
Abstract
Introduction:
The Patient Dignity Inventory (PDI) is a reliable screening instrument for a variety of problems (physical, existential, and social) that affect the dignity of patients during their end of life. The PDI has been translated into several different languages and has been validated in different settings. As such, it is important to validate the instrument in patients with cancer in Mexico to assess dignity in this population. The aim of this study was to translate and validate the Spanish version of the PDI in Mexican patients with cancer.
Methods:
This is a cross-sectional study that included patients with cancer, both those enrolled and not enrolled in palliative care, at the Instituto Nacional de Cancerología in Mexico City from September 2018 to August 2019. A translation and back translation were performed to obtain the Mexican version of the PDI (PDI-Mx) instrument. Patients completed the PDI-Mx, the Hospital Anxiety and Depression Scale (HADS), and functional scales (Eastern Cooperative Oncology Group [ECOG] and Karnofsky). Psychometric properties were evaluated by determining internal consistency, exploratory and confirmatory factor analysis (CFA), and concurrent validity with the HADS.
Results:
We included 290 participants with cancer (145 in palliative care and 145 not enrolled in palliative care). The Cronbach's alpha of the PDI-Mx was 0.95. There was a significant correlation with the HADS (rs = 0.757, p < 0.0001). The factor analysis showed four factors that explain 64.7% of the model. The CFA presented adequate indicators, which show the adjustment of the structure that indicates a balanced and parsimonious model.
Conclusions:
The Mexican version of the PDI shows adequate psychometric properties in patients with cancer. We suggest the use of PDI-Mx in clinical care and research.
The study was approved by the Institutional Review Board and Ethics Committee with numbers (016/063/CPI) and (CEI/1115/16) respectively.
Introduction
Dignity has been described as the essence of being human. Humans are characterized by elements of creative intelligence and free rationality; with physical, social, emotional, and cultural dimensions and a desire to transcend life itself.1,2 Dignity encompasses a quality that is innate and cannot be replaced by any other characteristic. As such, dignity is not of relative, but of absolute value. 2
Different subtypes of dignity have been described, including ontological and attributed dignity. Ontological dignity is grounded within the person. From this perspective, human beings deserve respect by the mere fact of being human, and hence must be treated in a qualitatively different manner than other living entities.3,4 The notion of attributed dignity refers to the worth, stature, or value that human beings confer upon others by acts of attribution.5,6
Human dignity has been the subject of much study, and represents an important facet of health care, particularly for patients who are at the end of life.3,7 One of the main challenges faced by health professionals who are dedicated to the care of patients with cancer is to identify problems that may cause suffering and represent an assault on dignity. 8 The provision of quality care is predicated on a deep understanding of the experiences faced by patients with serious, life-threatening conditions, including any potential cause for suffering (physical, psychological, spiritual, or existential), alone or in combination. 8 It is necessary to have a repertoire of instruments that can aid in exploring the impact of disease on patients.
Previously, Chochinov et al. developed a model to explain the perceived loss of dignity for patients with advanced cancer, where dignity was comprised of three factors: (1) factors associated with the disease; (2) social factors; (3) and psychological and spiritual considerations. These factors can be evaluated through a well-validated instrument, the Patient Dignity Inventory (PDI).9,10
The PDI is an instrument originally written in English, which contains 25 items encompassing five factors including symptom distress, existential distress, dependency, peace of mind, and social support. It entails Likert-type answers with a 5-point scale, which ranges from 1, “not a problem,” to 5, “an overwhelming problem”; for this instrument, higher scores indicate higher dignity-related distress. 10
Following its original implementation in English, the PDI has been translated and validated to different languages, including a validation performed in Spain by Rullán et al. in 2015. In this study, 124 patients were included, and results highlighted an internal consistency by Cronbach's alfa of 0.89, and adequate correlation with different instruments. 11 Nonetheless, there are several relevant differences in the colloquial use of language in Spain (Spain-Spanish) and Mexico (Mexican-Spanish), which could impair adequate understanding of this tool in Mexican patients with cancer.12,13 In other validations, the factor analysis has most commonly shown 4 and 5 components. The most frequently reported components being loss of meaning of life, anxiety and uncertainty, and loss of autonomy, with internal consistency values in most, which exceed 0.90.14–18
The PDI instrument has a significant and theoretically relevant correlation with other instruments that evaluate depression, demoralization, functional status, 11 well-being, and quality of life,19,20 the main instrument with which it has been previously correlated is the Hospital Anxiety and Depression Scale (HADS).11,21,22
The objective of this study was to translate, adapt, and validate the PDI instrument in Mexican patients with cancer.
Methods
Study design
This is a cross-sectional, observational, study. Nonprobabilistic convenience sampling was used to include patients from the Instituto Nacional de Cancerología in Mexico City (INCan), a large third-level nation-wide cancer reference center.
Study purpose and the data protection policy were detailed in a printed form accompanying the instruments. The study was approved by the Institutional Review Board and Ethics Committee (016/063/CPI) (CEI/1115/16).
Study participants
All patients attending any outpatient oncology consult at the INCan from September 2018 to August 2019 were approached to participate; the patients approached for participation included patients currently undergoing palliative care as well as patients not receiving palliative care at the time. Inclusion criteria were a histologically confirmed cancer diagnosis, regardless of tumor type and location, age ≥18 years, ability to read/write in Spanish, and a functional status 0–3 on the Eastern Cooperative Oncology Group (ECOG) scale 23 and ≥50 on the Karnofsky scale. 24 It should be highlighted that patients could participate in this study whether they were receiving palliative care or not.
Patients who fulfilled inclusion criteria were invited to participate and asked to sign an informed consent. Exclusion criteria included patients with delirium, hearing problems, and/or severe visual impairment, inability to understand or complete the questionnaires, or a critical illness besides cancer.
Procedures
Cultural adaptation of the PDI instrument
The PDI instrument in its original form was obtained from the original publication. 10 We obtained permission from the original authors to translate the instrument for academic and research purposes. The translation and cultural adaptation were performed according to the guidelines established by the World Health Organization, in accordance with the European Organization for Research and Treatment of Cancer (EORTC) approach. 25 The original instrument in English was translated by a native Mexican-Spanish speaking professional translator, and this version was then revised by a native Mexican Spanish-speaking expert, who also speaks English. Next, a third independent translator was summoned for the final revision. This third independent translator is a bilingual speaker with expertise in mental health (psychologist) and translations. A team comprising mental health experts (including psychologists and psychiatrists at the INCan) met to compare the original PDI and the translated versions. Idiomatic phrasing and conceptual as well as cultural equivalence with the original version were ensured. The final version of the instrument was back translated to English by a certified translator and sent to the original author of the PDI for overview and acceptance, therefore establishing the Mexican version of the PDI (PDI-Mx) (Supplementary Data). A pilot study was then performed with 30 participants, in which comprehension, instruction clarity, and item clarity were considered. 26
Application of the PDI-Mx instrument
Once all adjustments had been made, the PDI-Mx was given to all consenting study participants. The study population included patients ranging from those under surveillance after treatment, to patients with advanced cancer undergoing palliative care. To evaluate concurrent validity, the HADS was administered at the same time as the PDI-Mx. The HADS has been previously validated in Mexico. 27
Data analyses
Characteristics of the study population are presented with descriptive statistics, including clinical, social, and demographic variables, as means, standard deviations (SD), and interquartile ranges (IQRs), as well as absolute and relative frequencies according to each variable type. A Spearman correlation was performed between the PDI-Mx and sociodemographic and clinical characteristics. An exploratory factor analysis (EFA) with orthogonal (varimax) rotation was performed. Likewise, internal consistency was assessed for multi-item correlation using Cronbach's alpha. A p-value ≤0.05 was considered statistically significant. Following the EFA, the adjustment was evaluated through a confirmatory factor analysis (CFA) using the maximum likelihood method, which included the identification and specification steps for the model, estimation of standardized parameters (R 2 correlations, covariance, modification indices, and difference proportion critical value). Finally, the adjustment was evaluated considering the acceptable limits of the estimators, as well as collinearity in the variables. The following indices for global adjustment were taken into consideration: Chi-squared test and the proportion of chi-squared goodness-of-fit index (GFI) and its complements (adjusted GFI and Tucker-Lewis Index [TLI]), as well as the comparative GFI (comparative fit index [CFI]). Last, we calculated the root mean square error of approximation (RMSEA).23–25 All analyses were performed using SPSS version 21 for Windows (IBM Corp., Armonk, NY).
Results
Patients
A total of 312 patients were screened for inclusion. Among these, 290 patients met inclusion criteria and agreed to participate in the study. From the total population, 145 patients were currently attending the palliative care service, while 145 were from other outpatient clinics at the Institute and, importantly, were not currently undergoing palliative care. Most patients were female (69.7%; n = 202/290), and median age was 54 years (IQR: 44–64).
Regarding the disease stage in solid tumors, it should be noted that only 10.2% of the study population were patients with local disease; however, all patients with local disease were in the group of patients not currently undergoing palliative care, at the time of study inclusion. Meanwhile, patients with locoregional or metastatic disease represented 89.8% of the study population; among these, 140 patients were currently undergoing palliative care, while 115 were not undergoing palliative care at the time.
Baseline characteristics are summarized in Table 1.
Baseline Characteristics of the Study Population (N = 290)
ECOG, Eastern Cooperative Oncology Group; IQR, interquartile range.
Exploratory factor analysis
A total of 23 items were left, which were adjusted to four factors, with a Cronbach's alpha value of 0.956. The Kaiser-Meyer-Olkin (KMO) test was used to measure if the data were suitable for factor analysis, with a result of 0.944. Bartlett's sphericity test was also used to identify if the variables were unrelated. The result was statistically significant (χ 2 = 4959.052; gl = 300; p < 0.001). Furthermore, the EFA with varimax rotation explained 64.7% of variance. The PDI-Mx instrument presented a statistically significant association with the HADS (rs = 0.757, p < 0.001). Results from the EFA of the PDI-Mx instrument are summarized in Table 2.
Results from the Exploratory Factor Analysis of the Mexican Version of the Patient Dignity Inventory Instrument
Alpha = 0.956, explained variance = 64.7%.
Confirmatory factor analysis
The ratio between χ 2 /gl for global adjustment (2.398; p ≤ 0.001) shows practically null errors in the variance and covariance of the population-adjusted model. The main GFI (0.865) and CFI (0.927) confirm the model as complex and acceptable, meanwhile the root mean square residual index (0.049) is close to zero, and the RMSEA (0.070; 0.062–0.077) ratifies the model, since they penalize complexity, although the values stay close to 0.05 and 0.08, respectively. This indicates that the model is recursive and correctly overidentified. Results show a structure composed of four factorial components: (1) loss of meaning in life; (2) anxiety and loss of autonomy; (3) dependency; and (4) social support. The factorial and variance load of error explained by each item can be observed in Figure 1. Furthermore, Table 3 summarizes the criteria and interpretation of the complementary indices used.
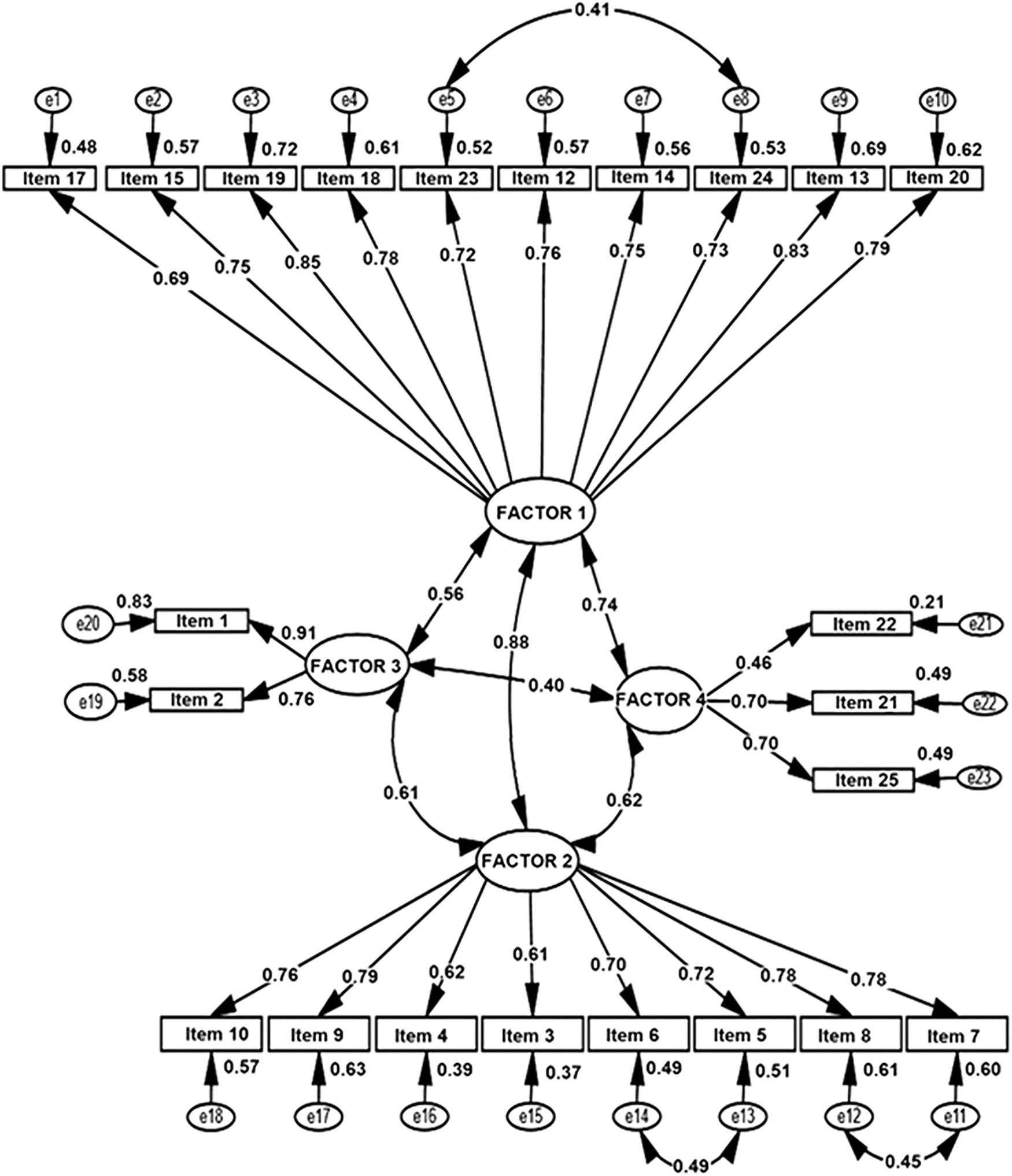
The factorial and variance load of error. First-order CFA of 4 factors for perceived dignity in patients with cancer (n = 290) χ 2 = 530.062, 221 DF, CMIN/DF = 2.398, p = 0.000, CFI = 0.927, PCFI = 0.810, TLI = 0.916, GFI = 0.865, AGFI = 0.831, RMR = 0.049, RMSEA = 0.070 (0.062–0.077), Hoelter, n = 149, (p = 0.01). AGFI, adjusted goodness-of-fit index; CFA, confirmatory factor analysis; CFI, comparative fit index; CMIN/DF, chi-squared/degree of freedom; GFI, goodness-of-fit index; PCFI, Parsimony Comparative Fit Index; RMR, root mean square residual; RMSEA, root mean square error of approximation; TLI, Tucker-Lewis Index.
Criteria and Interpretation of the Complementary Indices Used
CMIN/DF; CFI, comparative fit index; GFI, goodness-of-fit index; RMR, root mean square residual; RMSEA, root mean square error of approximation.
Clinical validation
The PDI-Mx scores presented a significant correlation with clinical variables such as age, the Karnofsky score, and the ECOG functional status. In the case of these aforementioned variables, we observed an inverse relationship. In the case of age, younger patients perceive higher dignity-related distress (Rho: −0.1181; p = 0.045). In the case of performance status, as measured by Karnofsky score and ECOG functional status, patients with higher functionality (in both independently evaluated scales mentioned) had lower PDI-Mx scores (less dignity-related distress).
Patients not undergoing palliative care had a median score in the PDI-Mx of 39 (IQR: 31–54), while patients undergoing palliative care had a median score of 43 (IQR: 33–59); p = 0.0621. Importantly, when stratifying by items, we identified significant differences between those patients undergoing, or not, palliative care in items 1, 3, and 11, referring to not being able to carry out tasks of daily living (p = 0.049), experiencing physically distressing symptoms (p = 0.0001), and no longer feeling like the person they once were (p = 0.01), respectively.
Discussion
Novel cancer therapies continue to emerge yearly, and although many show outstanding results in terms of survival, the impact of these interventions in other aspects of patients' lives remains scarcely explored.28–31 It is important to characterize how diverse interventions will impact quality of life, mental well-being, and social interactions. 32 It is imperative to have robust and validated tools, encompassing biopsychosocial dimensions of illness experience that enable tracking patient distress in the clinical and research setting. Many instruments had been designed and validated in English-speaking patients. Nonetheless, these are issues that transcend culture and geography, which is why these instruments must be validated in other populations. 17
The PDI instrument, based on the Model of Dignity in the Terminally Ill, was developed as a novel approach to evaluate issues pertaining to the dignity of terminally ill patients. Nonetheless, there are important cultural differences, which should be considered when applying these instruments to patients and interpreting results. 33 In this sense, although the PDI instrument had been previously translated into Spanish by Rullán et al. (2015), 11 this version was validated and tailored to European subjects from Spain. There are important cultural differences when considering Spanish-speaking patients from other continents, such as Latin-America, including several terms which are many times difficult to understand for most of the Mexican Spanish-speaking population (including, but not limited to necesidades corporales, personal sanitario, incertidumbre, etc.),12,13 this is also affected by some important demographic differences between populations in Spain and Mexico, including schooling, which justifies a cultural adaptation tailored to these patients.
To the best of our knowledge, this is the first validation of the PDI instrument in patients with cancer from Latin America. The sample included patients with different neoplasms and stages, with some receiving palliative care and others not, thus ensuring a representative and diverse population. The analysis included an exploratory and CFA, further strengthening the value of the study.
Dignity is a complex concept and relevant in every aspect of human life. Assessing dignity in patients with cancer is necessary, especially since fractured dignity is associated with considerable suffering. As such, health professionals must take dignity into consideration, to invoke strategies that can bolster dignity and improve quality of life.10,34
Results from this trial show that the PDI-Mx had a significant correlation with HADS, and we report the highest internal consistency and variance compared with previous studies.11,21,22 Results show a structure composed of four factorial components: (1) loss of meaning in life; (2) anxiety and loss of autonomy; (3) dependency; and (4) social support. These components speak to the disease burden faced by cancer patients, whether receiving palliative care or not. For example, patients often experience existential crises and loss of perspective on the meaning and purpose of life in the context of life-threatening or life-limiting illness. Furthermore, patients clearly confront dependency issues, as reflected in two components (anxiety and loss of autonomy; dependency), highlighting issues that can range from personal dependency to economic dependency, and autonomy to perform daily tasks. Finally, social support is an important factor, as patients may face indifference or even stigma due to their condition, further adding to their burden. The factorial structure of the PDI-Mx instrument in patients with cancer differs from the current literature, although some aspects resemble data reported by Li et al., 16 Kisvetrová et al., 17 and Bovero et al., 18 in terms of the level of internal consistency and variance. Nonetheless, the value for Cronbach's alpha was higher in this study compared with results reported by Rullán et al., 11 although we observed a similar result in terms of the significant correlation with the HADS tool. Interestingly, our results show a trend for a higher PDI score among patients undergoing palliative care, suggesting more dignity-related distress in these subjects relative to those not undergoing palliative, although this result did not reach statistical significance.
In our study, a reduction in the number of items occurs through the EFA, similar to data reported in the original version of the PDI instrument, 10 nonetheless, we chose to maintain all items due to their clinical relevance.
The confirmatory model included four factors with strong association between them, as shown in the exploratory analysis. The more powerful analyses for the model structure portray a well-balanced, parsimonious model, 35 rendering the recommendation of this instrument to evaluate dignity in Mexican patients with cancer, independent of tumor location or disease stage.
Findings from this study establish the usefulness of a valid and reliable tool, which can help assess dignity in patients. Dignity imbues a personal sense of stability and consciousness of individual needs, and helps perceive one's surrounding in a positive manner. 34
This study has limitations that must be considered, including the lack of concurrent validity with other variables, which, theoretically, should correlate with the PDI-Mx. Participants in this study were exclusively cancer patients. Other serious life-threatening diseases should be explored in the future to establish the clinical and diagnostic utility of the PDI-Mx in other patient populations, particularly considering the emotional toll of these conditions, including depression and anxiety.
Nonetheless, the data from this study show that the PDI-Mx instrument can be used in Mexican patients with cancer, both those who are currently receiving palliative care and those who are not. The PDI-Mx can identify dignity-related distress and assess the level of social support, which is accessible to the patient in facing their health condition. Similarly, this tool can aid in identifying patients whose dignity has been undermined, enabling referral for appropriate psychosocial interventions and support.
Conclusion
The PID-Mx instrument is a valid, easy-to-use, brief, and reliable tool for clinical and research purposes. As such, it is of considerable importance that this available tool be used to routinely to identify dignity-related distress among patients with cancer undergoing, or not, palliative care. The consistent use of the PDI tool among this population could aid in planning appropriate psychosocial interventions, which could positively impact the psychological sphere of patients living with cancer.
Footnotes
Acknowledgments
We would like to thank all the patients who participated in this study.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
O.R.-M., O.G.-V., A.L., and S.A.-P. received partial support from Consejo Nacional de Ciencia y Tecnología (CONACyT) Sistema Nacional de Investigadores, and declare no potential conflicts of interest. The rest of the authors do not report actual or potential conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.