
Abstract
Background:
Patients receiving dialysis have unmet palliative care needs. Limited access to palliative care is a key barrier to its integration into routine dialysis care.
Objective:
To determine the feasibility and acceptability of telepalliative care in rural dialysis units.
Methods:
This was a single-arm pilot clinical trial. The target population was patients with kidney failure receiving outpatient dialysis in a rural U.S. state. Feasibility was measured by one-month completion rate. Acceptability was measured using an adapted telemedicine questionnaire.
Results:
We recruited 39 patients with mean age 71.2 years to undergo a telepalliative care consultation while receiving dialysis. Four specialty palliative care clinicians (three physicians and one nurse practitioner) conducted the visits. The recruitment rate was 40% (39/96), scheduling rate was 100% (39/39), and one-month completion rate was 77% (30/39). Thirty-six patient participants (14 women and 22 men) completed the baseline survey. Audiovisual aspects of the visit were rated highly. More than 80% reported the visit being at least as good as an in-person visit and 41% felt the teleconsult was better. Eighty-one percent of patients felt the appointment was relevant to them, 58% felt they learned new things about their condition, and 27% reported the appointment changed the way they think about dialysis.
Discussion:
Telepalliative care is acceptable to patients receiving dialysis and is a feasible approach to integrating palliative care in rural dialysis units.
The study was registered with Clinicaltrials.gov (NCT03744117).
Introduction
Patients with kidney failure experience many burdensome symptoms, undergo frequent hospitalizations and interventions, and have shortened life expectancy.1–4 Yet, prognostic awareness is low and advance care planning is underutilized in patients receiving dialysis. 5
There is a growing body of literature demonstrating the potential benefits of palliative care in dialysis patients. 6 Palliative care includes care for patients with serious illness, such as kidney failure, and may include attention on symptom management as well as advance care planning. Palliative care improves quality of life without shortening survival. 7 However, several barriers exist for patients receiving dialysis access palliative care, including lack of availability of specialist palliative care, low referral rates to palliative care, and travel time and costs associated with additional clinic visits, particularly for patients on thrice weekly in-center dialysis treatments.
Specialist palliative care services are more likely to be found in academic medical centers than in small rural hospitals. There are few reports of telepalliative care and no published accounts of using telemedicine for palliative care in dialysis units. We sought to determine the patient- and clinician-rated acceptability and feasibility of using telemedicine to deliver palliative care for patients receiving maintenance hemodialysis.
Methods
Design
The Institutional Review Board at The University of Vermont approved this study and procedures adhered to the Declaration of Helsinki. This was a single-arm clinical trial conducted in a rural U.S. state.
Population and clinical setting
The target patient population was adult patients receiving maintenance dialysis for kidney failure at one of the University of Vermont Medical Center (UVMMC) dialysis units. The overall UVMMC dialysis population is predominantly white, but is similar to national data in other respects, mean (standard deviation) age was 65 ± 14 years and 41% female, and patients report similar Kidney Disease Quality of Life survey results. 8 UVMMC dialysis units are nonprofit clinics staffed by medical center employees (nephrologists, nurses, and technicians) and located in five towns across the state, 3–89 miles (5–143 km) from the UVMMC and serving rural patients. We excluded people receiving dialysis for acute kidney injury, non-English speaking, unstable psychiatric illness, or unable to provide consent. We also excluded people who received dialysis during times that clinicians were not available (n = 155), that is, outside of usually outpatient clinic hours (8 am–5 pm) (Fig. 1).
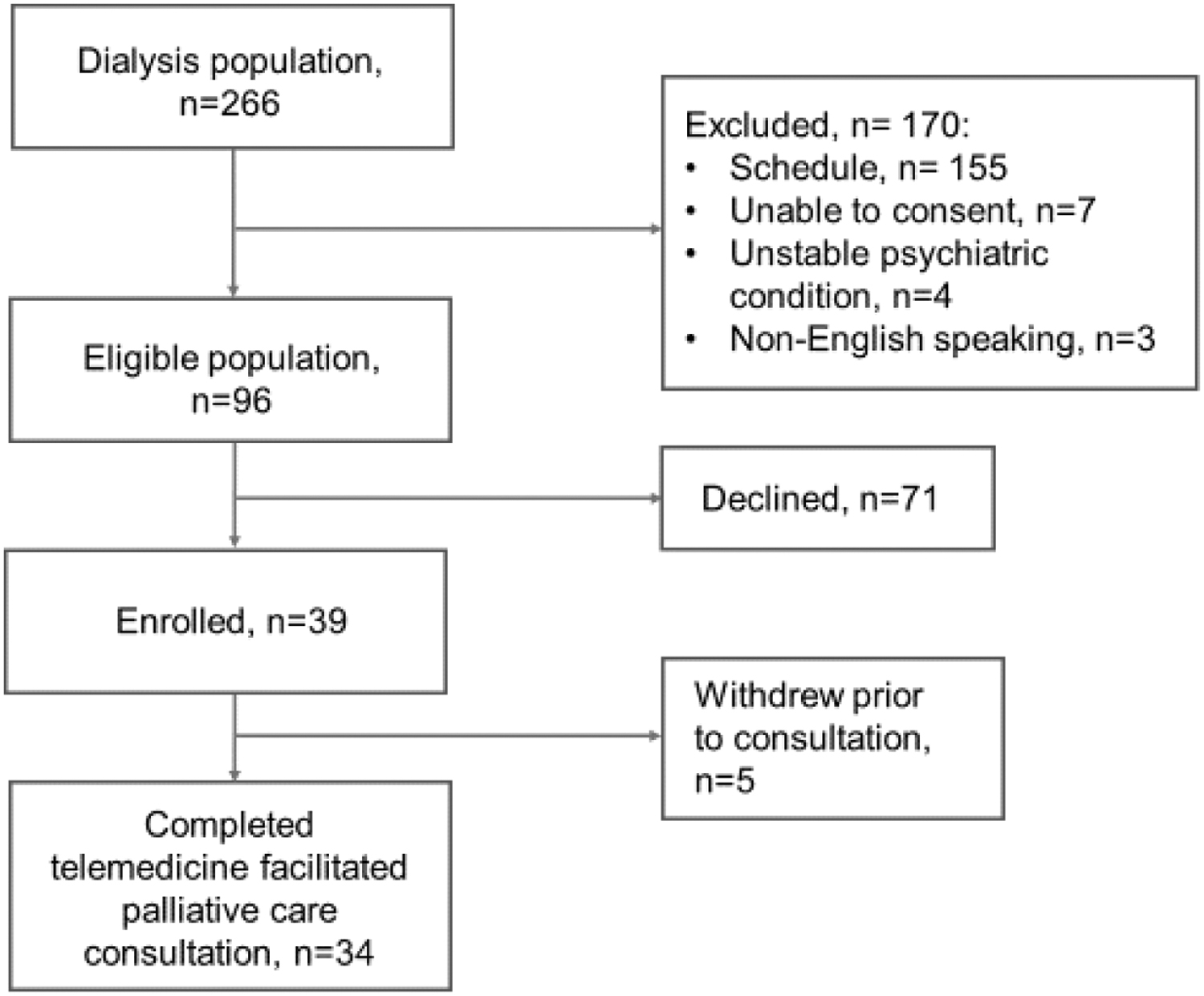
Flow diagram of patient recruitment.
Recruitment
In October 2018, we recruited clinician participants from the palliative medicine division at UVMMC to conduct teleconsultations. We recruited from five dialysis units with the most remote/rural location (Table 1). Between November 2018 and January 2020, we recruited patients based on matching dialysis shifts with clinician availability. Dialysis staff provided information to research staff regarding ineligible individuals, that is, non-English speaking, unable to provide consent. Informed consent procedures by trained research personnel occurred chairside in the dialysis unit and participants provided written consent. Patients were given the option during the consent process to choose to do the consultation before or after their scheduled dialysis treatments in a clinic room, or at home if they had Internet service and a device.
Recruitment across Rural Dialysis Units
UVMMC is the academic medical center from which the telepalliative care consultations originated.
Eligible participants include patients who meet inclusion criteria and are receiving dialysis at time when palliative care clinicians are available for outpatient telemedicine consultation.
UVMMC, University of Vermont Medical Center.
Intervention
Consult scheduling was coordinated with dialysis staff to avoid disruption with dialysis care (e.g., cannulation or administration of medications). In general, consults occurred 30 minutes after starting dialysis. Before the consultation, the research team provided the clinician with a patient summary, including dialysis vintage, etiology of kidney failure, and presence of advance directive/clinician order for life-sustaining treatment (COLST) on chart. This information was derived from nephrologist, dietician, and social worker notes in the dialysis electronic medical record, to which palliative care clinicians do not have access. To maximize privacy and audiovisual quality of the video recordings, the clinicians conducted the consult from the Telepresence Studio in the Vermont Conversation Lab using a large wall-mounted screen with a small camera on a freestanding tripod to position the camera in the clinician's sight line. The Lab is located within the Larner College of Medicine, adjacent to the UVMMC. Patients used an iPad that was mounted on a portable stand (IV pole) and positioned next to the dialysis chair. We used Zoom for the telemedicine platform and the password-protected medical center network was used for Wi-Fi connection. Dialysis staff or research personnel brought the iPad to the patient at the time of the consult, opened the Zoom app and returned at the end of the consult to remove the iPad. Patients were offered headsets as needed to cancel out ambient noise and to enhance privacy. Immediately preceding the consult, research personnel confirmed the patient wished to proceed with the research study and then introduced the palliative care clinician. Palliative care clinicians conducted consultations as per their usual practice and documented the conversation in the electronic medical record.
Measures
Clinician participants completed a survey at the time of consent and a telemedicine acceptability questionnaire survey after each consult. The telemedicine acceptability survey was adapted from similar intervention studies9,10 and questions were scored from 1 to 5, with lower scores indicating higher degrees of acceptability. Patient participants completed a baseline questionnaire on demographics, income, education, religious affiliation, experience with health care, and quality of life (physical and emotional overall scores). Immediately after the consult, patients completed the telemedicine acceptability survey. We assessed feasibility by the recruitment, scheduled, and completion rates. Our primary interest was one-month consultation completion rate among those who enrolled. We elicited patient and clinician feedback regarding the intervention using an open-ended question in the acceptability survey, “Do you have any comments or suggestions about today's tele-consult?” We summarized these data into themes with representative quotations from patients and clinicians.
Results
Feasibility
We enrolled four clinicians (three men and one woman; three MDs and one NP) to participate in video consultations with patients receiving dialysis. Between November 2018 and January 2020, we approached patients from five dialysis units for participation in this study and 39 enrolled (Table 1). Thirty-six completed the baseline survey and were scheduled for a teleconsult. Thirty-four completed the teleconsult and follow-up survey. Although one patient requested family be present, the family did not attend the scheduled teleconsult. All participants initially elected to have the teleconsult in the dialysis chair rather than in a private room. Thirty-two completed the teleconsult during dialysis treatment and two later decided to have the teleconsult in a private room immediately before dialysis treatment. One teleconsult was interrupted due to technical difficulties and was continued at a later date and follow-up survey was conducted after the second visit. Recruitment of patient participants is shown in Figure 1. Seventy-seven percent were completed within one month and the remainder were completed within four months.
Among the recruited participants, 24 were male, 16 were female, and mean age was 71.2 years. Nearly all patients self-identified as non-Hispanic white (n = 35). Baseline characteristics and quality of life measures are shown in Table 2.
Patient Baseline Characteristics
IQR, interquartile range; SD, standard deviation.
Acceptability
Acceptability scores were high, with a mean score of 1.75/5, on a 1–5 Likert scale where 1 and 2 indicated a measure was agreeable or helpful (Table 3). Eighty-one percent reported the teleconsult being at least as good as an office visit and 42% felt the teleconsult was better. Eighty-four percent felt the teleconsult was relevant, 6% were unsure, and 9% felt it was not relevant.
Acceptability of Telemedicine Rated by Patient Participants
Mean ± SD or n (%) unless specified.
Fifty-eight percent felt they learned new things about their condition, whereas 22% did not learn new things and 21% were unsure. Patients were split regarding whether the teleconsult changed the way they thought about dialysis: 28% felt it did, 38% were unsure, and 34% felt it did not change the way they felt about dialysis. Approximately half of the patients (56%) wished to meet with the palliative care clinician again and another 34% felt that they might want to meet again with the palliative care clinician.
The acceptability scores for the 33 consultations as rated by clinicians were similar to patients' scores (Table 4). In 60% of the teleconsults, clinicians rated the teleconsult at least as good as an office visit, and 36% felt it was better than an office visit.
Acceptability of Telemedicine Rated by Clinician Participants
Mean ± SD or n (%) unless specified.
Representative quotations from patients and clinicians are included in Table 5.
Representative Patient and Clinician Comments on Acceptability of Telepalliative Care in Dialysis Units
Discussion
We conducted a feasibility and acceptability study of telemedicine-facilitated palliative care consultations in patients receiving dialysis in a rural setting. We found the intervention to be feasible and acceptable with respect to audiovisual criteria as well as patient-reported relevance and helpfulness of the consultation. More than three-quarters of patients felt telemedicine was better or equivalent to an in-person consultation and more than half wanted to meet again with the palliative care clinician suggesting broad acceptance of telepalliative care. Patients who enrolled were scheduled for consults and three-quarters occurred within a month. To our knowledge, this is the first study demonstrating that telepalliative care is feasible and acceptable in patients receiving maintenance dialysis.
Integration of palliative care into usual dialysis care is still relatively uncommon. One approach is to train dialysis social workers and nephrologists, as was done in the Shared Decision Making Renal Supportive Care intervention. Patients with shortened life expectancy were enrolled across dialysis units in Massachusetts and New Mexico. 11 Social workers in the study felt that needing to be present in person was a barrier to future implementation, and nephrologists felt feasibility was limited due to time constraints and space resources. Another approach is to employ specialist palliative medicine physicians in the dialysis unit. A single-center study of 91 dialysis patients found that patients who underwent in-person consultations during their dialysis shifts were accepting of having palliative care conversation during dialysis and only one patient requested a private room to have the discussion. 12 Both this study and ours do not rely upon training nephrologists or dialysis staff to have serious illness conversations. Our study extends the current literature by demonstrating that palliative care clinicians do not need to be physically present in the dialysis unit. This finding may help to reduce barriers for rural patients and improve access to specialist palliative care.
Little is known about telemedicine conducted at in-center dialysis units. Before the severe acute respiratory syndrome coronavirus-2 (SARS CoV-2) pandemic, the use of telemedicine in dialysis was limited to home dialysis or patients in remote locations. Since the pandemic occurred, the Centers for Medicare & Medicaid Services (CMS) lifted these restrictions, temporarily allowing for teledialysis visits. 13 Previous studies of telemedicine and dialysis have typically focused on care of pediatric populations or home dialysis monitoring. Modes of telehealth communication interventions have included telephone calls, remote monitoring software, and, less commonly, videoconferencing. In prior studies, care was provided by nurses, health care teams, and nephrologists, but none addressed specialty care delivered through telemedicine.14–25 In addition, prior studies used telemedicine to deliver care to patients at home, whereas our study demonstrates the use of telemedicine with the patient at satellite dialysis units. We report that patients are accepting of meeting new clinicians and undergoing palliative care consultations through telemedicine during dialysis. Although clinicians were also accepting of telemedicine, qualitative data identified issues, including noise and interruptions, as well as decreased alertness potentially due to the dialysis procedure negatively impacting the quality of the consultation (Table 5).
Although this study occurred just before the emergence of SARS CoV-2 in our region of the United States, there are several relevant insights for care during the pandemic. Simple and preexisting technology in our dialysis units, including an iPad mounted on an IV pole, can facilitate telemedicine. This allowed patients to access specialty care from clinicians located at a distance and the device was easily sanitized between patients. Perhaps justifying the use of telemedicine during a pandemic, patients are already accepting of the use of telemedicine for serious illness conversations and many felt that telemedicine was as good, if not better, than an in-person visit. Patients were willing to have conversations during their treatments and generally did not request that family members be present; absence of family became a new standard of care during the pandemic. Although we have used teledialysis in the past between patients and their nephrologists, these telepalliative care conversations were conducted by clinicians not known to the patient and were still deemed to be acceptable.
There are limitations to consider. (1) Although our study participants expressed broad acceptance of telepalliative care, this is likely a selected group who were willing to participate in a telemedicine research study focused on palliative care. Reasons nonparticipants offered for choosing not to be part of the study included not liking telemedicine. It is not known if this is due to poor experiences in the past with the technology, a preference for in-person connection, patient sensory limitations to this mode of communication, or other reasons, as this was not the goal of our study. Although the participation rate was similar to what has been reported in other palliative care interventions, 26 these barriers should be explored and addressed in dialysis units considering integrating telepalliative care. It is also conceivable that in time of crisis or high need for palliative care services, more patients might be willing to accept telepalliative care. Telepalliative care could also be used as a follow-up to an in-person or in-patient consultation. (2) Selection bias may also have been introduced due to tendency to recruit patients from daytime dialysis shifts. It is possible that these patients differed, for instance, in their acceptance of telepalliative care or experience of palliative care consultations compared with those who participated during the daytime. For instance, healthier patients could be preferentially dialyzed on the evening shift and might be less accepting of palliative care. Alternatively, healthier patients may have been more likely to follow through with the consultation and/or found it easier to engage with telemedicine, thus increasing the feasibility and acceptability. (3) Patients receiving maintenance dialysis in our region do not reflect the race/ethnic characteristics of the U.S. dialysis population. However, some characteristics were similar to national samples, including age, socioeconomics, and baseline quality of life. 8 It is not known at this time if more diverse patient groups might be more or less accepting of telemedicine in dialysis care.27,28 Further study in larger and diverse populations is needed to determine the stability of our estimates. (4) Our center is developing an outpatient palliative care practice that relies in part on our established telemedicine infrastructure. The generalizability to other centers without these resources may also be a limitation. (5) Although participants were accepting of the intervention, the quality of the palliative care consultations may have been impacted by lack of privacy in the dialysis unit.
Conclusion
Telemedicine-facilitated palliative care consultations in rural dialysis units are feasible and acceptable to patients receiving maintenance dialysis. Future studies should evaluate the impact of ongoing palliative care consultations on symptom burden, participation in advance care planning, dialysis withdrawal, satisfaction with care, and quality of life.
Footnotes
Authors' Contributions
K.L.C., M.K.T., R.D.S., T.R., M.A.L., and R.G. contributed to the conception and design of the study, methodology, and interpretation of the data. K.L.C. acquired funding, wrote the original draft, collected the data, and conducted the formal analysis. M.K.T., R.D.S., T.R., M.A.L., and R.G. revised and edited the article.
Acknowledgment
The authors gratefully thank the patient and clinician participants in this study.
Funding Information
Research reported in this publication was supported by the National Palliative Care Research Center Career Development Award (K.L.C.). R.G. was supported by the Bob and Holly Miller Endowed Chair in Palliative Medicine. Research was also supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number P20GM135007: Vermont Center for Cardiovascular and Brain Health (K.L.C.).
Author Disclosure Statement
No competing financial interests exist.