
Abstract
Background:
Perceived self-efficacy in advance care planning (ACP) is frequently used to measure the impact of ACP programs for professionals responsible for advanced chronic patients. A validated ACP Self-Efficacy (ACP-SE) scale is not currently available in Spanish.
Objective:
To culturally adapt and validate Baughman's ACP-SE scale into Spanish (ACP-SEs).
Methodology/Design:
An instrumental study was performed in two phases: (1) cultural adaptation of the ACP-SE scale and (2) psychometric properties measurement.
Setting/Participants:
The survey was sent to 5785 professionals: physicians, nurses, psychologists, and social workers, members of scientific associations in the areas of primary care, geriatrics, and palliative care in Catalonia, Spain.
Results:
Five hundred thirty-eight questionnaires were obtained, respondents were physicians (69.0%) and nurses (28.4%) and mean age was 47 years (standard deviation [SD] = 10.1). Most were women (79.6%), 68% had >15 years of professional experience, and 80.7% worked in primary care. Internal consistency was high (Cronbach's alpha = 0.95) and showed a unidimensional structure explaining 56.2% of total variance. Mean score was 67.37 (SD = 16.1). Variables associated with greater self-efficacy were previous training (t = −3.23, df = 273.76, p = 0.001), previous participation in ACP processes (t = −6.23, df = 521, p < 0.001), and membership in geriatric or palliative care scientific association (p < 0.001). ACP-SEs positively correlated to other compared scales.
Conclusion:
The ACP-SE scale demonstrates adequate psychometric properties. This is the first self-efficacy scale for ACP in Spanish. It should facilitate a better understanding of implementation processes related to ACP programs for professionals involved in caring for patients with advanced diseases.
Introduction
Advance care planning (ACP) enables individuals to define goals and preferences for future medical treatment and care, to discuss these matters with family and health care providers, and to record and review these preferences when appropriate. 1 Patients, their families, and the health care professionals who care for them participate in this process, which is particularly significant when the individual can no longer make his/her own decisions. ACP has become ever more important in recent years, and it is increasingly being integrated into health care models and policies for individuals with advanced chronic disease (ACD). 2 The proper implementation of ACP requires that the concept underlying the process be widely disseminated to promote a greater understanding of it. In addition, it is also essential to implement measures to ensure that the patient's ACP-related data are registered in an integrated information system. 3
The systematic integration of ACP in routine health care practice presents a challenge for public health systems.4,5 Barriers to ACP implementation among health care professionals include the following: insufficient knowledge about the ACP process; inadequate communication skills; fear of talking about end-of-life processes with patients; difficulties in managing ethical-clinical dilemmas; and the absence of a clearly defined role for professionals responsible for managing the ACP process.6,7 Caring for people in final stages of their lives requires professionals to have high levels of emotional intelligence to manage the effect of continuous contact with difficult conversations, including care goals expectations, suffering and death, and dying.8,9
Training is essential to overcome these barriers and to improve the self-confidence of professionals during the ACP process. Research shows that skill acquisition can be improved by increasing the professional's perceived capability to conduct the ACP, 10 a construct defined as “self-efficacy,” which refers to the individual's belief in his/her ability to carry out a particular task.11,12 Indeed, perceived self-efficacy is one of the main predictors of success in learning processes and in promoting the acquisition of new behaviors in general, 13 and ACP in particular. 14
Data from recent studies indicate that greater self-efficacy is a predictor of positive outcomes when implementing ACP. However, some of those studies have used ad hoc or nonvalidated instruments to measure self-efficacy.15,16 Baughman et al.14,17 developed and validated an instrument to measure self-efficacy, known as the ACP Self-Efficacy (ACP-SE) scale. The ACP-SE contains 17 items rated on a 5-point Likert-type scale. The validation process obtained a unidimensional structure with a single factor that explained 58.38% of total variance. The scale showed good internal consistency (Cronbach's alpha = 0.95). In that study, Baughman et al. surveyed a random sample of primary care physicians, 14 finding that 35% of physicians had initiated the ACP process in 75% or more of their patients with life-limiting illnesses. However, only 34% of those physicians had received specific training in ACP.
To our knowledge, this is the first and only validated scale in English about ACP-SE and one does not exist in Spanish. Given the growing international relevance of ACP, there is a need for validated tools to assess self-efficacy in languages other than English to measure the impact of professional training on self-efficacy in ACP implementation programs.
The aim of this study was to translate, culturally adapt, and validate the original ACP-SE scale into Spanish (ACP-SEs). We expect that the ACP-SEs will show psychometric properties in terms of internal consistency and positive correlations in terms of convergent validity in a sample similar to the original scale and adjusted to the cultural context.
Materials and Methods
Design
An instrumental study was performed. This was carried out in two phases: an initial phase in which the translation and cultural adaptation of the ACP-SE scale were conducted and a second phase in which the behavior of its psychometric properties was measured.
Translation and cross-cultural adaptation
The translation and cultural adaptation of the ACP-SE scale was carried out in accordance with the recommendations of the International Test Commission. 18 We obtained permission from the authors of the original scale to translate it into Spanish. The scale was translated separately by three professionals with an excellent command of the English language. These include a philologist, an expert in cross-cultural adaptation, and an expert in ACP. The only item that needed discussion was the one that reflected the verb “engage,” which required an adaptation since it does not have a direct translation in Spanish. The three versions were then evaluated by the research team and one single version of the Spanish scale was reached.
Two bilingual individuals, both qualified translators, back-translated the scale into English. Both versions were compared to the English original one. The three forms displayed very good similarity.
To ensure this scale included all the elements that define the ACP according to the current clinical practice in our context, we added two additional items to the original scale: (1) involve the patient in the discussion about ACP, as was used by Baughman et al. as a global question on ACP-SE and the base to the ACP_SE scale 14 and (2) correctly register the agreed plan over the course of the ACP, was added because registration of ACP-related data is an important phase in the implementation of ACP process in our context. 2
A final Spanish language version (19 items) was reviewed by a group of experts in primary and palliative care and ACP, ensuring that all items were understandable and clear. No relevant modification was made. Finally, the definitive Spanish version was considered complete (Supplementary Table S1).
Sample
For the second phase, a convenient sample, enlarged from Baughman's study, was defined. It included members of four scientific associations closely involved with the patient populations that need ACP, as follows: (1) Catalan-Balearic Association for Palliative Care (in catalan SCBCP; 340 members), (2) Catalan Association for Geriatrics and Gerontology (SCGiG; 422 members), (3) Catalan Association for Family and Community Medicine (CAMFiC; 4223 members), and (4) Catalan Association for Family Nursing (AIFiCC; 800 members). Thus, the total sample comprised physicians, nurses, psychologists, and social workers.
Measurement instruments
The questionnaire contained three sections (survey available upon request): (1) sociodemographic variables (age, gender, profession, professional experience health care setting, years of experience in the specific setting, and type of membership); (2) variables to assess prior knowledge, training, and experience with ACP; and (3) a final section that included four scales, three of them used for the convergent validity, as follows:
ACP-SEs scale, containing 19 items rated on a 5-point Likert-type scale (1: not at all capable and 5: completely capable). Wallston's Personal Competence Scale,
19
which evaluates the individual and generalized perception to overcome/cope with difficult situations, in its Spanish version validated by Fernández-Castro et al.,
20
comprised 8 items (4 positive and 4 negative) rated on a 6-point Likert-type scale (1: totally disagree and 6: totally agree). Cronbach's alpha for this version was 0.83. Trait Meta-Mood Scale (TMMS-24) developed by Salovey et al.,
21
modified and adapted to Spanish by Fernández-Berrocal et al.,
22
which assesses perceived emotional intelligence. Later, the factor structure of the Spanish instrument was confirmed in a sample of health professionals (Aradilla-Herrero et al.).
23
This is a 24-item scale rated on a 5-point Likert-type scale that measures three emotional dimensions (attention to, clarity of feelings, and mood repair). Cronbach's alpha for the validated version in a sample of nurses and nursing students was 0.87 for attention and clarity and 0.84 for repair.
23
Bugen's Coping with Death Scale
24
was initially designed to assess the ability of professionals to cope with death after specific training in the subject. The short version was validated by Galiana et al.
25
in a sample of palliative care professionals. It includes nine items rated on a 7-point Likert-type scale (1: totally disagree and 7: totally agree). Cronbach's alpha for the short version was 0.85.
Procedure and ethical considerations
The questionnaire was created using the RedCap platform. Presidents of each society were invited to participate. They were responsible for sending, by internal mailing, the link to the questionnaire to the members of the aforementioned scientific associations in October 2018. The primary investigator did not have access to the participants' email addresses and the decision to respond to the survey was entirely voluntary and anonymous. All responses were coded for test-retest purposes. Professionals agreed to participate by responding to the survey. Three reminders were sent to increase the participation rate and one reminder for the retest. The latest retest was sent in December 2018. The estimated time needed to complete the survey was 15 to 20 minutes (5 minutes for the retest).
All research procedures used in this study were established in accordance with the Declaration of Helsinki. The ethics committee at the University of Vic reviewed the study protocol and it was approved by the code RS005_S. Moreover, the study was designed in accordance with the ethics criteria established by Spanish Organic Law 3/2018 of 5 December on personal data protection and the guarantee of digital rights, following the General Regulation (EU) 2016/679 of April 27, 2016, on data protection.
Data analysis and psychometric evaluation
Data analysis included a description of the participants' sociodemographic profile as well as determination of internal consistency, test-retest reliability, and concurrent and discriminant validity. The total score on the ACP-SEs was calculated as the sum of scores for the items, which was rescaled from 0 (minimum) to 100 (maximum) score. 26
The internal consistency of each item was analyzed in terms of the corresponding dimension using Cronbach's alpha coefficient. The minimum coefficient for each item was set at 0.7 to consider the measure acceptable. Construct validity was evaluated through an exploratory factor analysis carried out using polychoric correlations between items and unweighted least squares using the R statistical software psych package (v. 1.7.8).
To evaluate construct validity, the mean scores on the ACP-SEs were compared according to known groups and the magnitude of the effect was estimated by calculating the standardized mean differences (Cohen's d effect size). 27 To determine convergent validity, the ACP-SEs scores were compared with the other scales using Pearson's correlation coefficient.
Estimators of the 95% confidence interval (CI) and the statistical significance criterion were set at α < 0.05. The data were managed and analyzed using R (v.3.4.4) for Windows.
Test-retest
For the analysis, the intraclass correlation coefficient (ICC) was calculated and the two measures were compared using Student's t-test for paired data or the Wilcoxon signed rank test for related data, according to the distribution of the variables.
Results
Sample characteristics
After the back-forward translation process, a 19-item ACP-SEs was performed. The validation survey was sent to 5785 professionals, and 538 valid responses were received (response rate: 9.29%) (Fig. 1).
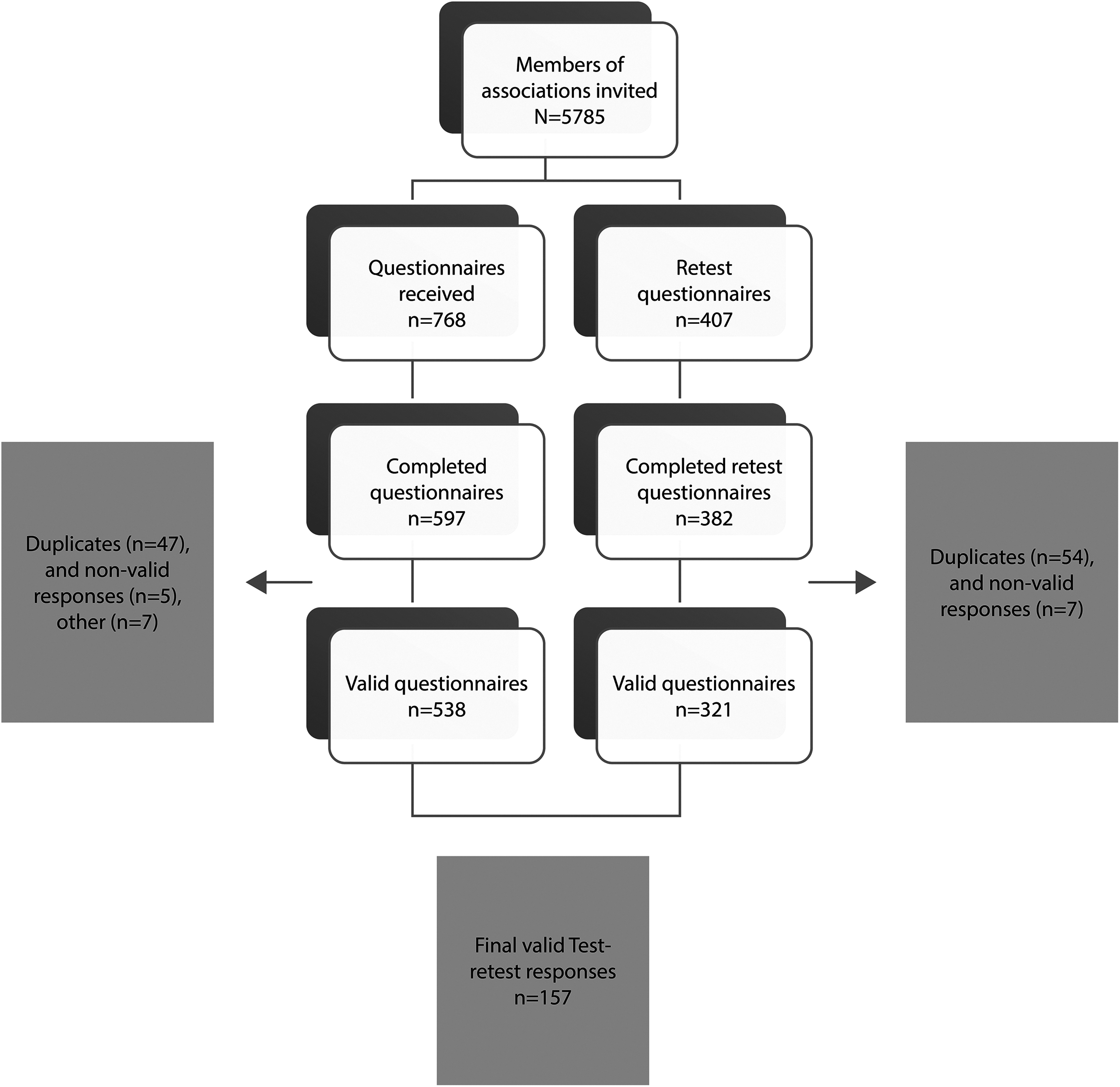
Flow chart of sending and collection of questionnaires, with an initial sample of 5785 professionals.
Majority of responses were obtained from physicians (69.0%) and nurses (28.4%). The mean age was 47 (standard deviation [SD] = 10.1). Most respondents were women (79.6%), had ≥15 years of professional experience (68%), and worked in primary care settings (80.7%) (Table 1).
Demographic and Professional Characteristics of the Participants
SD, standard deviation.
Reliability and dimensionality
The internal consistency of the scale was high (Cronbach's alpha = 0.95). The scale was unidimensional, loading a single factor that explained 56.17% of total variance (Fig. 2).
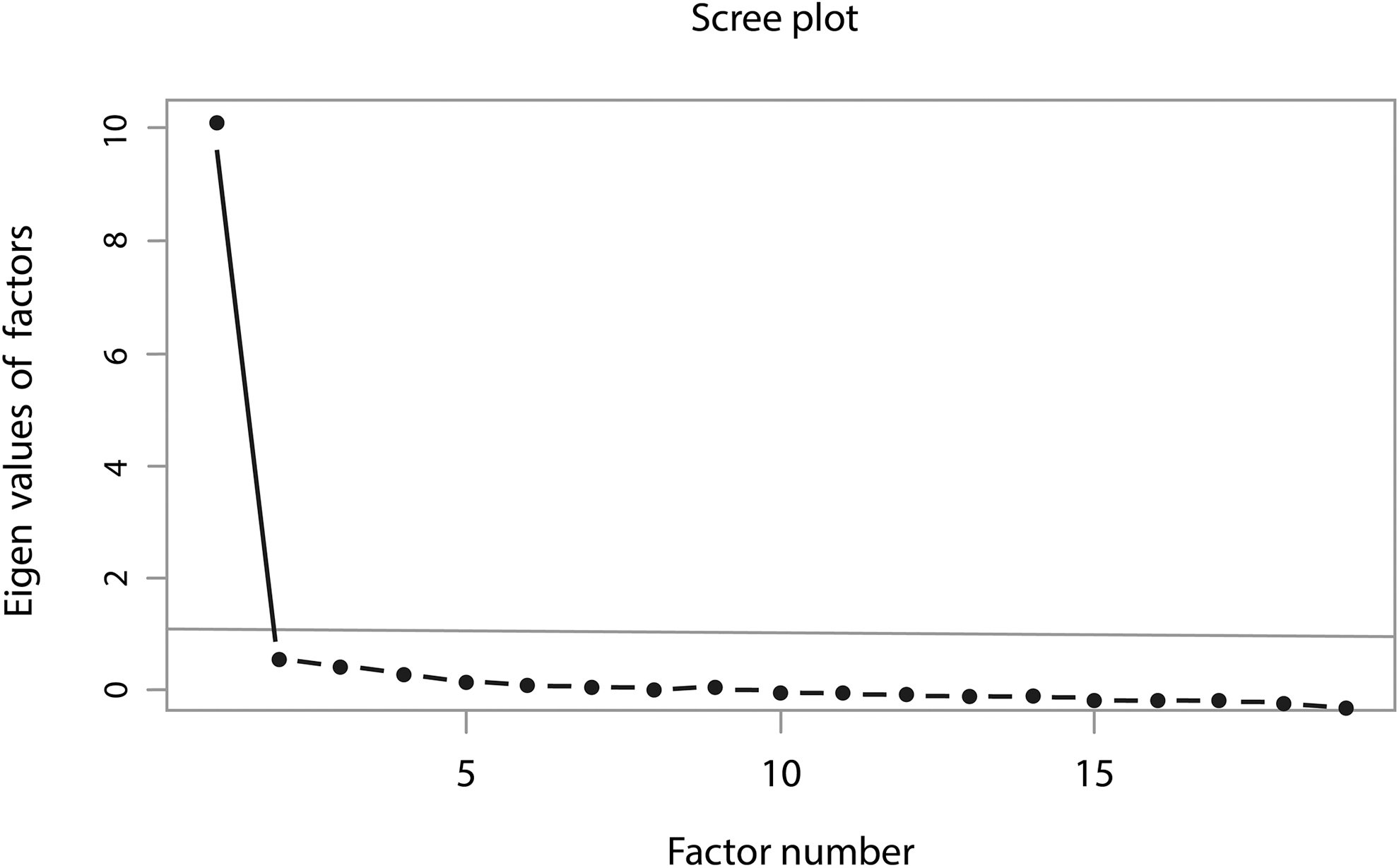
The scree plot supported a one-factor solution.
All scores were >0.62, except for item 10 (ensure that patient's treatment preferences will be honored at a hospital if patient is hospitalized), which was 0.43. However, that item was retained to ensure comparability with the original scale (Table 2).
Factor Loading Items for the One-Factor Solution of the ACP-SEs Compared with the Original ACP-SE Factor Loading Items;
Items exclusive to the Spanish version.
ACP-SE, Advance Care Planning Self-Efficacy.
The resulting mean score (sum of item values) was 67.37 (SD = 16.1).
Test-retest reliability
For the retest, 321 responses were obtained, and 157 were paired. (Fig. 1) The median time between the test and retest was 37 (21–43) days, although this time was <15 days in 21 cases. The test-retest ICC was 0.88 (95% CI: 0.83 to 0.91). No statistically significant difference between the test and retest scores was observed (t = −1.12, df = 156, p = 0.26).
Comparison between groups
Known groups were compared in terms of sociodemographic variables and ACP practice. (Table 3) There are no significant differences in terms of age and years of experience in the specific setting or professions. Statistically significant differences in terms of gender were observed, with men scoring higher on the ACP-SEs. Given the limited number of responses received from social workers (n = 6) and psychologists (n = 8), they were underrepresented in the sample.
Comparison of ACP-SEs Values among Known Groups
p < 0.05; ***p < 0.001.
Significant differences were also observed between participants with and without previous ACP training (t = −3.23, df = 273.76, p = 0.001). However, the magnitude of effect was low (Cohen's d = −0.32), with a mean difference of −5.12 (95% CI: -8.24 to -2).
Significant differences were observed in the ACP-SEs score between professional with and without prior ACP experience, with scores significantly higher among professionals with prior experience (t = −6.23, df = 521, p < 0.001). The magnitude of the effect was moderate (Cohen's d = −0.54), with a mean difference of −8.4 (95% CI: -11.05 to -5.75).
Finally, participants belonging to the SCBCP (Palliative Care) and SCGiG (Geriatrics) had significantly higher self-efficacy scores than nonmembers (Table 3). For the other two associations, no significant difference was observed between members and nonmembers.
Relevance to other variables
As we observed in Table 4, the ACP-SEs was positively and significantly correlated with the Wallston's Perceived Competence Scale and Bugen's Coping with Death Scale, as well as with the TMMS-24 subscales (attention, clarity, and repair) (Table 4).
Pearson's Correlation Coefficient between ACPS-SEs and the Compared Scales
p < 0.05; **p < 0.01; ***p < 0.001.
BCDS, Bugen's Coping with Death Scale; TMMS-24, Trait Meta-Mood Scale; WPCS, Wallston's Perceived Competence Scale.
Discussion
The proposed Spanish-language version of the ACP-SEs scale demonstrates adequate psychometric properties in a sample of professionals closely involved with the patient population beneficiaries of ACP processes. The results confirm that it is a unidimensional scale. During the cultural adaptation process, two items were added to the scale to adapt it to the ACP model in Catalonia, including one item to assess the professional's perceived capacity to involve the patient in the discussion about ACP and the capacity to correctly register the ACP data.
This study was conducted in a group of professionals who routinely care for individuals who could benefit from ACP. The respondents, physicians and nurses, work in a wide range of settings, mostly primary care, and are aware of the ACP concept.
One of the main findings of this study is that professionals with previous training in ACP had a higher level of perceived ACP-related self-efficacy than those without previous training. This suggests that promoting training among professionals who care for individuals eligible for ACP would allow those professionals to reflect on and express their wishes, expectations, preferences, and values with regard to health-illness processes. 28
Interestingly, the number of years of professional experience on the specific setting was not significantly associated with perceived self-efficacy. Although this finding is consistent with previous studies,14,29 it was nonetheless somewhat surprising, given that a previous survey in Spain (Palliative Care professionals) found a significant association between years of professional experience and training with perceived self-efficacy. 30 However, it is worth noting that most responses in our study came from primary care professionals, who might conduct ACP processes less frequently than palliative care professionals, who are mainly involved in caring for potential candidates for ACP.
Another significant finding was that professionals who had previously applied ACP had a greater perceived self-efficacy. These results are consistent with those of Baughman et al., 14 further confirming that more experience with ACP is associated with higher levels of self-efficacy.
We also found that professionals belonging to the SCBCP and SCGiG had a greater level of ACP-SE. This may be because these professionals—who regularly care for individuals with ACD or at final stages of life—are more involved in implementing care models to promote patient autonomy31,32 and in initiating discussions about suitable therapy, place of care, and patient expectations 33 —all of which are key components of ACP. 34 Working with a specific framework of care could promote a wide range of skills to cope with difficult conversations on clinical practice, 33 especially during the last phases of life or dying.
Many strategies have been developed to help professionals discuss questions related to death or dying with patients, 35 but many professionals continue to encounter difficulties with it 36 and many also report a lack of training in communication skills related to this aspect.37,38 Our study suggests that professionals who are better able to manage the issue of death would have a higher degree of self-efficacy in ACP and a greater ability to manage their own emotions. Previous studies have shown that professionals with less anxiety toward death understand and manage their emotions better. 23 In this regard, the way professionals personally cope with death can regulate their efficacy to manage the emotions surrounding end-of-life processes and they may thus feel better able to initiate difficult discussions with patients. 8
Training to acquire the skills needed to conduct ACP process may include contents about communication skills, 15 self-awareness, and coping strategies related to death and dying. These elements can overcome the barriers and difficulties expressed by professionals with regard to initiating the aforementioned difficult conversations, 39 and training could also help to promote a positive attitude when these professionals need to discuss end-of-life care with their patients. 40
The ACP-SEs scale could be a useful tool to not only assess ACP training and implementation programs, particularly to measure the impact of such programs, but also to identify how mature, predisposed, informed, and well-trained professionals feel with regard to caring for individuals with ACD and their families.
One of the limitations of this study is the low response rate. We had expected a higher response rate, which would have better reflected the diversity of the sample, including professionals from different health care disciplines, such as psychologists or social workers. Most respondents were primary care professionals who, unlike professionals working in PC and geriatrics, take care of a wide range of patients, and not only those who benefit from ACP. As the aim of the study was the cross-cultural adaptation and validation of the ACP-SE scale, we consider that the data collected were a sufficient response to the main proposal of the study.
Finally, although prior training had a significant effect on self-efficacy, the magnitude of the impact was low. In this regard, it is worth noting that professionals receive diverse types of training on ACP, and thus the actual level of knowledge acquired could be quite diverse.
Conclusion
The Spanish ACP-SE scale demonstrates appropriate psychometric values. It is the first self-efficacy scale for ACP to be validated in Spanish. The ACP-SEs could be considered an essential tool for evaluating self-efficacy on ACP. In further research, assessing professionals' perceived self-efficacy in managing ACP processes could be highly relevant for the development and design of training programs whose aim is to implement ACP processes in individuals with advanced illnesses.
Footnotes
Authors' Contributions
C.L., A.A.-H., and M.S. conceptualized and designed the study. C.L. and A.A.-H. were involved in data collection, N.M. performed the statistical analysis, and C.L., A.A.-H., and M.S. contributed to data analysis and interpretation of the findings. C.L., A.A.-H., and M.S. wrote the draft of the article. C.L., A.A.-H., M.S., and N.M. reviewed and approved the final article. All authors meet conditions of the International Committee of Medical Journal Editors regarding authorship.
Acknowledgments
We would like to thank the people and organizations that have supported this study. We would also like to thank Bradley Londres for professional language editing and Dr. Pablo Martínez for the external revision of this article.
Funding Information
Publication of this article is supported by the grant awarded by Barcelona's Official School of Nursing (Project Code: PR-363/2019).
Author Disclosure Statement
The authors have no intellectual passion, political, religious, and institutional affiliations, which might lead to a conflict of interest in making this article. The lead author affirms that the article is an honest, accurate, and transparent account of the study being reported; that no relevant aspects of the study have been omitted; and that any discrepancy from the study as planned has been explained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.