
Abstract
Background:
Little is known about end-of-life care experiences of Asian Americans and gaps in end-of-life care quality between Asians and non-Hispanic whites.
Objective:
Compare the perceptions of next-of-kin of Asian and non-Hispanic white decedents on end-of-life care quality.
Design:
Mortality follow-back survey.
Setting/Subjects:
Population-based sample of 108 Asian and 414 non-Hispanic white bereaved family members or close friends of adult, nontraumatic deaths in the San Francisco Bay area in 2018.
Measurements:
Survey items examined whether health care professionals treated the dying person with respect and dignity, respected their cultural traditions, respected their religious or spiritual beliefs, provided enough information about what to expect during the last month of life, provided emotional support to the family after the patient's death, and whether the dying person and the family received the needed help after work hours.
Results:
Of the 623 surveys (weighted n = 6513), 108 (weighted percentage = 17.6%) were from caregivers of Asian decedents. Almost half of these respondents indicated that they did not always experience respect for their cultural traditions (45.9% vs. 21.8%, p = 0.00) or respect for their religious and spiritual beliefs (42.2% vs. 24.5%, p = 0.01). With the exception of two outcomes, worse caregiver-reported care quality for Asian decedents persisted after adjustment for cause of death, site of death, type of health insurance, respondent's relationship to decedent, decedent age, and respondent education.
Conclusions:
Compared with caregivers of non-Hispanic whites, caregivers of Asian decedents reported unmet needs for caregiver support and lack of respect for cultural traditions and religious/spiritual beliefs.
Introduction
Asian Americans (hereafter referred to as “Asians”) are the fastest growing ethnic group in the United States, projected to surpass Hispanics and become the largest immigrant group by 2055. 1 Despite the rapid population growth of Asians, little is known about their end-of-life care experiences. Prior literature on racial disparities in end-of-life care has focused on health care use, care preferences, and care planning. Studies suggest that, compared with non-Hispanic whites, minority patients are more likely to die in hospitals, have longer hospital stays, more ICU stays, and are less likely to use hospice services.2–4 They are also less likely to engage in advance care planning and have their care preferences documented.5–7
Similarly, Asians tend to be less knowledgeable about hospice care 8 and advance care directives,9,10 and have lower rates of hospice use and completion of advance directives than non-Hispanic whites.11–13 Studies have also documented that Asians in the United States and Canada tend to receive more aggressive care in their last months of life.14–16 Overall, Asians have received less attention than African Americans and Latinos in research focused on racial disparities in end-of-life care experiences.
Patient and family experiences of care are an essential domain of health care quality, as they reflect the person-centeredness of care. 17 A mortality follow-back survey contacts the next-of-kin listed on a death certificate to examine bereaved family member's perceptions of the quality of care in the last weeks of life. Dying persons are often unable to be interviewed, and hence, measuring experiences of bereaved family members or close friends is important when assessing end-of-life care quality. Prior research has characterized the dying experience of blacks compared with whites using a mortality follow-back approach, 18 but no study to date has characterized end-of-life care experiences of Asians compared with non-Hispanic whites from the perspective of bereaved family members.
To address this gap, we examined end-of-life care experiences reported by bereaved family members or close friends of Asian and white decedents. We conducted a mortality follow-back survey in the San Francisco Bay area, which has a large Asian population comprising 35.9% of all persons in San Francisco County and 31.8% in Alameda County. 19 By focusing on the survey items that assess (1) health care professionals' respect for cultural traditions and religious beliefs and (2) caregiver support in the last month of the decedent's life, our research identifies areas in which Asian patients and their families in the San Francisco Bay area report concerns and opportunities for improvement in Asians' end-of-life care experiences.
Methods
Design and participants
A cross-sectional, retrospective study using a mortality follow-back survey was conducted in 2019 and 2020. Death certificates identified the next-of-kin or informant of eligible adults who died from nontraumatic deaths resulting from chronic progressive illnesses in 2018 in nine counties surrounding San Francisco. Persons who died from trauma, suicide, complications of pregnancy, and those younger than 18 years were excluded. Decedents received end-of-life care in a variety of settings, including hospitals, nursing homes, and home-based medical services, such as hospice and home health care.
Surveys were mailed to the informants identified on the death certificate. First, a self-administered survey was sent by mail. If no response was received after several weeks, potential respondents whose phone numbers were available were contacted via telephone. If a phone number was not available, a second self-administered survey was sent by mail. Telephone follow-up was not conducted in the second round of survey due to the limited yield of telephone administration in the first round.
To enhance response from those who might prefer to complete the survey in either Spanish or Chinese instead of English, surveys were mailed in both English and Spanish or English and Chinese, respectively, for sampled informants who (1) resided in a zip code with greater than 10% Spanish or Chinese speakers and (2) whose decedents' death certificate indicated that they were of Hispanic or Chinese ethnicity.
The survey was administered about 9 months after the patient's death, ranging from 139 to 459 days after death with a median of 291 days. A total of 623 persons participated in the survey, resulting in a response rate of 21.0%. Sampled next-of-kin of non-Hispanic white decedents were more likely to respond than next-of-kin of nonwhite decedents (38.1% vs. 27.2%, p < 0.001). Response rates were lowest among next-of-kin of decedents who died in hospitals, and highest in a nursing home or long-term care facility (17.4% vs. 25.8%, p < 0.05). The study was approved by both the RAND Corporation's and the State of California's Institutional Review Boards (IRBs).
Measures
Quality of end-of-life care in the last month
Based on Teno et al.'s conceptual model of patient- and family-centered medical care20,21 and the CAHPS Hospice Survey, 22 the mortality follow-back survey was designed to address the following domains of end-of-life care: staff and physician communication; symptom and pain management; goal-concordant care; respect for culture, spiritual, and religious beliefs; and caregiver support (Supplementary Data). Survey questions were grouped into either questions specific to places of care or specific services (i.e., hospice), or global questions about the overall care experience in the last month of life irrespective of place of care. This study analyzed the global questions about care quality in the last month, as there were limited sample sizes to compare responses by race across sites of care.
The selected survey items asked whether health professionals (1) treated the patient with dignity and respect, (2) respected the patient's cultural traditions, (3) respected the patient's religious or spiritual beliefs and practices, (4) provided needed help during evenings, weekends, or holidays, (5) provided as much information as the respondent needed about what to expect during the last month of life, and (6) provided emotional support to the respondent in the weeks after their loved one's death (Supplementary Table S1). Response scales for questions (1)–(4) were “never, sometimes, usually, or always.” For question (5), response options were “no; yes, somewhat; yes, definitely”; and for question (6), “too little; right amount; too much.” Health professionals or staff were defined to include all the doctors, nurses, social workers, chaplains, aides, and other staff who provided care at varying settings of care such as at home, in an assisted living facility, in a hospice, a hospital, or a nursing home.
Our outcomes of interest were “reported quality concerns.” Responses except for the most favorable response (i.e., always; yes, definitely; right amount) were given a value of 1 and identified as an opportunity to improve.
Decedent and respondent characteristics
The variable of primary interest in our analysis was the patient's race and ethnicity, which was identified by survey responses from their next-of-kin. Variables characterizing the study sample included the decedent's age, type of health insurance, cause of death, site of death, hospice use ≥2 days, the main language spoken at home, the respondent's relationship to the decedent, respondent age, and respondent education. Information about cause of death and site of death was collected from death certificates, while other variables were collected from survey responses.
Analytic approach
A sample description of Asian and non-Hispanic white patients and their next-of-kin respondents is presented using percentage and 95% confidence intervals (CIs). The 95% CIs for descriptive data were calculated using Stata's-proportion-command and the Wilson score method. Using six binary outcome measures, chi-squared tests examined bivariate associations between reported quality concerns in the last month and race. We performed multivariate logistic regression models for each of the six binary outcomes (i.e., reported quality concern vs. most positive care experience), adjusted for cause of death, site of death, type of insurance, respondent education, decedent age, and respondent's relationship to decedent, to further confirm the association of Asian race with reported end-of-life care experiences. We performed a sensitivity analysis between the subpopulations of Asians and non-Hispanic whites who mainly spoke English at home to remove any language differences and determine whether the differences in reported care experiences by race persisted. Survey weights were used to account for the complex sample design and to make the findings representative of the populations in the San Francisco area. Quantitative data analyses were conducted using Stata version 16 software (StataCorp, College Station, TX).
Results
Sample description
Table 1 shows decedent and respondent characteristics. Of the 623 interviews (weighted n = 6513), 108 (weighted percentage = 17.6%) were Asian and 414 (weighted percentage = 60.7%) were non-Hispanic white. Compared with non-Hispanic white decedents, a lower proportion of Asian decedents were Medicare beneficiaries or Medicare beneficiaries with private insurance coverage (35.2% vs. 76.3%) and those who used hospice services for at least two days (47.4% vs. 63.2%). A higher proportion of Asian decedents were covered by Medicaid (22.2% vs. 5.4%) or were dual-eligible (17.4% vs. 5.1%) and died in a hospital (44.1% vs. 21.8%). Roughly half of Asian respondents (46.4%) did not primarily speak English at home, while the great majority of white respondents (96.0%) primarily spoke English at home.
Decedent and Respondent Characteristics by Race
Medicare group includes Medicare beneficiaries with or without supplemental/private insurances. For those with Medicare only, the comparison was 17.9% versus 33.8%.
Other diseases include chronic kidney or liver disease, primary hypertension, type 2 diabetes, hyperlipidemia, and other diseases that were too low in frequency to report based on the data use agreement to use death certificate data.
Missing values for English spoken at home account for 14.2% for Asians and 2.9% for whites.
Missing values for education account for 6.7% for Asians and 2.2% for whites.
Quality of end-of-life care in the last month
Figure 1 presents bivariate comparisons of reported quality concerns between Asian and white decedents. Overall, compared with non-Hispanic white decedents, next-of-kin of Asian decedents reported more concerns with the quality of care. Next-of-kin of Asian decedents more often reported that the staff providing care did not always treat the patient with dignity and respect compared with next-of-kin of non-Hispanic white decedents (37.1% vs. 22.6%, p = 0.03). Almost half of next-of-kin of Asian decedents reported that the decedent's health care providers did not always respect their cultural traditions compared with less than a quarter of next-of-kin of white decedents (45.9% vs. 21.8%, p = 0.00). Over 4 in 10 next-of-kin of Asian decedents reported that health care providers did not always respect their religious and spiritual beliefs and practices compared with fewer than 1 in 4 next-of-kin of non-Hispanic white decedents (42.2% vs. 24.5%, p = 0.01). Almost three-quarters of next-of-kin of Asian decedents reported unmet needs for receiving help during after-hours compared with less than half of next-of-kin of non-Hispanic white decedents (70.3% vs. 46.1%, p = 0.02).
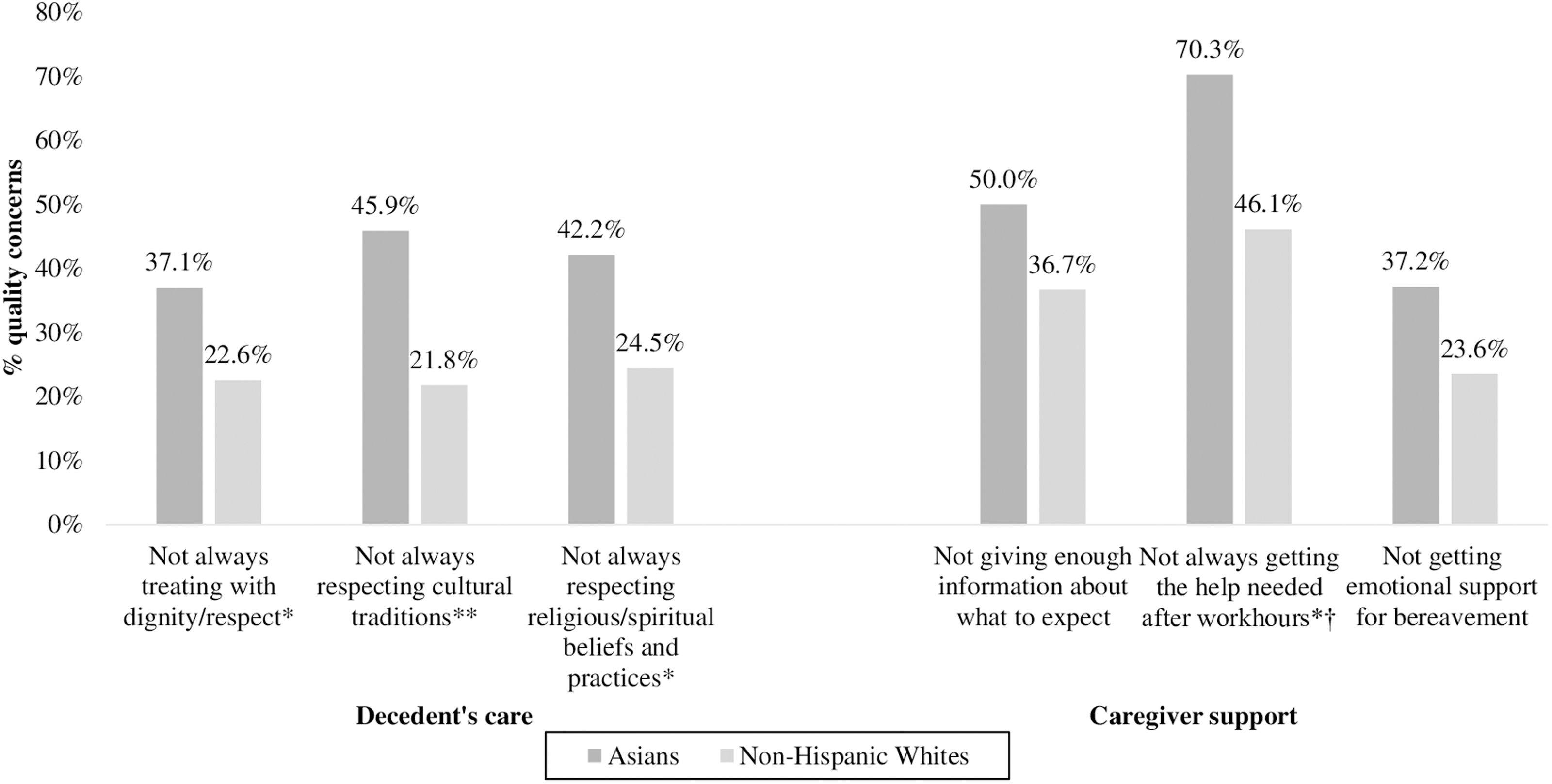
Proportion of respondents expressing quality concerns by the decedent's race. *p < 0.05, **p < 0.01. p-value is obtained from chi-squared tests. Total number of respondents for each item is as follows: Staff not always treating with dignity/respect (n = 499, weighted n = 4863); staff not always respecting cultural traditions (n = 481, weighted n = 4735); staff not always respecting religious/spiritual beliefs and practices (n = 478, weighted n = 4735); staff not always giving information about what to expect in the last month of life (n = 494; weighted n = 4711); respondents not always getting the help needed after work hours (n = 265; weighted n = 2413); respondents not getting the right amount of emotional support after their loved one's death (n = 477; weighted n = 4600). †The denominator represents persons who needed help after hours. Of the 498 valid responses (weighted n = 4765), a weighted percentage of 57.1% of Asians and 50.4% of whites reported that they needed help during evenings, weekends, and/or holidays.
The association between Asian race of decedents and poor experiences of end-of-life care compared with non-Hispanic whites persisted after adjusting for cause of death, site of death, type of health insurance, respondent's relationship to decedent, decedent age, and respondent education (Table 2). Asian decedents were more likely to experience lack of respect from staff for their cultural traditions (adjusted odds ratio, AOR = 3.59, CI = 1.88–6.86), and for their religious or spiritual beliefs (AOR = 2.85, CI = 1.45–5.62). There were also significant quality gaps between next-of-kin of Asian and non-Hispanic decedents on receiving as much information as they wanted about what to expect during the last month of the decedent's life (AOR = 2.15, CI = 1.10–4.19) and receiving the right amount of emotional support after the decedent's passing (AOR = 2.39, CI = 1.23–4.63). Differences in the likelihood of reporting that the decedent was treated with dignity and respect and got needed help after hours were not statistically significant after adjustment.
Multivariable Logistic Regressions on Next-of-Kin Perspectives of Quality of Care in the Last Month of Life
A multivariate model adjusted for cause of death, site of death, type of insurance, respondent education, decedent age, and respondent's relationship to decedent.
CI, confidence interval.
Our sensitivity analysis found similar patterns among respondents who speak mainly English at home; however, differences between reported care experiences for Asian decedents and non-Hispanic white decedents were statistically significant for only two of the outcomes of interest (respect for cultural traditions and religious and spiritual practices), likely due to the smaller sample available for this analysis (Supplementary Figure S1 and Supplementary Table S2).
Discussion
Despite the rapid growth of the population of Asians in the United States, few studies exist on end-of-life care experiences of Asian Americans. Using a mortality follow-back survey approach, our study demonstrates significant quality gaps in end-of-life care between Asians and non-Hispanic whites in the San Francisco Bay area. About half of next-of-kin of Asian decedents reported more concerns with health care providers' respect for the patient's cultural traditions and religious beliefs and practices. Next-of-kin of Asians were also more likely than next-of-kin of non-Hispanic whites to report unmet needs for caregiver support, measured as receiving enough information about the patient's last month and bereavement support.
Cultural traditions and religious beliefs shape care preferences and affect interactions with health care providers. 23 Our finding suggests that the medical staff may not have carefully addressed patient wishes and preferences influenced by cultural traditions or spiritual beliefs, and thus, patient preferences are not likely to be reflected in the care they receive. Prior evidence suggests that effective approaches for patient engagement in decision making for end-of-life care vary across cultures. For instance, Asian Americans are often reluctant to directly discuss topics related to death, 24 and tend to be more comfortable with collective decision making involving families and physicians than a decision-making model heavily relying on patient autonomy.9,13 Asian Americans are also open to discuss and receive more information about future treatments such as hospice services, as long as information is delivered in culturally sensitive ways by content experts. 8
According to a recent qualitative study of multiethnic patients in California, patients identified a lack of cultural awareness from their providers as a major barrier to meaningful end-of-life care discussions and quality end-of-life care. 25 Health care providers will need to develop careful approaches to communicate patients' cultural and spiritual needs in health care delivery. Future qualitative studies may add to the present analysis and inform health care providers by investigating care experiences for patients and families with different religious or spiritual beliefs and cultural traditions.
We also found a significant quality gap between next-of-kin of Asian and white decedents in receiving information on what to expect during the last month of the decedent's life and receiving desired levels of emotional support in the weeks after their family member's death. Previous studies have identified similar patterns for other racial and ethnic minority groups. A prior national study reported that family members of African American decedents expressed more concerns over not being adequately informed on what to expect during the dying process and more unmet needs for bereavement support than those of white decedents. 18 Similarly, in medical care not specific to end-of-life care, studies have shown that clinicians' implicit racial and ethnic biases negatively affected how much information a physician provided to black and Hispanic patients compared with non-Hispanic white patients 26 and led to poor interpersonal communication and distrust in primary care. 27 Our study extends existing literature by showing that the disparities experienced by blacks and Latinos are also consistently observed in Asian populations, and that unequal provisions of information and inadequate caregiver support based on the patient's racial background persist in end-of-life care.
It is notable that racial gaps in end-of-life care experiences persisted when we controlled for the decedent's type of insurance and the respondent's education, and when we restricted our analytic sample to those who primarily spoke English at home. This suggests that racial disparities in quality of end-of-life care are not solely explained by the patient's social assets and conditions (e.g., financial and health insurance barriers, limited education, or language barriers), but also by health care providers' failure to respond to the needs, culture, and preferences of Asian patients and their families. 17
Important limitations need to be acknowledged. First, our mortality follow-back survey focused on the San Francisco Bay area, with a response rate of 21.0%. Therefore, our findings may not generalize to other locations in the United States; however, our findings suggest the importance of studying end-of-life care experiences for Asian Americans in other geographic areas. Second, this is a retrospective study that relies on the memories of the family or close friends of the decedent. Recall bias can pose a threat to the internal validity of this study. However, previous evidence has shown that proxy respondents tended to accurately report their experiences on diverse quality of care domains,28,29 and we do not have reason to believe that this bias would be greater among next-of-kin of Asian decedents than among next-of-kin of white decedents. Last, there is evidence that Asians tend to report lower satisfaction with medical care than other racial and ethnic groups, and that the lower satisfaction is, in part, explained by their different use of response scales. For instance, Asians less frequently select the most extreme response option (e.g., the most positive experience) than whites,30,31 which may explain their reporting worse care than other groups. In our analysis, next-of-kin of Asian decedents were more likely than next-of-kin of non-Hispanic white decedents to select response options such as “usually” or “yes, somewhat,” and less likely than next-of-kin of non-Hispanic whites to select options such as “always” or “yes, definitely” (see Items 1–5 in Supplementary Table S1). The quality gaps found in our study cannot be entirely explained by systematic differences in Asian's response patterns; nonetheless, the magnitude of the differences we report should be interpreted bearing in mind these differences in response patterns.
Despite these limitations, this article highlights notable racial differences in quality of end-of-life care among Asian decedents and their family members in the San Francisco Bay area. The findings of our study suggest organization- or health systems-level investments to develop interventions to deliver high-quality and culturally sensitive end-of-life care for diverse populations. 32 Our finding also adds to the end-of-life care quality literature by focusing on Asian Americans, who have been given less focus in prior literature than other minority patients, including African Americans and Hispanics. As the population of Asians in the United States and the emphasis on shared decision making increase, 33 efforts to develop cultural sensitivity in care delivery and to ensure equal provision of information and emotional support across all racial/ethnic backgrounds will be crucial in providing goal-concordant and patient- and family-centered end-of-life care.
Conclusion
Significant disparities in the quality of care exist for Asian Americans in the San Francisco Bay area. Compared with next-of-kin of white decedents, next-of-kin of Asian decedents were more likely to report lack of respect for religious/spiritual beliefs and unmet needs for caregiver support, including insufficient provision of information and bereavement support. Efforts are needed to promote high-quality, patient- and family-centered care at the end of life for Asian Americans.
Footnotes
Acknowledgments
The authors appreciate the time and efforts invested by the survey respondents and staff at the RAND Corporation.
Funding Information
Data for this study were originally assembled for research funded by the Stupski Foundation.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.