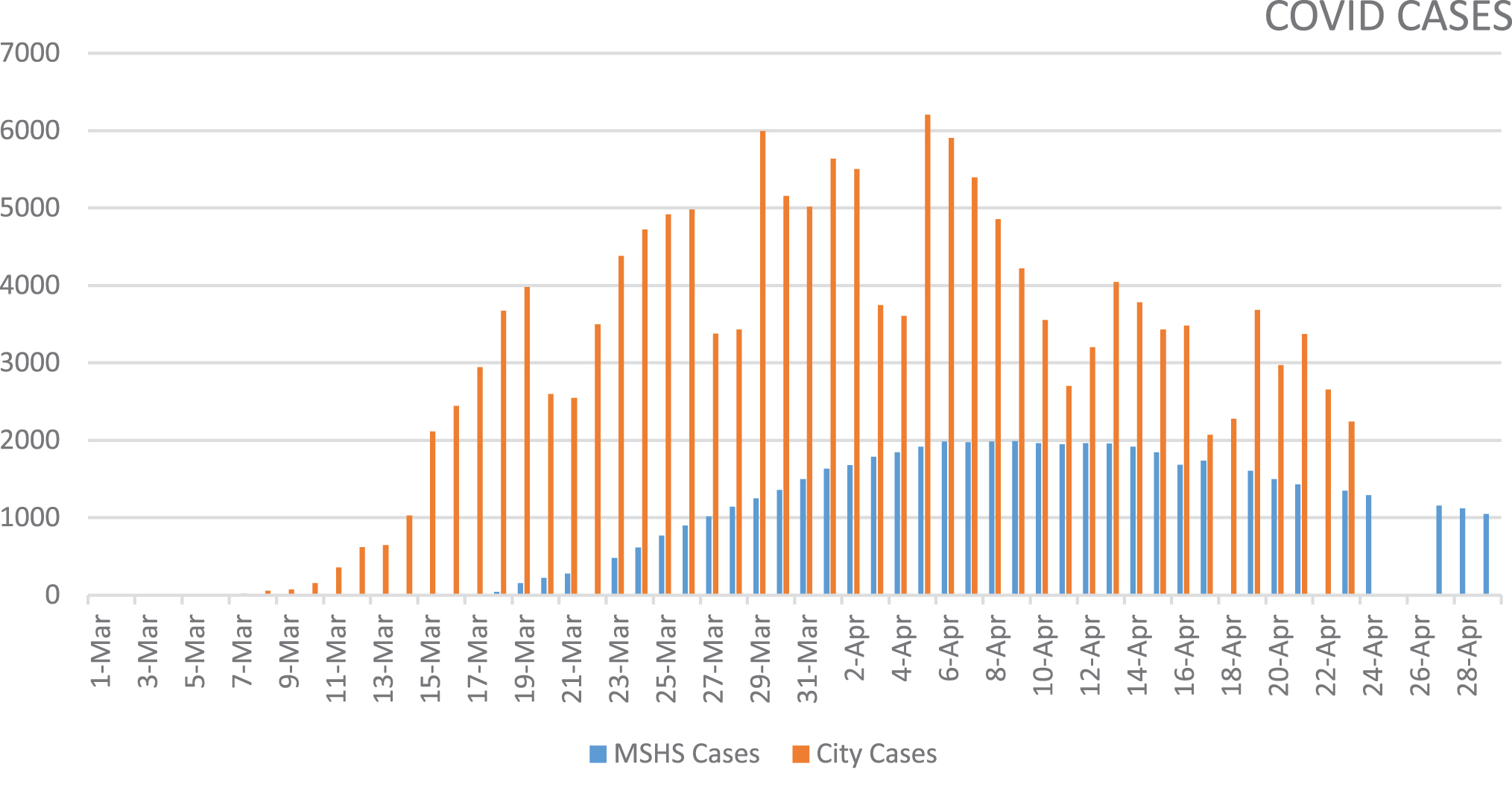
COVID-19 cases. COVID, coronavirus disease.

COVID-19 deaths city, MSHS, MSH. MSH, Mount Sinai Hospital; MSHS, Mount Sinai Health System.
MSH, a 1144 bed tertiary- and quaternary-care teaching facility, was the only MSHS hospital with a pre-existing in-patient PCU. As understanding of the COVID-19 clinical course increased, and patterns of resource allocation emerged, PCU leadership focused on (1) tracking key indicators signaling the need for conversion to a COVID-19 unit and (2) identifying factors to facilitate a successful conversion.
The need for conversion was informed by international data indicating a median length of stay (LOS) for hospitalized COVID-19 patients of 10–13 days.3,4 In NYC, median hospital LOS for these patients was ∼12 days. As the number of hospitalizations increased, PCU conversion would help maintain ICU bed availability. As ICU capacity became limited and expected mortality rate began increasing, the decision was made to convert the unit.
Results
Of the 148 patients screened and accepted for admission during a five week period (April 8, 2020 to May 15, 2020), 135 (109 COVID-19 and 26 non-COVID-19) patients were stable enough to be transferred to the unit. Thirteen patients either died or were unstable for transfer. Two patients were transferred back to a medicine floor after care goals changed. Patient volume averaged 27 per week, approximately double the pre-COVID-19 average volume of 12 patients per week (∼600/year). Fifty-nine (55%) patients were males. Sixty-one (57%) patients were 50–79 years old; 40 (37%) patients were 80–99 years old. Fifty (47%) patients were from an ICU, 48 (45%) from general medicine floors, and 7 (6%) from the emergency department. Of COVID-19 patients, 61 (57%) had a LOS of <48 hours. Forty-eight (44.8%) patients received chaplaincy support. Sixty-two (58%) patients had at least one remote (Zoom) session with family, or an inpatient visit. Twenty-three (21.5%) patients were transferred into the unit on pressors, and 68% were managed on either ventilators (45%), bilevel positive airway pressure (BIPAP) (11%), or oxygen through high flow nasal cannula (12%), Figures 3 and 4.
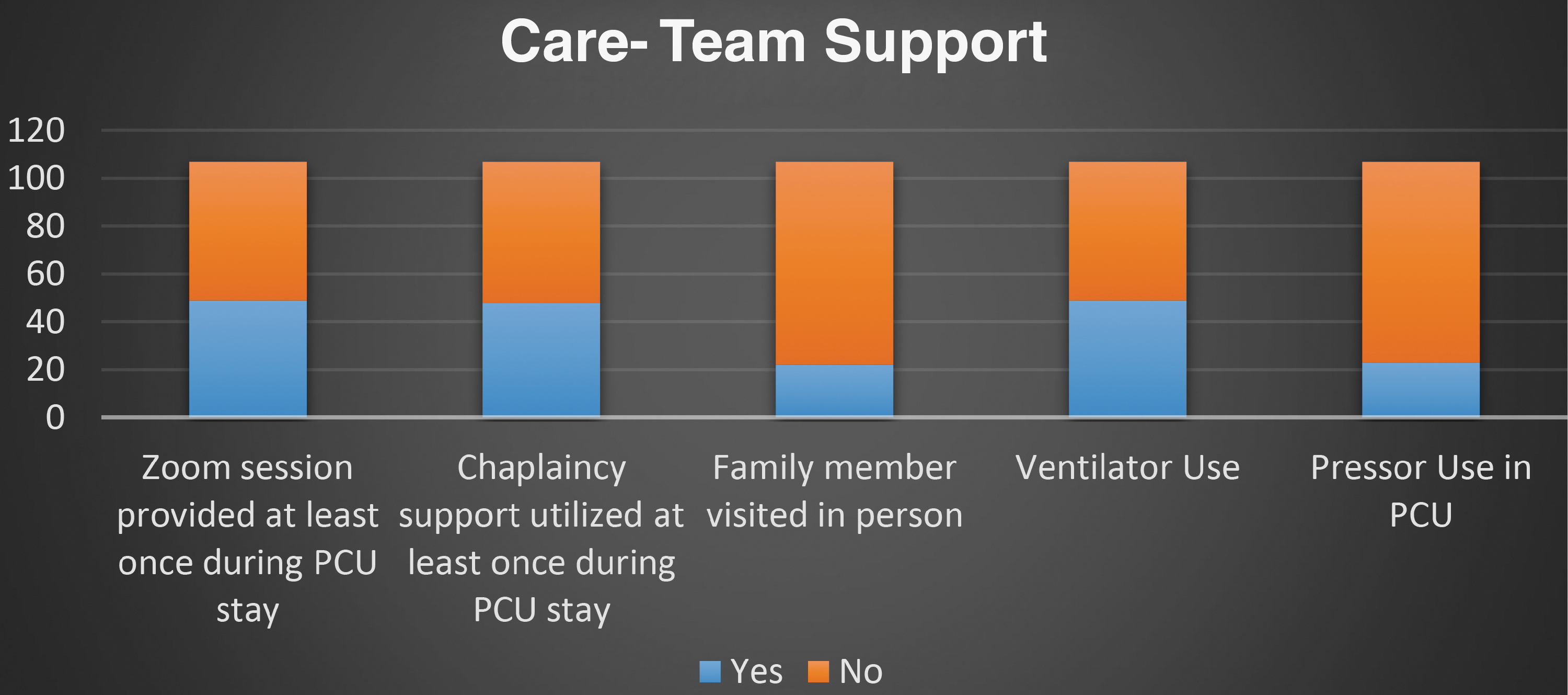
Care team support.
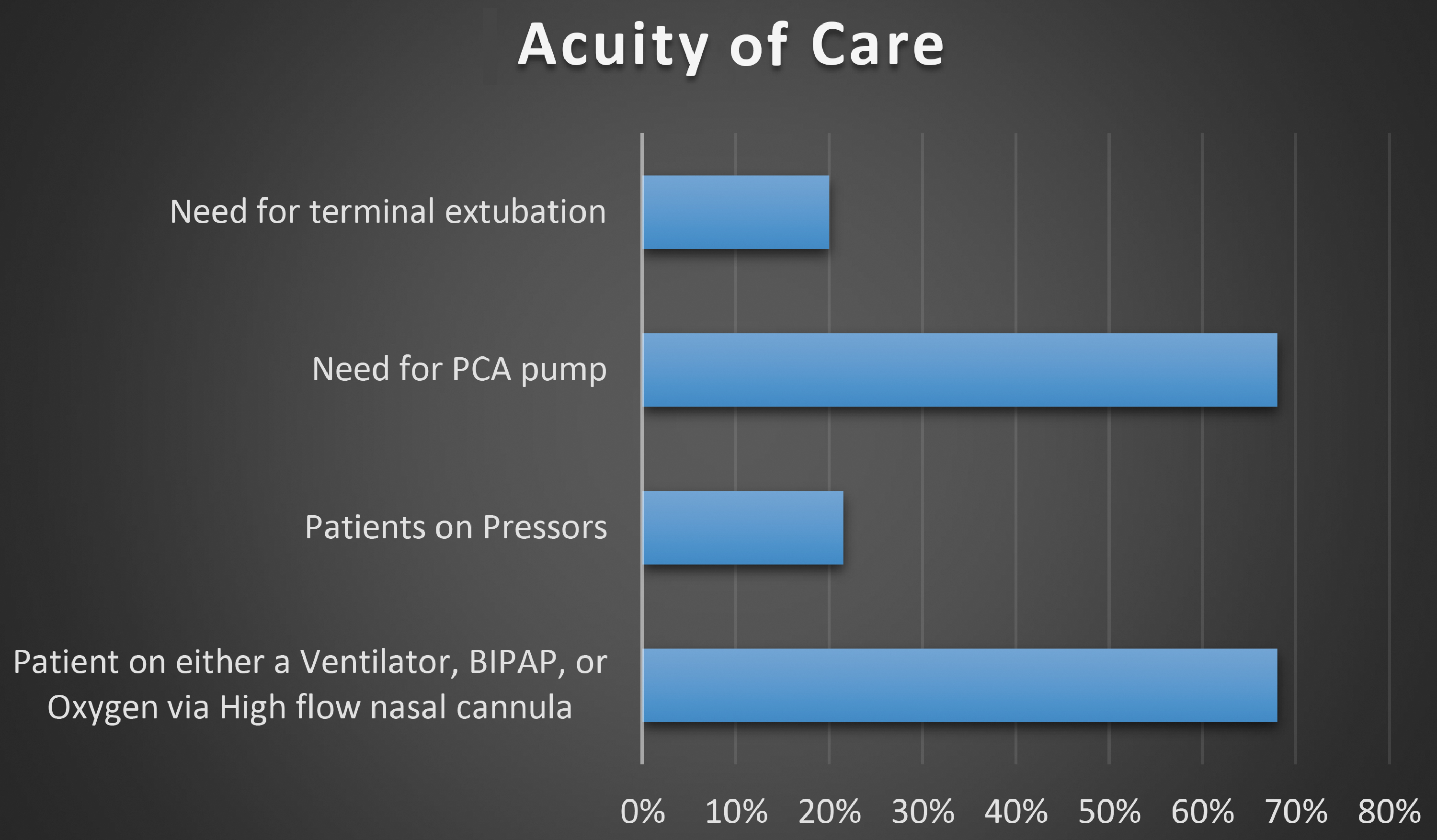
Acuity of care.
Implementation
It has been suggested that four key elements, characterized as “stuff, staff, space, and systems,” are needed to meet increased demand for palliative care capacity during a health crisis. 5 Using these four categories as the framework, we describe our successful PCU conversion into a COVID-19 care unit.
Systems
The key systems factors and indicators that determined the timing of our unit conversion and accepting COVID-19 patients are described in Table 1.
System Factors and Indicators
COVID-19, coronavirus disease 2019; ICU, intensive care unit; LOS, length of stay.
Space
With guidance from the infection control department, we transformed our PCU into a mixed population end of life single room occupancy unit. (Note: geographic case clustering can also be implemented when there is no existing unit.) Table 2 outlines space modification goals, and resources and implementation strategies to achieve these goals.
Space Modification
PPE, personal protective equipment.
Staff
Four domains should be considered to address staffing issues: staff education, team size, nursing ratio, and environmental sanitation.
Staff education
Nursing education should include end-of-life (EOL) symptom assessment, isolation precautions, and medication delivery/extended pump training. At MSH, specialized teams gave frequent COVID-19 updates on number of cases, changing policies and practice, medication delivery protocols, and extended personal protective equipment (PPE) use.
Team size
As patient turnover increased, an extra geriatric attending, a fellow, and a nurse practitioner (NP) were added to help care for patients at end of life. The clinical team's workflow included (1) patient selection and triaging in collaboration with palliative care consult teams, 24 hour palliative care support line, 6 emergency department, and referrals from community and other facilities; (2) bedside clinical care; and (3) collaboration with inter-disciplinary team (IDT) and nursing staff to coordinate video/audio and physical visits and daily clinical updates for families.
Nursing ratio
We anticipated that staff workload could be predicted by estimating the volume of daily transfers to the unit and number of daily expected deaths. At the peak of the surge, the weekly patient volume doubled the pre-COVID-19 average, including patients requiring ventilator support. Given these projections, we established and maintained a maximum nurse-to-patient ratio of 1:4.
Environmental care
We worked collaboratively with unit environmental care specialists to assure safety for clinical teams; care stations and all unit surfaces were cleaned every two hours during business hours, with reduced frequency at night.
Wellness
Given the physical and emotional toll of the pandemic, planning focused on meeting staff needs. Palliative care social workers and chaplains created weekly “coffee chats,” a safe and supportive forum for staff. A quiet space for personal reflection was identified. Palliative care leadership made weekly outreach calls to staff, providing support and offering wellness resources.
Stuff (medications, equipment, and policies)
Medication administration protocols
Factors taken into account were medication availability and frequency of medication administration. To minimize staff risk, scheduled medication administrations were minimized and, whenever possible, with drips located outside of the patient rooms. If medications were being administered at scheduled intervals, adjunct medications were scheduled at the same intervals.
Modified clinical management protocols
Agitation, shortness of breath, and delirium were common symptoms. Agitation increased the risk of patients removing their oxygen masks/cannulas. As a result, haloperidol and lorazepam were important in the end-of-life care for these patients. The palliative extubation protocol was modified to reduce risk of staff infection (Table 3).
Modifications to Medication Management and Clinical Protocols
ET, endotracheal tube.
Discussion
Our patient demographic pattern was consistent with regional COVID-19 demographics for age and gender. Transfer to the unit was only feasible for patients stable enough to be moved. The high level of acuity of these patients and the rapid turnover rate justified our robust staffing ratio. Patients with relatively longer LOS were able to receive supportive care from chaplaincy, and Zoom sessions with family members. In-person visits were permitted for actively dying patients. The volume of admissions and relatively short unit LOS helped maintain availability of both general medicine and ICU beds.
Other lessons gleaned from our experience include the importance of early planning, especially identifying and monitoring key indicators that will trigger the conversion process. Timely collaborations, particularly with emergency, nursing, palliative care, and engineering departments, are essential to secure operational resources. Coordination between unit leadership, engineering, and IT departments allows for proper space utilization, placement of cameras, monitors, and negative pressure devices. Staffing may be a challenge, especially if there is insufficient time to train the required workforce. When gaps in staff knowledge and skills are identified, mobile ID and specialized nursing teams may be available for staff education. Nurses “floated” to a unit can also be paired with previously trained nurses. Offering psychosocial support to staff and sustaining clinician well-being must be a priority. A “resilience room” equipped with soft music and appropriate lighting and books can be set aside on the unit for staff.
Conclusion
Published descriptions of methods and benefits of colocating patients at the end of life during pandemic conditions are lacking. We believe that these operational insights gained from transforming our PCU during COVID-19 will be helpful to other programs and institutions during this pandemic, or in future public health emergencies.
Footnotes
Funding Information
No funding was given.
Author Disclosure Statement
No competing financial interests exist.