
Abstract
Background and Objective:
With the increase of visits among patients with end-of-life needs, palliative care (PC) interventions delivered in the emergency department (ED) have become increasingly important. The objective of this systematic review was to examine the effectiveness of ED-based PC interventions.
Methods:
A comprehensive search of the literature was conducted to identify any comparative studies assessing the effectiveness of ED-based PC interventions. Two independent reviewers completed study selection, quality assessment, and data extraction. Relative risks (RR) with 95% confidence intervals (CIs) were calculated using a random effects model and heterogeneity (I2) was reported.
Results:
A total of 18 unique studies were included. Two studies reported no difference in return visits to the ED (RR = 1.31; 95% CI: 0.73–2.35; I2 = 47%). Two randomized trials reported no difference in mortality (RR = 0.89; 95% CI: 0.71–1.13; I2 = 0%), while one cohort study reported an increased mortality among patients referred to PC in the ED (RR = 1.89; 95% CI: 1.58–2.27). Overall, six out of eight studies reported a decrease in hospital length of stay (LOS) among patients undergoing an ED-based PC intervention compared with usual care.
Conclusions:
While there is compelling evidence to suggest that ED-based PC interventions can reduce hospital LOS, the evidence for the impact of these interventions on other outcomes is less robust. More high-quality comparative studies are needed to better understand the overall impact of ED-based PC interventions on improving patient outcomes as well as improving throughput and other quality of service-related outcomes.
Introduction
An increase in emergency department (ED) presentations among patients with end-of-life (EOL) conditions1,2 has prompted numerous investigations into the effectiveness of ED-based palliative care (PC) interventions.3,4 Indeed, early integration of PC services in the ED has been recommended by the Choosing Wisely Campaign in the United States to improve patient care. 5 Considering that some patients have reported the ED to be “distressing, exhausting, and disruptive,” 6 and would rather be cared for at home, 7 it is important for ED-based PC interventions to not only improve the quality of patient care, but also provide patients with access to palliative or hospice services in the community to provide alternatives to the ED.
While there is evidence for the need of PC services, there is a shortage of research describing how EDs can successfully integrate PC without straining resources and increasing costs. While preliminary studies have suggested possible benefits of earlier introduction of ED-based PC interventions,8,9 published systematic reviews have shown limited impact of ED-based PC interventions to improve outcomes.3,4 These reviews, however, have primarily relied on a purely descriptive summary of the results3,4 and new studies continue to be published.10,11 As such, the objective of this systematic review is to conduct an up-to-date and comprehensive search of the literature to identify and synthesize the available evidence through pooled or individual meta-analysis on the effectiveness of ED-based PC interventions.
Methods
Protocol
A study protocol was developed and registered on PROSPERO (registration no. CRD42018097375) to define the objective, selection criteria, data collection, and analysis. This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines for outcome reporting in systematic reviews. 12
Inclusion/exclusion
To be eligible, included studies had to be either randomized controlled trials (RCTs), before/after studies, or controlled observational studies. Studies were required to enroll adult patients (≥18 years) presenting to the ED with any advanced or EOL conditions. Included studies had to assess any type of PC intervention delivered in the ED. The studies had to utilize a control/comparison group consisting of standard/usual care as defined by the study authors. Additional information regarding the inclusion/exclusion criteria for the review are listed in Supplementary Appendix S1.
Outcome
The primary outcome was the proportion of patients who returned to the ED. Secondary outcomes of interest included mortality, disposition of the index visit, subsequent health care utilization (i.e., hospice use, intensive care unit [ICU] admission, hospitalization), length of stay (LOS) (i.e., ED LOS, hospital LOS, and time to PC consult), quality of life (QoL), proportion of patients receiving PC, and presence of symptoms.
Search methods for identification of studies
A search of the literature was designed and executed by an experienced health librarian (S.C.) on the following databases: OVID Medline, Ovid EMBASE, EBSCO CINAHL, SCOPUS, Proquest Dissertations and Theses Global, Cochrane Library, and PROSPERO using controlled vocabulary and key words representing the concepts “emergency department” and “palliative care”. Works specifically related to “palliative radiation” OR “palliative chemotherapy” were excluded. Searches were adjusted appropriately for different databases. Searches were conducted in October 2019. No limits based on language, year of publication, or publication status were applied. Foreign language articles were translated by a reviewer with native language skills or using Google Translate 13 if a reviewer with native language skills was not available. Detailed search strategies are available in Supplementary Appendix S2.
A search of the grey literature included Google Scholar, clinical trial registries (clinicaltrials.gov, Cochrane Central Register of controlled trials, and controlled-trials.com), backward and forward SCOPUS searches of included studies, bibliographies from known reviews, and hand searching of abstracts from emergency medicine conferences including Canadian Association of Emergency Medicine (2015–2019), Society of Academic Emergency Medicine (2015–2019), American College of Emergency Physician Abstracts (2015–2019), and the European Association for Palliative Care (2016, 2018).
Data collection and analysis
Selection of studies
Two reviewers (A.G., M.K.) independently screened the title and abstracts of citations from the search to identify potentially eligible studies. The full text of potentially relevant studies was retrieved and reviewed for eligibility by two independent reviewers (A.G., M.K.) using predefined inclusion/exclusion criteria. Disagreements were settled through third-party adjudication (S.W.K., C.V.R.).
Data extraction
Data were extracted onto standardized forms by two independent reviewers (A.G., H.R.) and discrepancies and disagreements were resolved using third-party adjudication (S.W.K.). The data were then extracted onto summary of finding tables. Authors were contacted to clarify any missing or unclear data identified during data extraction, when necessary.
Quality assessment
The methodological quality of cohort studies was assessed using a modified Newcastle–Ottawa Scale. 14 The quality of RCTs were assessed using the Cochrane risk of bias tool, 15 while the quality of before/after studies were assessed using the before/after quality assessment checklist. 16 Quality assessment was conducted by two independent reviewers (A.G., H.R.) and disagreements were resolved through third-party adjudication (S.W.K.).
Data synthesis
Studies were pooled if they represented similar populations, outcomes, study designs, and the research team judged that clinical heterogeneity was sufficiently low. Statistical analysis of the data was completed through Review Manager (RevMan, Version 5.4. The Cochrane Collaboration). For dichotomous variables, individual and pooled statistics were calculated as relative risks (RR) with 95% confidence intervals (CIs) using a random-effects model. A random effects model was used as it was assumed that the study effect sizes would not be identical due to the inherent differences among the studies with respect to patient population, implementation of the interventions, differences in ED management, and study methodology. For continuous outcomes, individual trial results were calculated as mean differences (MDs) with 95% CI using a random effects model. The weights given to each study in the pooled analysis was based on the Mantel–Haenszel method. When pooling was not possible, a descriptive analysis of the data was completed. Planned subgroup analysis of the primary outcome included study type (RCT vs. before/after vs. cohort), intervention type, and clinical conditions.
For the impact of PC interventions on LOS, a pooled meta-analysis was not possible as the majority of studies assessing LOS did not report any measures of variance for the intervention or control groups.10,17–20 Furthermore, the three studies that did report measures of variance each utilized a different study design, further limiting the ability to pool.8,9,11 Finally, the units of time used across the studies varied between minutes and days. As a result, the ratio of means (RoMs) with 95% CI was calculated for the LOS outcome variables as this method can be used regardless of the units used in individual trials and without a pooled standard deviation.21,22 In some cases, the 95% CI for the RoM of a particular study could not be calculated due to insufficient information provided by the study authors.10,18–20 The 95% CI was estimated in one study that did not report standard deviation but reported the p-value. 17 Due to methodological and clinical heterogeneity, pooling of the RoMs was not completed.
Heterogeneity was assessed using the I2 statistic with values of 25%, 50%, and 75% representing low, moderate, and high degrees of heterogeneity, respectively. 15 Publication bias of the primary outcome was proposed, as well as sensitivity analyses based on fixed effects and study quality, in which studies considered to be low quality were excluded from the analysis of the primary outcome.
Results
Search results
After the removal of duplicates, the title and abstracts of 5279 studies were reviewed for relevance. A total of 5164 studies were excluded for irrelevancy, and the full text of 115 studies was reviewed. A total of 95 studies were excluded, whereas 20 articles met all of the inclusion criteria and were included in the review (Fig. 1). Two of the included articles23,24 were found to be a supplemental report for one of the included trials. 9 Overall, the results from 18 unique trials were included.
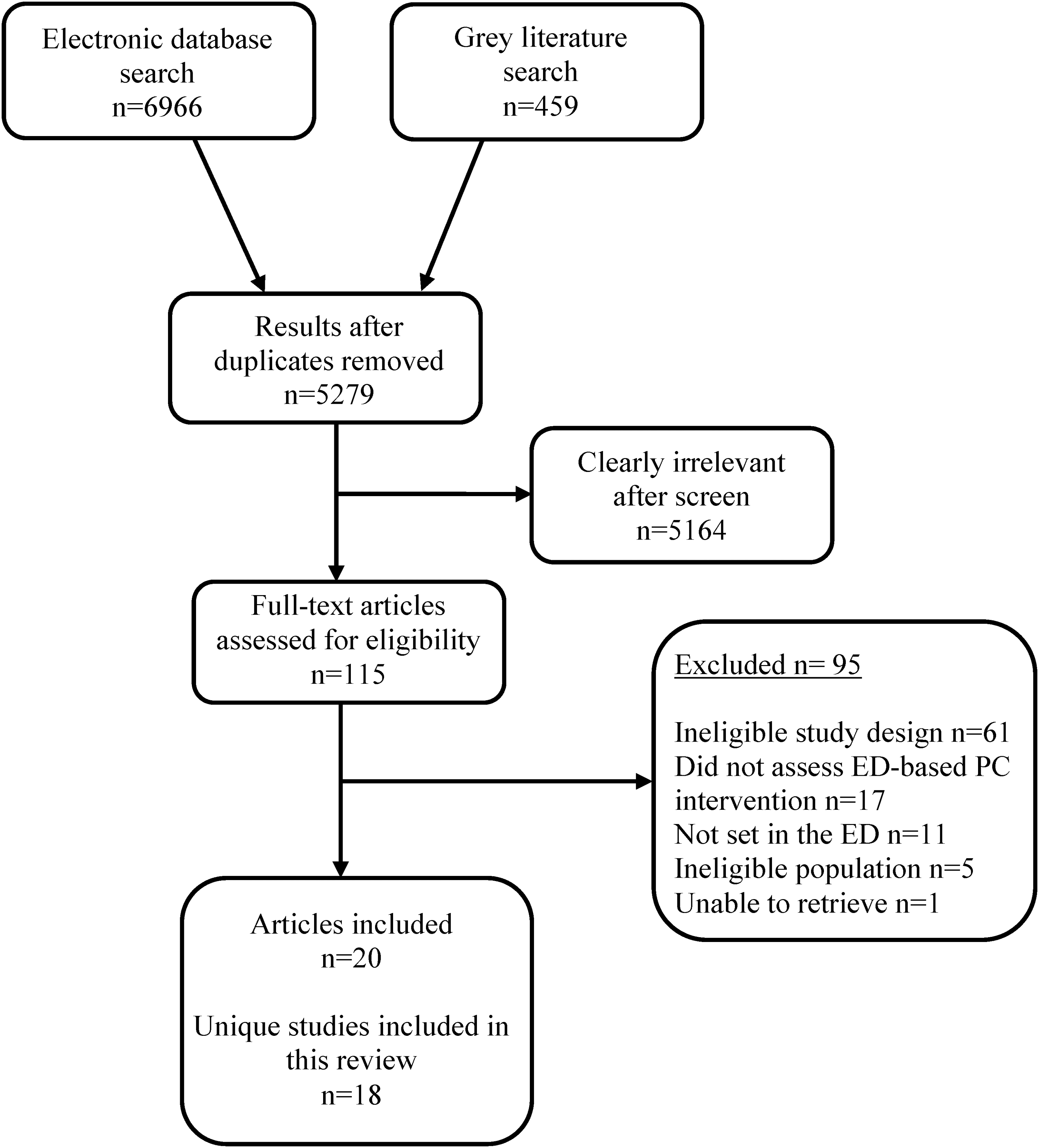
Literature search flow diagram.
Study characteristics
The included studies consisted of six unique RCTs,9,17,25–28 seven before/after studies,10,29–34 and five controlled observational cohorts8,11,18–20 (Table 1). Three of the included studies were protocols for ongoing clinical trials in which no outcome data were available for extraction.25,26,28 At least 4625 patients were enrolled across the studies; however, five of the included studies did not report the number of enrolled patients.19,30,31,33,34 The target patient population varied considerably across the studies (Table 1). Some studies specified that they enrolled patients with specific EOL conditions, including advanced cancer,9,11,29 advanced cancer/end-stage organ failure, 25 or advanced dementia/critical illness.18,30 Some studies allowed patients with any unspecified advanced illness to participate in the study, or reported to including any patients who underwent palliative services.8,10,19
Summary of the Study Characteristics of Systematic Review of Emergency Department-Based Palliative Care Interventions
COPD, chronic obstructive pulmonary disorder; ED, emergency department; EOL, end of life; GOC, goals of care; ICU, intensive care unit; PC, palliative care.
Interventions
See Table 1 for additional information on the PC interventions implemented in the included studies. While the exact nature of the interventions varied among the studies, the majority of studies (n = 14) assessed the impact of early requests for PC consultations in the ED.8,9,11,17–20,25–28,30,32,33 While several studies specified that the PC consult consisted of goals-of-care (GOC) discussions, spiritual/social needs assessments, and discussions regarding alternative care options,9,30,18 most authors did not specify what the PC consultation consisted of. The majority of studies reported that the control groups consisted of usual care, which was not typically defined; however, in some cases, studies specified that patients received a referral for a PC consult after the patient had been hospitalized.
Other PC interventions assessed included a PC education initiative targeting ED staff regarding PC and EOL conditions26,34 as well as providing workshops on communication in serious illness, and communication and feedback from a PC/hospice team (n = 2). Finally, two studies assessed the efficacy of ED-initiated referrals of patients to an inpatient PC unit 29 or ED-ICU. 31
Risk of bias assessment
The quality of the three published RCTs was assessed (Supplementary Appendix S3).9,17,27 The quality of the three published RCTs was considered unclear due to a lack of details as to how patients were randomized, blinded, and a lack of information regarding allocation concealment.17,27 One study was assessed as having a high risk of bias 9 due to a lack of blinding as well as a failure to report an outcome in the article that was listed in the protocol.
Overall, the quality of the before/after studies was mixed (Supplementary Appendix S4).10,29–34 For the majority of studies, the comparability of the pre and post groups was unclear, nor was an independent assessment of outcomes common. Data collection during pre- and postintervention periods were also not collected during similar time frames. Most studies reported that the pre- and post- groups came from the same source and utilized similar methods of outcome assessment.
Finally, the quality of the five cohort studies was also mixed with the quality of the studies ranging from high,8,19 moderate,11,20 and low 18 primarily due to a lack of reporting (Supplementary Appendix S5).
Primary outcome
A brief summary of the primary and secondary outcomes are reported in Table 2. Publication bias could not be assessed due to a lack of studies assessing the primary outcome.
Outcomes of Published Studies Assessing Palliative Care Interventions in the Emergency Department
Return to the ED
Only two included studies assessed the impact of the PC interventions on return visits to the ED.8,11 No differences in the proportion of patients with return ED visits was found (RR: 1.31; 95% CI: 0.73–2.35; I2 = 47%) (Fig. 2). A sensitivity analysis based on study quality reported identical outcomes, as no low-quality studies assessed return visits to the ED. A sensitivity analysis using fixed effects reported similar results (RR: 1.27; 95% CI: 0.83–1.94; I2 = 47%).

Impact of PC interventions on return to the ED. ED, emergency department; PC, palliative care.
Secondary outcomes
Mortality
Five studies assessed the impact of PC interventions in the ED on mortality.9,17,20,33,34 A pooled analysis of two RCTs failed to identify a difference in mortality (RR: 0.89; 95% CI: 0.71–1.13; I2 = 0%) (Fig. 3).9,17 One study reported no differences in median estimates of survival between intervention (289 days; 95% CI: 128–453) and control (132 days; 95% CI: 80–302) groups (p = 0.20). 9 One study reported lower in-hospital mortality among the control patients compared with patients receiving an ED-referral to PC (RR: 1.89; 95% CI: 1.58–2.27) (Fig. 3). 20 Two studies reported patient mortality for the intervention group; however, failed to report mortality for control patients.33,34
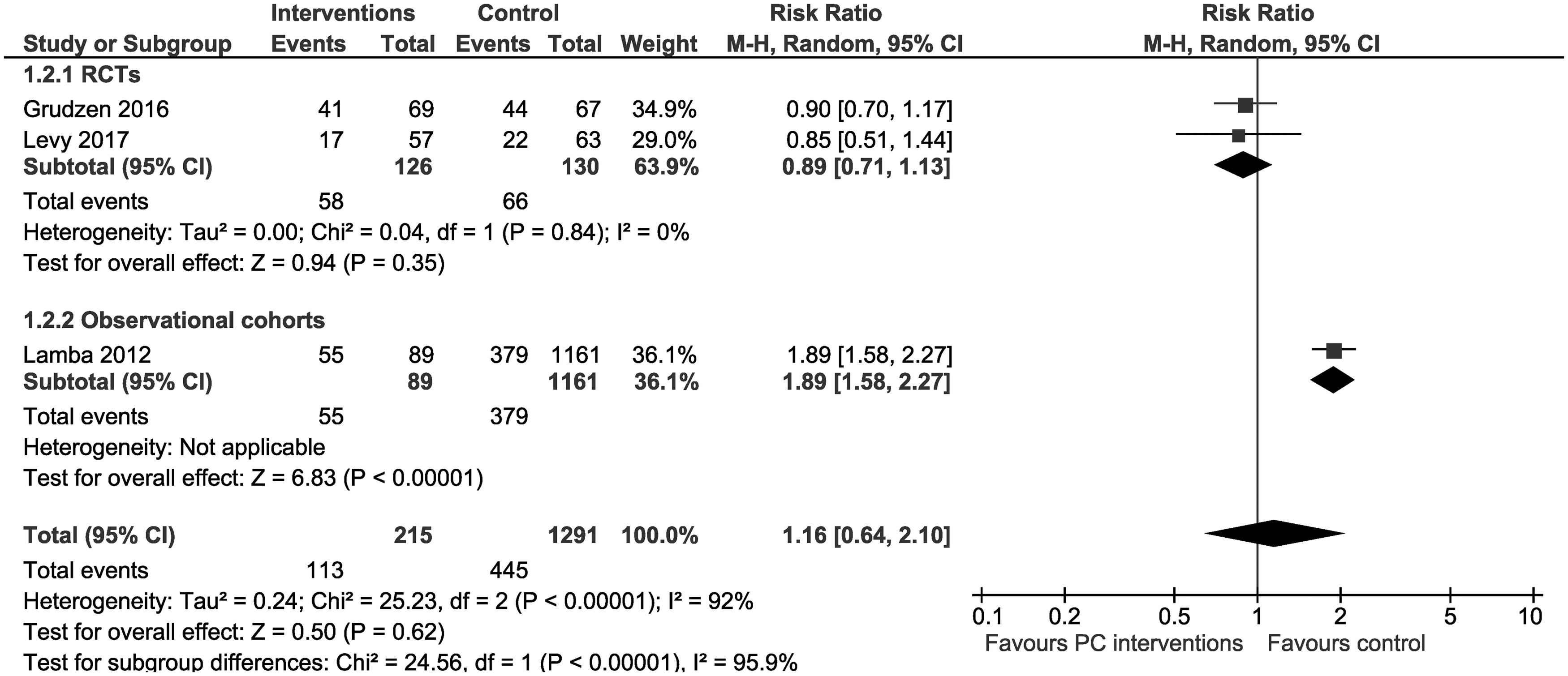
Impact of PC interventions on mortality.
Disposition
Ten studies assessed the impact of ED-based PC interventions on disposition (Table 2).8,9,11,19,20,30–33 A pooled analysis of two observational cohorts found that patients in the intervention group were more likely to be discharged home compared with control (RR: 0.67; 95% CI: 0.50–0.89; I2 = 0%). One before/after study reported an increase in patients discharged home following an ED-based PC consult compared with control patients (RR: 0.62; 95% CI: 0.42–0.92). 32 Of the five studies assessing discharge to hospice care, two reported an increase in the proportion of intervention patients discharged to hospice care compared with control.32,19
While significant heterogeneity in study design prohibited pooling among five studies assessing hospitalization, none of the studies identified a difference in hospitalization to an inpatient ward or ICU among intervention or control patients (Table 2).8,9,11,30,32
Subsequent health care utilization
One study reported no differences in subsequent hospice utilization (RR: 1.09; 95% CI: 0.62–1.90) or ICU admissions (RR: 1.17; 95% CI: 0.37–3.64) within 180 days between intervention and control patients. 9
Length of stay
Only one study assessed the impact of ED-based PC interventions on overall ED LOS. 11 Patients receiving a PC consultation in the ED experienced 46% longer ED LOS compared with control patients who did not undergo any consultations (MD: 148; 95% CI: 95.04–200.96 and RoM: 1.46; 95% CI: 1.26–1.69).
Eight studies assessed the impact of ED-based PC interventions on total hospital LOS,8–10,17–20,32 in which six studies reported a decrease in hospital LOS compared with control patients (Table 2 and Fig. 4).8,10,17–20 Overall, the most dramatic impacts were seen with ICU and hospice care patients. One study reported an increase in the median hospital LOS (two vs. zero days, p = 0.0003), 32 whereas another study reported no change in the patients' index hospital LOS (MD: 1.15; 95% CI: −0.82 to 3.12 and RoM: 1.20; 95% CI: 0.82–1.62).
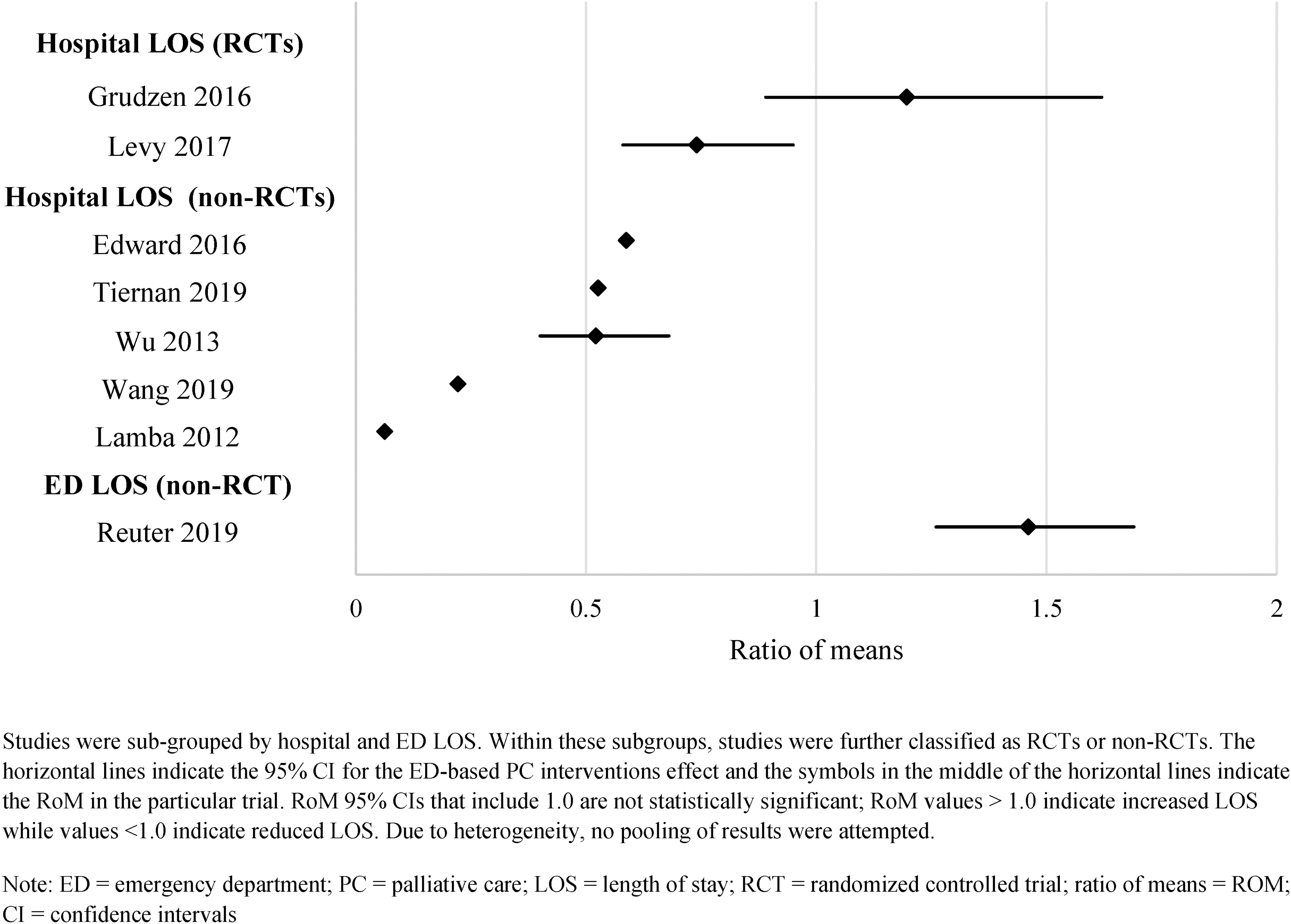
The impact of emergency-based PC consultations on total hospital and ED length of stay.
Among three studies assessing time to PC consultations, one study reported a significant decrease in time to PC consult among intervention patients (43 vs. 162 hours, p < 0.001), 17 whereas the remaining studies reported no differences between the groups.8,23
Quality of life
While one study reported a significant change in patient QoL scores among patients with early ED-initiated referral to PC compared with control patients, an individual meta-analysis identified no differences between the groups. 9
Patients undergoing PC consultations
Eight studies assessed the proportion of patients undergoing PC consultations,10,17,19,23,29,31,33,34 of which only three studies reported a significant increase in the proportion of patients receiving PC consultations in the ED among intervention patients compared with controls.10,19,23
Presence of symptoms
In two studies that assessed the proportion of patients with major depressive disorder 9 or depression/anxiety scores, 17 no differences between intervention and control groups were reported.
Discussion
Using an a priori protocol, this systematic review conducted an expansive search of the literature to identify 18 unique comparative studies of ED-based PC interventions. This review found moderate but consistent evidence that ED-based PC interventions reduce hospital LOS, however, due to infrequent and incomplete outcome reporting, the impact of these interventions on other outcomes remains unclear. For example, no firm conclusions could be drawn regarding important clinical outcomes, such as return ED visits, mortality/survivability, presence of symptoms, and/or patient QoL. While not necessarily an indicator of effectiveness of ED-based PC interventions, return to ED is an outcome that future studies should consider. Given that many patients have reported their preference to be treated at home,6,35 and evidence that patients receiving PC services in the last six months of life are less likely to have unplanned ED visits, 36 ED visits are worth further investigation as a measure of patient QoL.
It is perhaps not surprising that PC interventions would not have any meaningful impact on mortality, given that PC interventions are aimed at providing comfort care. In addition, it is unclear whether lower mortality would even be a goal of PC interventions, as many patients may prefer to be kept comfortable and pain free, rather than undergoing aggressive management to extend their life. As a result, the usefulness of using mortality as an indicator of the effectiveness of ED-based PC interventions is limited, and should probably be focused on other indicators of care.
Unfortunately, this review found that the impact of ED-based PC services on many of these other indicators of care to be infrequently assessed and are often reported incompletely. Many studies failed to report outcomes for control groups and did not report standard measures of variance for continuous outcomes. The lack of consistent and complete outcome reporting has limited the ability of the current and previous systematic reviews3,4 to conduct meaningful meta-analysis of the effectiveness of ED-based PC interventions. It is imperative that high-quality comparative studies with robust and complete outcome reporting are completed to better understand how ED-based PC interventions can be delivered to best improve outcomes for patients.
Perhaps not surprisingly, the lone study to report on ED LOS found that PC consultations conducted in the ED increased LOS, which could be due to consultation delays and additional interviews. Conversely, six of eight studies reported a significant and large decrease in hospital LOS associated with ED PC interventions. The reduction in hospital LOS is likely due to the time-sensitive nature of PC consults, and that obtaining the consultation early while the patient is still in the ED likely results in earlier decisions on GOC, expedited PC referrals, and more appropriate management. It is important, however, for additional research to further assess the impact of ED-based PC interventions on ED and hospital LOS. In particular, if ED-based PC interventions do increase ED LOS, it is important to explore the benefits/risks posed to patients with EOL conditions before any ED-based interventions are implemented. Methodological heterogeneity and infrequent/incomplete outcome reporting for LOS outcomes also limited the ability of this review to conduct meaningful meta-analysis and more studies are recommended to provide evidence clarity.
While the overall findings of this review are similar to other systematic reviews assessing ED-based PC interventions,3,4 there are some important differences. First, the current review identified more unique published comparative studies (n = 15) than either of the previous reviews,3,4 which is likely the result of an up-to-date and expanded literature search. Second, the other systematic reviews strictly conducted a descriptive summary of the results, whereas the current review attempted individual or pooled meta-analysis when sufficient data were possible to provide a quantitative estimate of the impact of ED-based PC interventions on important outcomes.
In addition, this review conducted a RoM analysis of the studies reporting hospital and ED LoS in an effort to address the incomplete outcome reporting among many of the included studies, which in turn allows this review to provide a more detailed summary of the impact of ED-based PC interventions on LoS. Overall, we believe this review provides the most relevant, up-to-date and robust assessment of the impact of ED-based PC interventions on important patient outcomes.
As discussed perviously,3,4 the current review highlighted several concerns regarding the available studies assessing ED-based PC interventions that have contributed to the inability to provide robust conclusions regarding the effectiveness of these interventions. In addition, these concerns have delayed the ability for health care providers to better design and implement PC interventions to improve the quality of care of patients with EOL needs. The majority of the available data comes from nonrandomized studies that can be prone to bias and overestimation of treatment effects. Even among the published RCT's identified in this review,9,17,27 two of the studies were only published as abstracts with no further publications.17,27
In addition, inconsistent reporting of important clinical outcomes, as well as incomplete reporting of measures of variance, failure to report the number of included patients, and failure to report treatment effects for intervention and control groups were frequent issues that limited the ability of this review to effectively summarize the impact of ED-based PC interventions for important clinical outcomes.
Finally, studies frequently did not report the implementation strategies of ED-based PC interventions, making it difficult to duplicate studies or replicate interventions into practice. Given all these concerns, we recommend that an Utstein-style consensus be established through experts in emergency and palliative medicine for the standardized conduct and reporting of studies assessing ED-based PC interventions. For future studies, researchers need to prioritize conducting high-quality randomized controlled studies, with complete reporting of important clinical outcomes along with full details regarding how their ED-based PC interventions were implemented. Otherwise, these issues identified in the current and previous reviews3,4 on ED-based PC interventions will continue, as will the inability of health care providers to advocate for ED-based PC interventions for those patients most in need.
Limitations
There are several limitations with this review that must be considered. Differences among the interventions and their implementation may have impacted the results of this review. Given that the majority of studies assessed PC consultations in the ED, the impact of the other interventions assessed in this review, including PC education-based interventions and referrals to PC programs/care units are largely unknown due to inconsistency of outcome reporting. Second, details regarding treatment fidelity (e.g., how the interventions were implemented) were frequently missing and so it is unclear if these interventions were implemented in the manner that was intended. It is vital for future studies to report the implementation strategies of their interventions to ensure replicability of the study, as well as to ensure that the intervention was implemented sufficiently.
Third, it is also possible that differences in the patient population, including clinical acuity, availability of social support, and clinical conditions may have impacted the results, as patients with less clinical acuity and more social support might be more likely to benefit from PC interventions compared with patients with severe symptoms and no available support structure. Fourth, the majority of the data reported in this review comes from studies employing a nonrandomized study design, so it is possible that the biases inherent in nonrandomized studies could have impacted the results of this review. Fifth, as with any systematic review, there is a risk of selection and publication bias; however, steps were taken to minimize these risks, including conducting an extensive search of the published and unpublished literature with no limitations and dual independent study selection with adjudication.
Finally, these interventions have a cost associated with them; the lack of health economic data precluded any assessment of the cost-effectiveness of a strategy employing ED-based PC referrals. One of the included studies reported evidence that consults with a Geriatric Emergency Medicine Service team reduced the use of aggressive and costly interventions. 18 Additional research on the costs-effectiveness of palliative interventions is needed.
Conclusion
This review found moderate but inconsistent evidence for ED-based PC interventions to reduce hospital LOS; however, additional research is needed to provide clarity as to the impact of these interventions on important health indicators, including QoL, subsequent ED/health care utilization, and symptom management. It is vital that future studies employ stronger methodology, detailed descriptions of implementation strategies, and robust outcome reporting to better understand how interventions to promote PC services in the ED can be implemented to provide the best quality of care for patients with EOL needs.
Footnotes
Authors' Contributions
S.W.K. contributed to the conception and design of the review, study screening, acquisition of data, data analysis and interpretation, and article preparation. C.V.R. contributed to the design of the review, study screening, acquisition of data, and article preparation. She has no conflicts of interest to declare. A.G., M.K., and H.R. contributed to study screening, acquisition of data, and article preparation. She has no conflicts of interest to declare. S.C. contributed to the development of the electronic search and article preparation. E.H.Y. contributed to acquisition of data, data analysis and interpretation, and article preparation. She has no conflicts of interest to declare. B.H.R. is the guarantor of the review. He secured funding and contributed to the conception and design of the review, study adjudication, data analysis of interpretation, and article preparation.
Acknowledgment
The authors would like to thank Dr. Harvey for responding to their requests for additional information regarding their article.
Funding Information
Funding for this review was provided by the Ministry of Alberta Health, Government of Alberta. Dr. Rowe's research is supported by the Canadian Institutes of Health Research (CIHR) by a Scientific Director's Grant (SOP 168483) through the Government of Canada (Ottawa, ON). These funding organizations had no involvement in any aspect of the conduct, analysis, and article preparation of this study; the funders take no responsibility for the conduct or results of this review.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.