
Abstract
Objective:
The objective of this study was to explore the feasibility of monitoring actively dying patients hospitalized in a palliative care unit using a nonwearable sheet-type monitor that measured the state of sleep and vital signs per minute. In addition, we aimed to clarify the incidence of increased respiratory rate and its relationship with survival time.
Design and Measurement:
This study was conducted at a 51-bed palliative care unit in Japan from April 2018 through October 2019. Actively dying patients hospitalized in the palliative care unit were eligible to participate. Increased respiratory rate was measured by Nemuri SCAN, and patient's information was extracted from their medical records.
Results:
In this study, 23 patients were monitored until death; 19 patients with an observational period of 7 days or longer (163 patient days in total) were included in this analysis. There were no adverse events due to use of the nonwearable device. The cumulative incidence of increased respiratory rate (defined as more than 30 respiratory rate per minute) was 63.16% during the observational period, and the mean time between appearance of increased respiratory rate and death was 4.17 ± 4.04 days.
Conclusion:
This study clearly shows that hospitalized actively dying patients can be monitored using a nonwearable sheet-type monitor that measures sleeping state and vital signs per minute. Further studies are needed to utilize these noninvasive continuous monitoring devices in daily clinical practice.
Introduction
Patients with cancer who are actively dying have various symptoms such as pain, malaise, and dyspnea.1,2 In this study, actively dying was defined as the hours or days preceding imminent death, during which time the patient's physiologic functions wane. 3 Close monitoring is considered necessary at the end of life because the state of actively dying patients is unstable. In the clinical end-of-life care setting, continuous monitoring (including electrocardiographic monitoring) is often not performed because of the burden on the patient. Patient assessment is conducted manually by nurses and doctors, but it is difficult to monitor patients continuously and comprehensively. Some studies have claimed that unnecessary monitoring should be discontinued because it causes stress for patients and their families and decreases the patient's quality of life. 4 Although a previous study that monitored patients admitted to a palliative ward using wearable monitors claimed that monitoring was important to improve assessments in palliative patients, 5 it remains challenging to monitor patient's condition properly until the end of their life using nonwearable monitors.
In recent years, techniques for nonwearable or noninvasive monitoring of a patient's state have been introduced. One example of nonwearable monitoring is a sheet-type monitor that is laid under the person's mattress to detect body movement. 6 This nonwearable actigraph was used as a tool to monitor patient's body movements and promote postural changes by caregivers to prevent pressure ulcers. However, that study only involved two patients who had lung cancer admitted in palliative care unit in Ottawa, and they were recorded discontinuously for 14 hours. 6
Two studies examined the prognostic utility of the respiratory rate in actively dying patients with cancer,7,8 although they did not measure the respiratory rate continuously (i.e., once or twice a day). In addition, although increased respiratory rate is observed at the end of life, 9 the clinical significance of this remains unclear. Therefore, we conducted a prospective study to examine the feasibility of continuous monitoring of actively dying patients hospitalized in a palliative care unit using a nonwearable sheet-type monitor (Nemuri SCAN) that monitors patient's body movement, heart rate, and respiratory rate on a minute-by-minute basis. In addition, we used the continuous monitoring data to describe the clinical utility of increased respiratory rate, which is sometimes observed in the dying phase and is assumed to be respiratory compensation of metabolic acidosis.
Materials and Methods
Setting and participants
This study was part of the sensing research projects involved in creating a model that integrated and analyzed biological, behavioral, and practical information to predict patient status. It was conducted in a 51-bed palliative care unit in Japan (Approval number: 1741110). The entry period was from April 2018 through October 2019, and the follow-up continued until the patient died. Palliative care physicians enrolled patients with an estimated life expectancy of a few weeks, as determined by clinical judgment and prognostic models such as the Palliative Prognostic Index 10 and the Palliative Prognosis Score. 11 Patients were enrolled in the study if they or their family members (if the patient's decision-making capacity was impaired) agreed to participate in this study. We could not approach some patients who by a sudden deterioration of their condition, had serious distress, severe dementia, or could not be approached because of the absence of a key person. In this study, only three sets of sensing devices were available, and it was not possible to enroll a fourth patient. Patients who were expected to die within a few hours were excluded from the study. The patients who were investigated for less than seven days were excluded to comprehend the symptom change near death.
Sensing devices
This study used Nemuri SCAN (NN-1100; Paramount Bed Co., Ltd., Tokyo, Japan), which can continuously monitor a patient's condition without any physical contact (Fig. 1). Nemuri SCAN is a sheet-shaped body vibrometer that contains a highly sensitive pressure sensor and is placed under the patient's mattress. This device determines the state of sleep, arousal, and time out-of-bed by measuring amount of activity, respiratory rate, and heart rate per minute. The reliability and validity of Nemuri SCAN are guaranteed.12,13
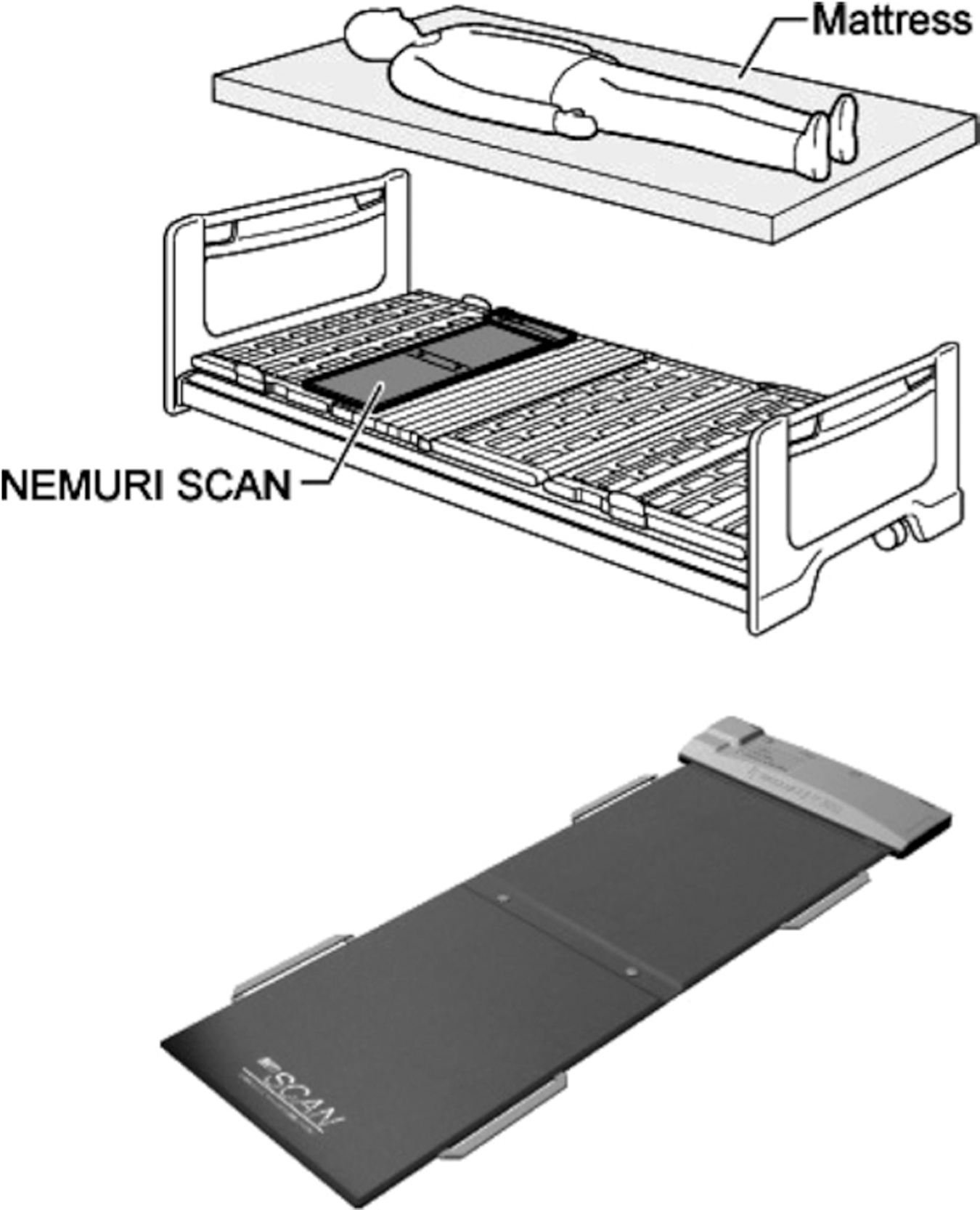
Nemuri SCAN (NN-1100; Paramount Bed Co., Ltd., Tokyo, Japan). 12
Measurements
In this study, the time of death was defined as the time at which the patient's medical record stated a death diagnosis by a doctor. Moreover, one day before death was defined as from the time of death to 24 hours before death. We investigated the following independent variables each day.
Independent variables
Independent variables were extracted from patient's medical records. Age, sex, and primary cancer site were recorded for patient characteristics.
Symptoms of terminal cancer patients were extracted as a reference from a previous study. 1 Four items were extracted from the medical records: use of drugs, symptoms, clinical signs, and nurse-measured vital signs. Each item was evaluated within one day. The use of drugs included four items: opioids, nonopioids, sedative-hypnotics, and artificial hydration. The symptoms consisted of six items and were evaluated as binary data: pain, dyspnea, malaise, restlessness, nausea, and dry mouth. The clinical signs consisted of eight items and were also evaluated as binary data: painful expression, cough, sputum, cold limbs, edema, oral fluid intake, oral food intake, and delirium. Six vital signs (as measured by nurses) were collected: body temperature, fever over 38.0°C (presence/absence), respiratory rate, heart rate, systolic blood pressure, and diastolic blood pressure. A standardized procedure for measuring vital signs was followed in the palliative care unit. Blood pressure and heart rate were measured with an automatic sphygmomanometer, and respiratory rate was doubled after obtaining measurements for 30 seconds. These vital signs were used as continuous values. When the nurses measured vital signs multiple times a day, we recorded the maximum value for that day. Two nurses (K.I. and S.F.) read each medical record and extracted clinical data separately, after which they compared the acquired data and arrived at a consensus if the comparisons did not match.
Outcomes
The outcome variable was increased respiratory rate. Increased respiratory rate was evaluated as a binary variable that was determined as a respiratory rate of 30 or more breaths per minute 14 at least once a day. Andersen defined severely abnormal respiratory rates as ≤8 or ≥30 breaths per minute. 14 However, in this study, we only used a respiratory rate of 30 or more breaths per minute to explore the clinical utility of increased respiratory rate in the dying phase, as this is assumed to indicate respiratory compensation for multiple organ failure-related metabolic acidosis. 15
Statistics
Data measured by Nemuri SCAN and information from patient's medical records were integrated in chronological order. First, we calculated descriptive statistics for patient characteristics, use of drugs, symptoms, clinical signs, and nurse-measured vital signs to clarify the background of the patients. Next, a descriptive plot of the cumulative incidence of increased respiratory rate was used to reveal the relationship between increased respiratory rate and prognosis. To examine the predictive factors for developing increased respiratory rate after three days, odds ratios were calculated with repeated measures logistic regression analysis using a generalized estimating equation. Variable selection was performed through univariate analyses using Student's t-tests or chi-square tests. Variables that indicated a statistically significant difference (p < 0.05) between those who developed increased respiratory rate after three days and those who did not were chosen as independent variables in the multivariate analysis model. All analyses were performed using SAS version 9.4 (SAS, Institute, Inc., Cary, NC), and p < 0.05 was considered significant.
Ethical considerations
This study was conducted with the approval of the Ethics Review Committee of Intervention Studies and Observational Research, Osaka University Hospital (Approval number: 1741110). After explaining the study protocol to eligible patients, written informed consent was obtained from each patient. Participation in the survey was voluntary, and patients were informed that all data would be anonymous and their privacy and personal information would be protected. If a patient did not have sufficient mental capacity to decide about study participation, written consent was obtained from the patient's family/proxy.
Results
Participants
In total, 23 patients who met the inclusion and exclusion criteria were included in this study. Of these, four patients were excluded because of one or more days of missing data from the nonwearable sheet-type monitor. The remaining 19 patients (163 patient days) were included in this analysis. There were no adverse events due to use of the nonwearable device, and all patients completed monitoring procedures until death.
Patient characteristics are summarized in Table 1. The mean age of the participating patients was 76.5 ± 10.5 years; there were 10 males and 9 females. The pancreas was the most frequent primary cancer site (n = 4), and none of the patients who met the inclusion criteria had respiratory organs (lung/thorax) as a primary site. Drugs used in the observational period were opioids (n = 11, 57.9%), sedative-hypnotics (n = 9, 47.4%), and nonopioid analgesics (n = 11, 57.9%). Within the observational period, eight patients had a body temperature of 38.0°C or higher. Table 2 shows the distressing symptoms recorded during the observational period. The main distressing symptoms were pain (n = 16, 84.2%), dyspnea (n = 10, 52.6%), malaise (n = 18, 94.7%), and delirium (n = 12, 52.6%).
Participants (N = 19)
SD, standard deviation.
Distressing Symptoms within the Survey Period (N = 19)
Relationship between increased respiratory rate and prognosis
Figure 2 illustrates the cumulative incidence of increased respiratory rate. In the observational period, 12 patients (63.16%) developed an increased respiratory rate. The onset of increased respiratory rate was most frequently observed within one day before the patient's death (n = 5, 26.32%), followed by four days before the patient's death (n = 3, 15.79%). The median survival time after onset of increased respiratory rate was 3.5 days.
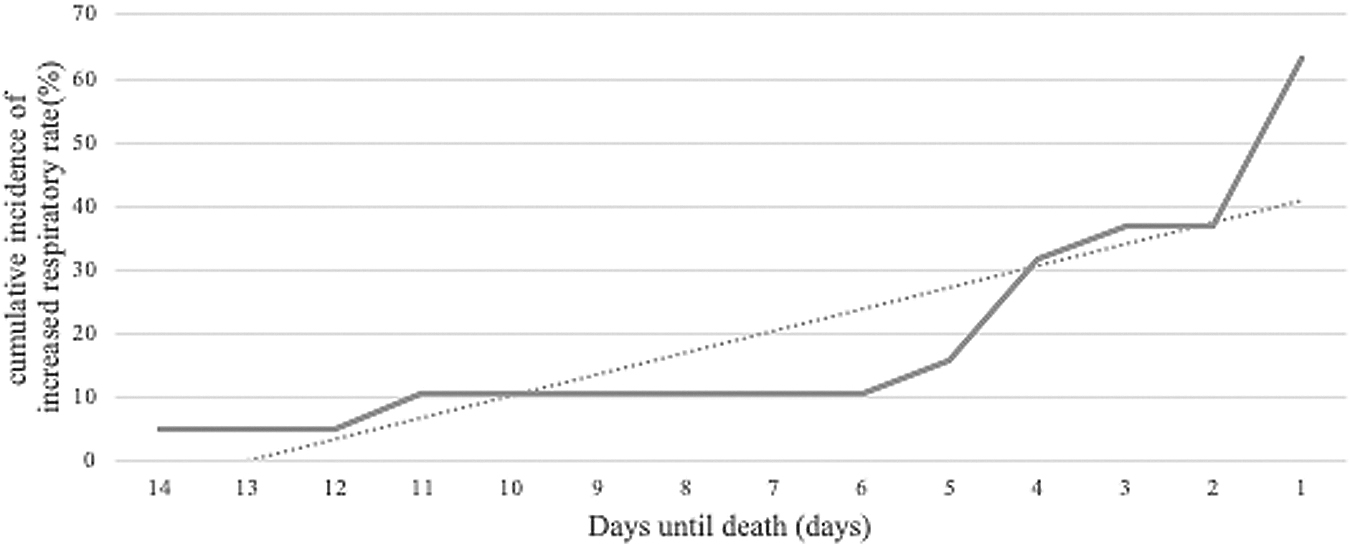
Cumulative incidence of increased respiratory rate.
Predictive factors for increased respiratory rate
In the univariate analyses (Table 3), age (p < 0.0001), opioids (p = 0.0029), artificial hydration (p = 0.0069), pain (p = 0.0426), sputum (p < 0.0001), oral fluid intake (p = 0.0497), systolic blood pressure (p < 0.0001), and diastolic blood pressure (p = 0.0309) showed significant differences between patients who developed an increased respiratory rate and those who did not. In the multivariable-adjusted model (Table 4), significant predictive factors for increased respiratory rate after 3 days were opioids (odds ratio 0.29, p = 0.0086) and systolic blood pressure (odds ratio 1.05 per 1 mmHg, p = 0.0397).
Relevant Factors for Increased Respiratory Rate after Three Days: Univariate Analysis (N = 163 Patient Days)
Relevant Factors that Increased Respiratory Rate after Three Days: Multivariate Analysis (N = 163)
CI, confidence interval.
Discussion
This preliminary study demonstrated that monitoring actively dying patients using a nonwearable sheet-type monitor was safe and feasible. The incidence of increased respiratory rate increased closer to the patient's death, and this phenomenon was closely related to limited survival (median survival time of 3.5 days from onset). No opioids administration and elevated systolic blood pressure were significantly associated with the occurrence of increased respiratory rate in the dying phase. One of the main purposes of this study was to determine the feasibility of using a nonwearable sheet-type monitor that measures sleeping state and vital signs per minute for actively dying patients who were hospitalized in an inpatient palliative care unit. There were no adverse events due to use of the nonwearable device in this study, and no dropouts due to adverse effects related to the device. The nonwearable sheet-type monitor was placed under the patient's mattresses. This study suggested that using the nonwearable sheet-type monitor may improve patient safety without the excess discomfort and restraint associated with contact-type monitoring measures such as continuous cardiac monitoring. Further research is needed to clarify the safety and comfort of this nonwearable sheet-type monitor.
Several studies have reported that the actively dying patients have breathlessness severity during the last week of life, 16 and dyspnea in people who could not report respiratory distress for themselves was measured objectively by a Respiratory Distress Observation Scale. 17 Studies regarding breathing on the final day of life have been conducted; however, only a few studies have quantitatively and continuously captured respiratory rate, and the results of the available studies were inconsistent. Although two studies conducted in palliative care settings indicated that respiratory rate fluctuated before death,8,9 another study conducted in an acute palliative care unit at a tertiary cancer care hospital revealed that respiratory rate was relatively constant during the final days of life. 7 These studies focused on the respiratory rate of actively dying patients with cancer by measuring the respiratory rate in the morning and evening 7 or on the day of admission, 8 so they showed limited ability to detect changes in the respiratory rate in the dying phase. Continuous measurement using a nonwearable sheet-type monitor is a promising technology to reveal the trajectory of respiratory rate at the end-of-life and its clinical importance.
Increased respiratory rate is often observed in actively dying patients and is considered to reflect respiratory compensation of metabolic acidosis due to multiple organ failure or circulatory failure, 15 and is not necessarily pathological. We explored some predictive factors for developing increased respiratory rate. Patients without opioid administration had a higher risk for occurrence of increased respiratory rate than those with opioid administration. Increased respiratory rate may in itself be a sign of distress, and the absence of opioid administration may be evidence of inadequate treatment of respiratory distress. Opioid administration in appropriate doses based on individual patient characteristics may improve distress, which may decrease increased respiratory rate. High systolic blood pressure was also identified as a significant predictive factor for increased respiratory rate. Although it is difficult to estimate the direct relationship between elevated blood pressure and changes in respiratory status, further research is needed to determine whether systolic blood pressure can be a surrogate marker for some forms of end-of-life distress.
Limitations
Although monitoring actively dying patients using nonwearable sheet-type monitors in a noninvasive and continuous way until death may be feasible, the present study had some limitations. First, the preliminary nature of this small-scale study using a convenience sampling should be noted. Because this study did not consider the individuality of demographic data, the findings should be confirmed and expanded in further large-scale studies. Second, patient information in this study might have been underestimated, and this study did not consider the individuality of demographic data because this information was extracted from medical records and half of the patients had delirium, although the variables included in the final model were factors that were less prone to bias. After a patient lost lucidity, symptoms were assessed by objectively based on clinical observations. Third, in this analysis, although we considered the adjustment of repeated measurement, the same participant data were counted multiple times. Therefore, the results of some cases might have a major influence on the overall findings. Fourth, this study was conducted in one palliative care unit in Japan, and data were only collected from patients with cancer; therefore, the generalizability of this study is limited. Finally, this study may have picked up a transitory increased respiratory rate. Nevertheless, even transitory increases of more than 30 in the respiratory rate may have clinical significance. Although we could not fully rule out transient increases in respiratory rate, we believe that the instability of the respiratory rate (i.e., a transient increase in respiratory rate to 30 or more) itself might have clinical implications for detecting a limited prognosis.
Conclusions
This preliminary study clearly shows that it is feasible to monitor hospitalized actively dying patients with a nonwearable sheet-type monitor that measures sleeping state and vital signs per minute. Furthermore, the findings showed an association between increased respiratory rate and prognosis, meaning increased respiratory rate may be a predictive factor for prognosis. The nonwearable sheet-type monitor has potential to improve the quality of life and end-of-life experiences of patients and family members.
Footnotes
Authors' Contributions
S.F. designed the study and management. K.I. and I.M. conducted data collection. K.I. and S.F. led the analysis. K.I. and I.M. drafted the report. All authors read and approved the final report.
Acknowledgments
We thank Miyae Yamakawa, Momoe Utsumi, Akari Higuti, Youko Higami, Haruka Tanaka, Tatsuto Suzuki, Masanobu Kawazoe, Mamoru Okumoto, Nobuhiro Nakamura, Yutaka Hatano, Wataru Mori, Garaashia Hospital, Naoko Otsuki, Etsuko Ohama, Yuki Moriki, Ayami Miyateke, Sonoko Ito, Katsura Kimiko, and Miho Tateishi from our project team, and Audrey Holmes, MA, from Edanz Group (![]() ) for editing the draft of this article.
) for editing the draft of this article.
Funding Information
This study was funded by the DAIKIN research fund and Grant-in-Aid for Scientific Research B (18H03112).
Author Disclosure Statement
No competing financial interests exist.