
Abstract
Purpose:
Guidelines suggest that advance care planning (ACP) and goals-of-care discussions should be conducted for patients with advanced cancer early in the course of their disease. A recent audit of our health system found that these discussions were rarely being documented in the electronic medical record (EMR). We conducted a quality improvement initiative to improve rates of documentation of goals and wishes among patients with advanced cancer.
Methods:
On the basis of previous analyses of this problem, we determined that provider capability and opportunity were the main barriers to conducting and documenting serious illness conversations. We implemented the serious illness care program (SICP), a systematic multicomponent intervention that has shown potential for conducting and documenting ACP discussions in two oncology clinics. Our goal was to conduct at least 24 serious illness conversations over the implementation period, with documentation of at least 95% of all conversations.
Results:
The SICP was implemented in two outpatient medical oncology clinics. A total of 15 serious illness care conversations occurred and 14 (93%) of these conversations were documented in the EMR. Total rates of documentation increased between the preimplementation and implementation period (4.2%–5.4% for clinician A and 0%–7.3% for clinician B).
Conclusion:
Implementation of the SICP resulted in increased rates of documentation, but the target number of conversations was not met. Further improvement cycles are required to address barriers to conducting and documenting routine serious illness conversations.
Introduction
Communication between oncologists and patients with life-limiting illness regarding their goals and values is an important aspect of quality patient care. Studies have shown that timely high-quality conversations are associated with improved quality of life, less distress, earlier use of palliative services, and improved family bereavement.1–5 In addition, several national guidelines suggest that goals-of-care discussions should be conducted for patients with advanced cancer early in the course of the disease.6,7
In our health system, despite having clear advance care planning (ACP) and goals-of-care designation (GCD) policies and procedures, a recent audit found that only 7.2% of 12,000 per quarter active cancer patients in our cancer center's electronic medical record (EMR) had a documented GCD (a medical order describing the general goals of care and the interventions and locations of care that might be used or withheld in service of these goals). 8 In addition, only 0.4% of active cancer patients had documentation of their values and priorities in the system's ACP/GCD tracking record.
Analysis of this problem in our health system has been conducted previously.9,10 We found that capability (i.e., some providers feeling inadequate in their skills in conducting these conversations) and opportunity (the lack of time in clinic, knowing which patients may be appropriate for an ACP/GCD conversation) were the major barriers for clinicians in conducting and documenting ACP/GCD conversations.
Similar findings have been reported in the literature.11–13 The serious illness care program (SICP) was recently shown in a cluster randomized trial to result in more, earlier, better, and more accessible documentation of ACP/GCD conversations. 5 Given that this intervention was a multicomponent intervention that addressed several components of the specific barriers we identified, we chose to implement this program as our quality improvement intervention.
Specific aims
The aims of this initiative was to identify at least 24 patients (12 patients per clinic) for a serious illness care (SIC) conversation and that at least 95% of all conversations would be documented in the EMR. These aims were developed based on discussions that concluded it would be feasible/reasonable to have one conversation per clinic per week, in three out of every four weeks.
Methods
We used the SICP implementation roadmap 14 to guide the intervention and workflow process adaptations. We chose two outpatient oncology clinics each with one medical oncologist (clinician). These were chosen based on self-selection of clinicians interested in implementing the SICP within their clinics.
Interventions
Provider training
A SICP-trained facilitator provided each clinician with a two-hour training session based on the SICP model. This included an overview of the principles and the practices of the program, the benefits of implementation, and a review of patient identification. Each clinician was provided with the Clinician Reference Guide. 15
Identification of patients
At the beginning of each 16-week period, the clinician together with his or her primary nurse was asked to identify at least one patient scheduled to be seen in clinic that week that would be appropriate for an SIC conversation. This was based on the patient meeting one or more of the following criteria: (1) a response of “no” to the question “would I be surprised if this patient died within the next year” or (2) any patient with a diagnosis of metastatic pancreatic cancer (due to the poor prognosis of less than one year in this population), or (3) symptom scores of >7 (out of 10, where 10 is the worst possible score) on more than three categories on our patient-reported outcome dashboard. 16
During the upcoming clinic visit, the nurse would provide the identified patient with the preclinic visit letter to prepare them for the SIC conversation. 17 This letter asked the patients to think through what is important to them and their wishes for the future, as well as whether these wishes had been shared with their loved ones. The subsequent visit with the patient would be scheduled during the last appointment of the clinic to allow adequate time to conduct the conversation. After the conversation, the clinician would document the conversation in the EMR as well as fill out a GCD order, if it was obtained during the conversation. Within 48 hours of the conversation, a postconversation survey (Supplementary Appendix SA1) was completed by the patient, as well as the clinician (Fig. 1).
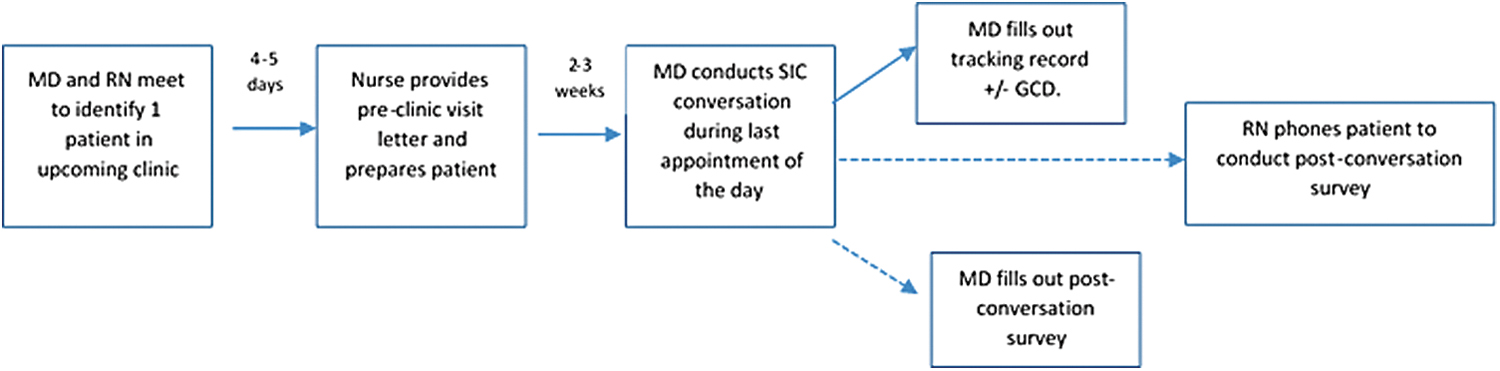
Flowchart depicting process of identifying patients and conducting the serious illness care conversation. Depicts part of the implementation process, Depicts an evaluation process. Color image is available online.
Clinician A implemented the SICP in the 16-week period from June 1 to September 20, 2019. This was followed by a debriefing session to synthesize the lessons learned that were then shared with clinician B. Clinician B implemented the SICP in the 16-week period from September 30, 2019, to January 17, 2020.
Measures
In each 16-week period, we collected data on the number of SIC conversations that took place and the number of conversations that were documented on the ACP/GCD tracking record in the EMR.
We analyzed data on a weekly basis and used a statistical process control chart (p chart) to assess the differences in documentation rates on the ACP/GCD tracking record between the 8 weeks preimplementation and during the implementation of the SICP in each 16-week period.
We received approval for this initiative by the Health Research Ethics Board—Cancer Care (HREBA.CC-19-0135).
Results
A total of 16 patients were identified for the SIC conversation (8 patients in each clinic). One patient was lost to follow-up. Patient characteristics are given in Table 1.
Patient Demographics of the n = 16 Patients Identified for the Serious Illness Care Conversation
GEJ, gastroesophageal junction.
Clinician A conduced seven SIC conversations over the 16-week period. Of those, six (86%) patients had a documented discussion on the ACP/GCD tracking sheet. Clinician B conduced eight SIC conversations over the 16-week period. Of those, all eight (100%) had a documented discussion on the ACP/GCD tracking sheet.
Figure 2 shows the preimplementation GCD tracking record rates (for any patient) compared with rates during the intervention for clinician A (Fig. 2a) and clinician B (Fig. 2b) using a statistical control chart (p chart). For clinician A, the average documentation rate increased from 4.2% in the eight weeks before implementation to 5.4% during the implementation. Special cause variation occurred at week 14 (i.e., week 6 of the intervention). For clinician B, the average documentation rate increased from 0% in the 8 weeks before implementation to 7.3% during the implementation with special cause variation occurring at week 10 (i.e., week 2 of the intervention).

Statistical control chart (p chart) for advance care planning/goals-of-care tracking record documentation rates preimplementation and during implementation of the serious illness care program for normal variation in the data;  , special cause variation in the data; UCL, upper control limit. Color image is available online.
, special cause variation in the data; UCL, upper control limit. Color image is available online.
Supplementary Figure S1 shows the results of the patient and oncologist surveys.
Discussion
In this quality improvement initiative using the SICP in two outpatient oncology clinics, we met our primary outcome of documenting at least 95% of all SIC conversations in the EMR. However, we were unable to achieve our goal of achieving at least 12 conversations in each 16-week period.
The rates of documentation of a patient's goals and wishes in our initiative are comparable with those from the recent randomized clinical trial. 5 In that study, 96% of patients who were part of the SICP intervention arm had a documented discussion compared with 79% of controls. Similarly, in our intervention, 86%–100% of all patients had documentation on the ACP/GCD tracking record, which was easily accessible in the EMR. High rates of documentation in the EMR after an SIC conversation have also been reported through a quality improvement initiative in primary care. 18
Although our improvement initiative addressed several provider and system-level barriers in our health system, we were unable to meet our goal of conducting at least 12 conversations in each 16-week period. The reasons identified by the clinicians and their primary nurses for this were inability to identify a patient who met the inclusion criteria on a weekly basis (either because of time limitations or no patient meeting the criteria in a given week), failure of the patient to show up for the scheduled appointment time, or issues with the clinic scheduling process that failed to book the patient during the appropriate time.
In addition, in our initiative, clinicians had to manually identify patients for the SIC conversation and we did not use an EMR trigger to identify patients and cue clinicians, which is a recommended part of the SICP implementation. Clinician training around how to best use EMRs for documenting SICP conversations may have also helped in meeting our goal. We plan to adapt the process based on these findings, before future improvement cycles.
Our initiative should be reported in the context of several limitations. It was conducted at a single urban academic cancer center, so our results may not be generalizable to other settings. It was also only conducted in the outpatient setting, so may need to be adapted when used with hospitalized patients, which may be a focus of future research. In addition, the clinicians in this initiative were self-selected and, therefore, likely represent early adopters of the SICP. Therefore, our findings may not be reproducible with less engaged clinicians.
Additional limitations include the small sample size and that we did not evaluate our intervention beyond 16 weeks to determine whether it was sustainable. Furthermore, we did not analyze the quality of the documentation of the SIC conversation in the medical record. The strengths of this initiative include that the intervention was simple, low cost, and used the existing resources within our health system and EMR to implement the SICP.
In conclusion, this quality improvement initiative using the SICP in an outpatient oncology setting led to improved rates of documentation of goals and preferences among patients with advanced cancer. Given that we did not meet our goal of number of conversations, further study is required to identify other barriers to having routine SIC conversations and how to sustain the results from this quality improvement initiative.
Footnotes
Acknowledgments
The authors thank the oncology clinic patients, clinicians, and primary nurses for participating in this project.
Funding Information
This project was funded by a grant by the Chief Medical Officer and Medical Affairs Quality Innovation Fund, Alberta Health Services.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.