
Abstract
Background:
There have been few studies evaluating the costs of palliative care (PC) in low- and middle-income countries (LMICs), especially for patients with cancer.
Objectives:
The objective of this study was to identify the sociodemographic and clinical variables that could explain the cost per day of PC for cancer in Brazil.
Methods:
This was a retrospective cost analysis of PC at a quaternary cancer center in São Paulo, Brazil, between January 2010 and December 2013. Factors influencing the cost per day were assessed with generalized linear models and generalized linear-mixed models in which the random effect was the site of the cancer.
Results:
The study included 2985 patients. The mean total cost per patient was $12,335 (standard deviation [SD] = 14,602; 95% confidence interval [CI] = 11,803 to 12,851). The mean cost per day per patient was $325.50 (SD = 246.30, 95% CI = 316.60 to 334.30). There were statistically significant differences among cancer sites in terms of the mean cost per day. Multivariate analysis revealed that the drivers of cost per day were Karnofsky performance status, the number of hospital admissions, referral to PC, and place of death. Place of death had the greatest impact on the cost per day; death in a hospital and in hospice care increased the mean cost per day by $1.56 and $1.83, respectively.
Conclusion:
To allocate resources effectively, PC centers in LMICs should emphasize early enrollment of patients at PC outpatient clinics, to avoid hospital readmission, as well as advance planning of the place of death.
Introduction
Palliative care (PC) is an interdisciplinary specialty focused on improving quality of life for seriously ill patients and their families through better symptom management and coordination of care, as well as optimal communication among professionals, the patient, and the family.1,2 Studies evaluating economic aspects have suggested that PC results in cost savings during inpatient care and during the end-of-life phase, especially for patients with cancer. 3 However, policymakers should interpret those findings with caution, because there are methodological differences among studies, and there are problems with the analysis, particularly in relation to the skewness of cost data. 4 The heterogeneity among such studies shows the challenges of conducting research in this area, such as defining which core components should be included in the economic evaluations. 5 To characterize patients with regard to resource use and complexity, it is necessary to consider the most important determinants of resource consumption. 6
Like other medical specialties, PC competes for limited and finite resources. Given the unique constraints in low- and middle-income countries (LMICs), payers and policymakers in such countries require evidence to validate the PC currently being provided and to explore ways that it could be made more cost-effective. 7
The majority of the studies evaluating the costs of PC have been conducted in the United States, depicting a privately funded health system. 8 Therefore, their findings cannot be generalized to a mixed private- and public-funded health care system, as exists in Brazil. The core cost components and the perspective from which analyses are undertaken are necessarily context and country specific. There have been few studies attempting to identify factors associated with a higher cost per day for PC in patients with cancer in LMICs, such as patient characteristics, diagnosis, and prognosis.
The objective of this study was to identify the sociodemographic and clinical variables that could explain the cost per day of PC in patients with cancer in Brazil.
Methods
Study design and setting
This was a retrospective cost analysis. The data used here were obtained in a previous study that estimated the cost of PC in patients with cancer treated at the Instituto do Câncer do Estado de São Paulo (ICESP, São Paulo State Cancer Institute), a quaternary teaching hospital in the city of São Paulo, Brazil. 9 The ICESP is a public hospital that works in a formal partnership with the state of São Paulo and the Brazilian Unified Health Care System. Since 2009, it has offered PC services provided by a multidisciplinary team, organized for outpatient, inpatient, and hospice care. Patient care can be integrated into oncologic care or can be provided separately. The ICESP serves ∼3400 patients per year, of whom ∼1500 are referred to PC. 9 This study was approved by the Ethics Committee of the Faculty of Medicine of the University of São Paulo (FMUSP) on June 5, 2019, no. 676 004.
Study population, data sources, and costing
We evaluated data from 2985 patients ≥18 years of age who received PC between January 2010 and December 2013. Sociodemographic and clinical data were obtained from electronic medical records. Because we analyzed the data from the perspective of the health care facility (ICESP), only formal health care sector costs were included: clinical consultations, interdisciplinary consultations, hospital admissions, emergency department visits, intensive care unit admissions, surgical procedures, chemotherapy, medications, laboratory tests, medical supplies, hospital supplies, and hospice care. The unit cost values, at the patient level, were collected from the ICESP administrative database. 9 The cost estimates were given in Brazilian reais (R$) for 2013 and adjusted for June 2018 values through the Consumer Price Index (CPI) 10 and then converted into U.S. dollars for 2018 (US$ = R$3.74) and then converted to international dollars (int-$) using the 2018 Purchasing Power Parity (PPP) exchange rate (2.044). 11 As variables that might explain the cost per day in patients with cancer, we selected the following: age; sex; marital status; level of education; Karnofsky performance status (KPS, a score ≥50 indicating better self-care capacity); referral to PC (yes or no); number of hospital admissions; place of death; site of the cancer; days in hospice; and length of stay (LOS), defined as the time (in days) from entry into PC to death.
Statistical analysis
The cost data for categorical variables are presented as mean and standard deviation (SD), and 95% confidence interval (95% CI) for the mean. We used Student's t tests for dichotomous variables. For categorical variables with more than three categories, we used analysis of variance with Tukey's post hoc test or Bonferroni correction for multiple comparisons. To identify correlations between cost and quantitative variables, we calculated Pearson's correlation coefficient.
We chose the cost per day as the primary outcome, because, in many cases, the SD of the total cost was greater than the mean, indicating wide dispersion of the data. In addition, according to May et al., 12 the mean cost per day used as the primary outcome of interest indirectly limits the impact of unobserved heterogeneity, reducing skew and leptokurtosis, and addressing specific stakeholders, such as a hospital reimbursed a fixed daily rate.
We performed a multivariate analysis to assess the effect that each variable had on the cost per day. The independent variables were sex, age at referral to PC, marital status, level of education, KPS score, referral to PC, number of hospital admissions, place of death, site of the cancer, and days in hospice. We got collinearity tolerances >0.1 and variance inflation factor (VIF) <10, for all the covariates considered as fixed effects in the model, which indicated that there is no collinearity among regressors.
In the modeling process, several adjustments were made, including generalized linear models (GLMs) and generalized linear-mixed models (GLMMs) in which the random effect was the site of the cancer. The GLM is best suited for the integration of high cost to a single model and reduced heteroscedasticity of residuals from ordinary least squares (OLS) regression. Therefore, we chose a GLM that allows a more flexible modeling of costs that are superior to OLS, the most common multivariate regression method. Recently published articles have used this model for cost analysis.6,13,14 We used automatic stepwise variable selection. After seeing the model diagnostics, we selected the final model on the basis of the deviance, Akaike information criterion, and Schwarz Bayesian criterion. Values of p < 0.05 were considered significant. Statistical analyses were performed with the IBM SPSS Statistics software package, version 24.0 (IBM Corp., Armonk, NY) and the program R, version 3.6.1 (R Development Core Team—www.r-project.org). We used the R packages ggplot2 for graphs and gamlss for model fitting. 15
Results
Characteristics of the sample
Table 1 provides the sociodemographic and clinical characteristics of the sample. The mean age of patients at the first PC consultation was 64.4 years (SD = 13.5). The majority were men and married (54.6% and 52.9%, respectively). Data related to the level of education were present in 737 (24.7%) of the 2985 electronic medical records; of the corresponding 737 patients, 659 (89.4%) had at least 9 years of schooling. Of the 2985 patients evaluated, 2308 (77.3%) were hospitalized at least once and 1565 (52.4%) were referred to PC during hospitalization. The majority of the patients (63.4%) died in hospice care. The most common site of cancer was the lung (in 12.4%), followed by the colon or rectum (in 12.3%) and the head or neck (in 11.8%). The mean time in PC care was 72.8 days (SD = 116.8), and the mean time in hospice care was 14.1 days (SD = 30.8).
Cost per Day of Palliative Care, by Sociodemographic and Clinical Characteristics, for Patients with Cancer Treated at the São Paulo State Cancer Institute, 2010–2013
Exchange rate, adjusted for purchasing power parity, in 2018: 1.00 U.S. dollar = 3.31 Brazilian reals; current exchange rate: 1.00 U.S. dollar = 5.36 Brazilian reals.
r = −0.110 in relation to the cost per day.
r = −0.396 in relation to the cost per day.
CI, confidence interval; KPS, Karnofsky performance status; LOS, length of stay; SD, standard deviation.
Costs
The distribution of the formal health care sector costs of the patients who received PC was positively (right) skewed (by 5.5) and overdispersed. The mean total cost per patient was $12,335, ranging from $517 to $262,265 (SD = 14,602; 95% CI = 11,803 to 12,851). After adjustment for LOS, there was no overdispersion (coefficient of variation, 75.7%) and the right skewness decreased (to 1.5). As given in Figure 1, the mean cost per day per patient was $325.50 (SD = 246.30; 95% CI = 316.60 to 334.30).
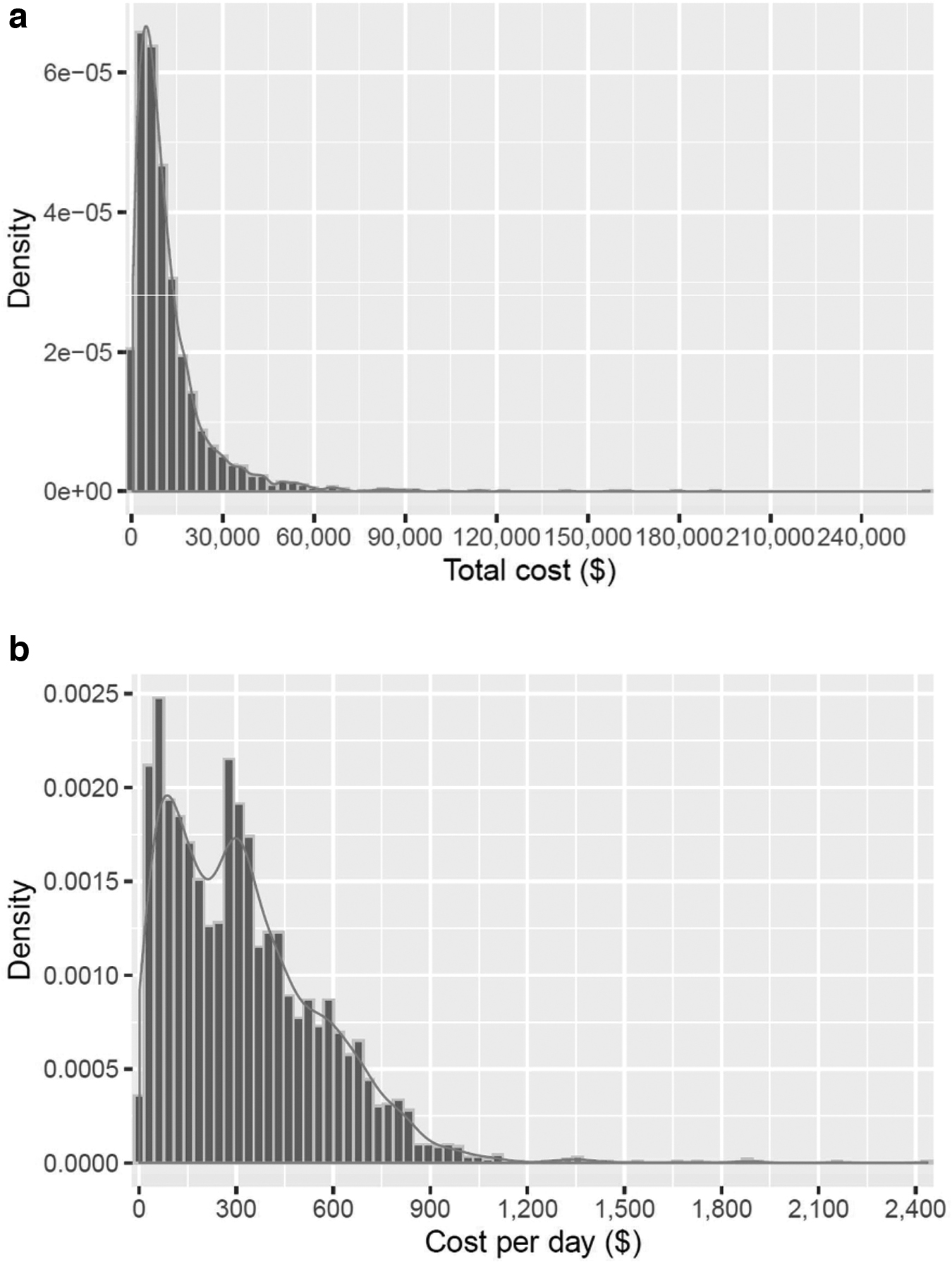
Distribution of total cost per patient
There was a statistically significant difference between one (or more) of the cost per day means for specific cancer sites and “other cancer sites.” Figure 2 provides box plots of the mean cost per day per patient according to the site of the cancer, respectively, showing the variation in the costs with right skewness. The mean cost per day was highest for the sites “other digestive tract locations” ($396.20), bladder ($394.40), blood ($388), and male genital organs ($354.10), whereas it was lowest ($193.00) for cancer located in the thyroid.
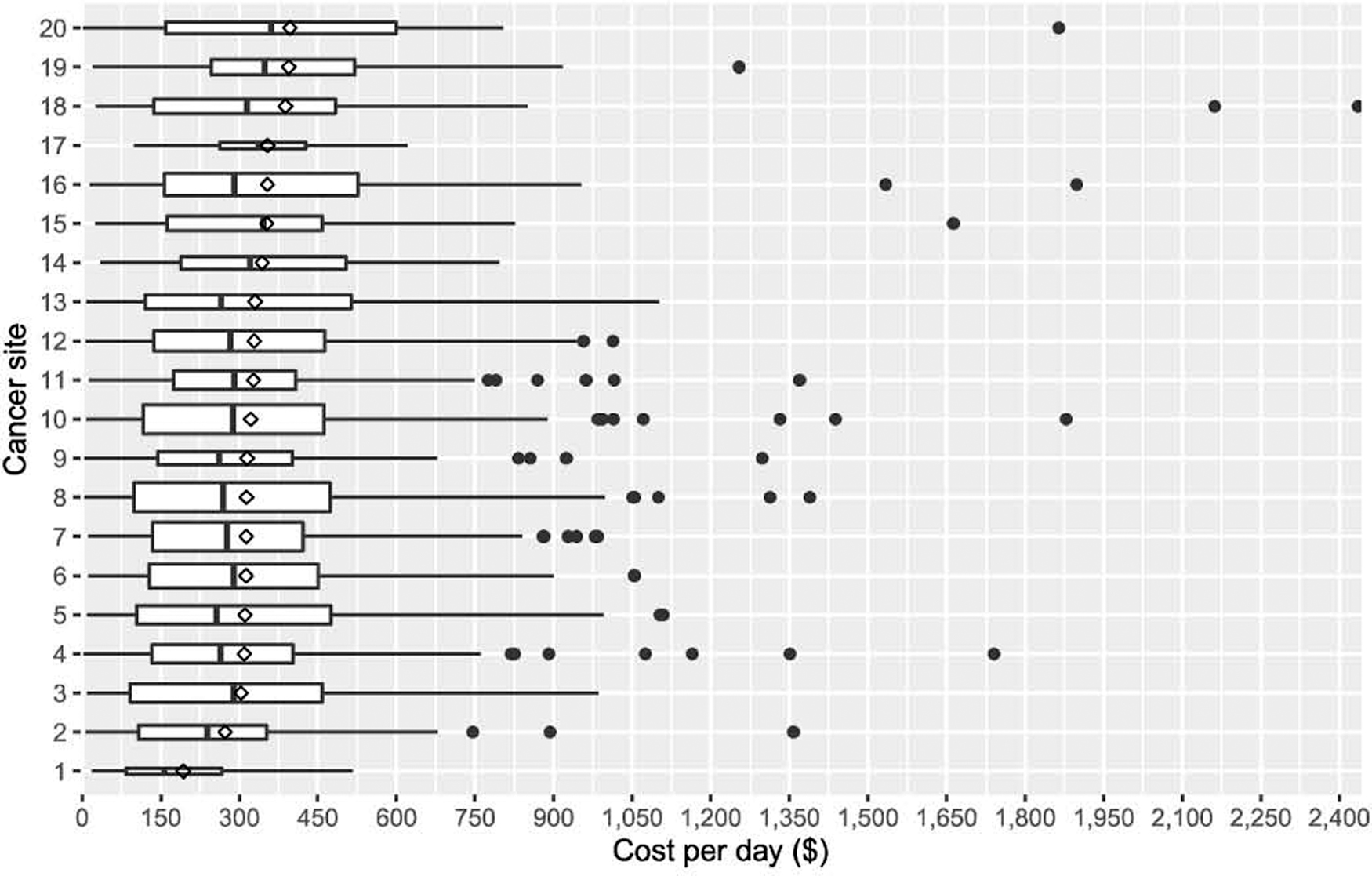
Box plot of cost per day by cancer site, in ascending order by mean cost. 1 (Thyroid) = $193.0; 2 (liver) = $272.9; 3 (other locations) = $303.2; 4 (prostate) = $309.7; 5 (esophagus) = $310.9; 6 (stomach) = $312.7; 7 (head/neck) = $313.3; 8 (colon/rectum) = $313.6; 9 (kidney) = $315.0; 10 (lung) = $321.6; 11 (brain) = $327.2; 12 (female genital organs) = $328.3; 13 (pancreas) = $330.0; 14 (neuromuscular site, not otherwise specified) = $343.8; 15 (melanoma) = $352.1; 16 (breast) = $353.7; 17 (male genital organ) = $354.1; 18 (hematologic) = $388.0; 19 (bladder) = $394.4; 20 (other digestive tract locations) = $396.2. The line in the box represents the median, the diamond corresponds to the mean, and the width of the box is associated with the sample size.
A univariate analysis showed that the following variables showed a statistically significant association with cost per day (Table 1): age, KPS score, referral to PC, number of hospital admissions, place of death, site of the cancer, and days in hospice. The multivariate analysis showed that sex, age, marital status, KPS score, referral to PC, number of hospital admissions, place of death, and days in hospice all had a significant effect on the cost per day (Table 2). Although the effect sizes were small, sex, age, KPS score, referral to PC, and days in hospice all had a desirable effect. The corresponding estimated parameters are negative, meaning that they can decrease the cost per day, although only slightly. The place of death variable had the greatest impact on the cost per day. When death occurred during hospitalization, the mean cost per day was higher by exp(0.446), corresponding to $1.56, compared with exp(0.605), corresponding to $1.83, when death occurred during hospice care.
Gamma Generalized Linear-Mixed Model with Log Link for Costs per Day
ϕ, Dispersion parameter; σb, standard deviation of the random effect; AIC, Akaike Information Criterion; SBC, Schwarz Bayesian Criterion.
Discussion
This study provides preliminary insights into the sociodemographic and clinical variables that explain the cost per day of PC in patients with cancer at a quaternary teaching hospital in Brazil. There was a statistically significant variation in costs depending on the site of the cancer. Multivariate analysis showed that the potential drivers of the cost per day in patients with cancer are the KPS score, the number of hospital admissions, referral to PC, and the place of death.
Our analysis highlights the significant role that the site of cancer plays in understanding variations in health care costs, given that the costs of PC are dependent on patient characteristics such as diagnosis. 16 However, previous studies have shown that the diagnosis does not significantly influence costs.6,14,17 Nevertheless, some of those studies did not select diagnosis for inclusion in multivariate models explaining the cost per episode,6,17 perhaps because of the influence that disparities in health care system and clinical practices have on health care resource utilization.
In accordance with our findings, a study on patient-related costs and factors associated with the cost of in-hospital specialist PC in Germany 7 identified factors explaining cost per episode, such factors including the KPS score, phase of illness (which could be related to the number of hospital admissions), and type of discharge (which could be related to the place of death).
Regarding the KPS score, previous studies have shown that extreme dependence was predictive of higher costs in PC units.6,18 Multivariate models have shown that the phase of illness and KPS score are factors that explain cost per episode. 6 In this study, we found that costs were higher for patients with a KPS score <50 and that a reduction in this score was a statistically significant factor influencing cost per day in the GLMM.
Emergency department visits, hospital admissions, and, in particular, intensive care unit admissions are key drivers of resource use and expenditures in cancer care. 19 Similarly, integrating PC into a hospital setting could have a positive impact on the total budget by lowering the cost per day. A study evaluating a new PC inpatient unit program implemented at Johns Hopkins Medical Institutions showed that performing PC consultations for inpatients reduced the 30-day readmission rate from 15% to 10%. 20 As in this study, these studies showed that number of hospital admissions is a key cost driver, related to intensity of treatment, which could be influenced by a PC program in the hospital setting. A previous cost analysis highlighted the importance of early PC, showing that cost savings from early PC accrue by shortening LOS and reducing the intensity of treatment, shorter LOS being associated with an estimated savings of 63%. 21
In this study, referral to PC was also a relevant cost driver, underscoring the importance of early PC. Our findings show that costs were lower for patients referred from outpatient care than for those referred from inpatient care. Patients referred to PC from outpatient had a reduced number of hospitalizations, and emergency visits, and ingresses earlier in PC service when compared with patients referred during hospitalization. Patient- and family-centered discussions on the goals of care and transition planning initiated by outpatient PC teams in the early phases of disease may be at least as important in driving cost savings as are reductions in the number of unnecessary tests and pharmaceutical use in the later phases. 21 Early PC consultations may be more related to care planning, which could clarify, for the referring physicians, the limited benefit associated with subsequent hospital admissions. Because late PC consultations may be more focused on symptom management and might not address care planning, their ability to influence the intensity of treatment and LOS is probably more limited. 21 Similarly, chemotherapy near death may reflect patient, family, or community preferences and the practice could be opposed by appropriate shared decision making by the treating clinicians, while discussing advanced directives, for instance. 19
Regarding the place of death, dying in a hospital is costly and is often not aligned with patient preferences related to end-of-life care.22,23 One previous study showed that the LOS was longer and the cost per day was higher for those who died during hospitalization than for those who died during hospice care. 24 In contrast, our data show that the mean cost per day was higher for the patients who died in hospice care than for those who died in the hospital. One possible explanation for this difference is late referral to hospice care, which means that patients were in a more advanced phase of the disease. Delayed referral can generate significant additional costs, such as administrative, food, and housekeeping costs, as well as those related to nursing, social counseling, and therapist staff, 8 which, at this phase of illness, are similar in both settings.
The main contribution of this study is that it provides information on the factors that may impact the costs of treating cancer patients in hospital PC units in LMICs. Therefore, the organization of PC services in these countries must consider aspects that are relevant for the management of hospital costs, such as early inclusion of patients in PC outpatient services, preventing hospital readmissions, and planning the place of death, regardless of the site of the cancer and the functional status of the patient.
At the same time, there has been increasing awareness that early discussion of goals of care, patient values, and preferences, as part of an advance care planning process (ACP), has the potential to reduce health care spending on inappropriate or futile interventions at the end of life.25,26 Studies suggest that good planning can improve pain control for patients, allow them a greater possibility of dying at home, less chemotherapy, increase utilization of appropriate hospice services, correlate with fewer hospital admissions, and considerably lower health care costs.27–32 Thus, oncologists and PC specialists must work toward finding the optimal time to discuss end-of-life care options for each patient to achieve high-quality ACP. In this sense, the cost drivers identified in this study may serve as outcomes to assess the impact of ACP implementation in the clinical setting.
Our study has some limitations. First, although it has been suggested that the overall cost of hospitalization is the most useful outcome measure for health managers and is the preferred dependent variable in a primary analysis, 25 we did not evaluate the overall cost as an outcome measure. However, the chosen measure (cost per day) was adjusted for LOS to adjust for variability. Second, our analysis was focused on hospital costs. Future studies should explore costs from the perspective of patients and their families, in terms of informal care. Third, the degree to which the evidence presented is generalizable is unclear, because of the specificities of a quaternary hospital, which do not correspond to the reality at most cancer centers. Nevertheless, our study represents an important first step toward explaining the cost per day of PC at a quaternary teaching hospital in Brazil. It is also important to consider some methodological issues. Variables of interest with missing data, like KPS score information, could be better explored with predictive models. Future studies should also consider other type of models that might allow better understanding of various cost parameters. Because of the skewness and leptokurtosis, which are common to health care utilization data, it may be of interest to model other parameters. Therefore, a Generalized Additive Model for Location, Scale, and Shape (GAMLSS) could be an option.
Conclusion
Our data suggest that a KPS score <50, a higher number of hospital admissions, referral to PC from inpatient care, dying in a hospital, and dying in a hospice setting explained the higher cost per day of PC for patients with cancer at a quaternary teaching hospital in Brazil. To address health care costs, PC teams may consider focusing their efforts on integrating early end-of-life care with other specialties. In this regard, oncologists also have an important role in the delivery of primary PC (PC practiced by primary care clinicians, not specialized in palliative medicine), 33 and in facilitating timely referral of patients to PC teams, to enhance symptom management, communication, decision making, and end-of-life care.
To allocate resources effectively, cancer hospitals must tailor integration-based interventions according to their resources, size, and the level of primary PC available. PC facilities in LMICs must emphasize early inclusion of patients in PC outpatient services by means of: integrating PC early in the disease trajectory; avoiding hospital readmission while discussing goals of care with patients and families; and planning the place of death, regardless of the site of the cancer and the functional status of the patient, by motivating advance directive completion.
Footnotes
Funding Information
No funding was received.
Author Disclosure Statement
No competing interests exist.