
Abstract
Background:
The current cost of treatment of malignant pleural effusion (MPE) with an indwelling pleural catheter (IPC) is unclear.
Objective:
We propose a review of the scientific evidence on the cost and effectiveness of this therapeutic option.
Methods:
Systematic review of the literature on the cost and effectiveness of the treatment of MPE by IPC, according to the PRISMA methodology and quality according to the scientific guidelines.
Results:
A total of 4 articles, 152 patients, and 159 IPCs were included. The use of IPC was associated with improvement in symptoms and quality of life. The most common complications were infections (empyema in 20.9% of patients and cellulitis in 17.3%); 9% of cases were hospitalized due to complications, and <2% required subsequent procedures. The average cost of IPC (set/drainage bottles) ranged from €2,025.6 to €1,200.5 if it was placed on an outpatient basis, €1,100 if survival was <6 weeks, and €4,028 in patients with mesothelioma. Complications increased the cost, and taking into account follow-up visits, additional tests, and days of admission for complications, the cost was >€5,000. Compared with pleurodesis, the cost of IPC was significantly lower when patient survival was <14 weeks, but not when survival was longer or home care was required.
Conclusions:
The use of IPC is associated with good control of MPE and seldom requires many subsequent procedures; however, it is also associated with a certain rate of complications, which may increase costs. However, ambulatory management may help reduce costs, which are directly related to the type of tumor, the duration of survival, and the need for specialized treatment.
Introduction
Malignant pleural effusion (MPE) is a common complication of neoplastic disease, and associated with high morbidity, mortality, and health care costs. Up to 15% of all cancer patients will develop MPE. This incidence is expected to rise as new treatments prolong survival.
The incidence of lung cancer increases in women, and also due to the increasing age of the population.1,2 The main symptoms of MPE are dyspnea, chest pain, and deterioration of the quality of life. Given that MPE is considered as a manifestation of terminal disease, the main goal of treatment is palliative, that is, to control and alleviate secondary symptoms. Pleurodesis used to be recommended as a first-line intervention for the treatment of MPE.
Other approaches such as indwelling pleural catheter (IPC) placement were traditionally reserved for patients ineligible for the former, for example, with trapped lung or in case of failure of pleurodesis.1–3 However, in recent years, a number of randomized clinical trials and high-quality studies have shown IPC to be effective and similar to pleurodesis in terms of symptom control and improvement of the quality of life, and with significant benefits for patients such as ambulatory management and the need for fewer additional pleural procedures.4–6
Recent systematic reviews comparing the effectiveness of IPC versus pleurodesis concluded that the two approaches share a similar success rate for the control of MPE.
IPC is associated with a shorter duration of hospitalization and reduced need for subsequent interventions, but a higher rate of complications, mainly cellulitis, although the difference is not statistically significant.7–10 The latest recommendations for the treatment of MPE therefore position IPC as a first-line treatment for the management of MPE.4–6 The choice between IPC and pleurodesis should be based on the risk/benefit balance in each case and the cost of each procedure.4–6 Cost–effectiveness analyses are an economic evaluation model that provides a framework for comparison of the cost and clinical outcomes of health care interventions.11,12 Although the cost of outpatient management is generally accepted to be lower compared with hospital treatment, the available evidence on the costs of IPC is based on a series of studies with limited caseloads and different designs. Regular drainage involves a significant number of bottles and can increase the use of health care resources, such as the number of medical or nursing visits, as well as indirect costs (derived from lost days of work, missed days of work for family members, etc.). A typical initial IPC drainage frequency might be three times per week, with subsequent adjustment based upon volumes and drainage-associated symptoms. Some centers provide early training to families and patients who then perform drainages at home with a named contact or emergency card in case of difficulty. Others elect to utilize community nursing teams which, while perhaps less flexible than family-led drainage, allows those who do not have family support to have IPCs and provides patients with a more tangible safety net. Despite the evidence supporting the indication of IPC as a first-line treatment for MPE; the current costs of this therapeutic option are unclear. It therefore seemed appropriate to carry out a systematic review of available economic evaluations to assess the cost of this therapeutic option.
Methods
We carried out a search of the literature using the PubMed (Medline) and Embase electronic databases to identify studies analyzing the cost–effectiveness of treating MPE with an IPC.
To obtain the information, we used a predefined search strategy with the following keywords: IPC, costs, effectiveness, efficacy, usefulness, benefit, and MPE. The article search and inclusion protocol followed the PRISMA methodology for conducting systematic reviews. 13
The search period was between January 1st, 2009 and May 1st, 2020. We also performed a manual search of the bibliography of the studies included and relevant reviews for additional studies not returned by electronic literature searches. The search was exhaustive so as not to miss any information relevant to the study objectives: review of the scientific evidence on the cost and effectiveness of this therapeutic option.
The following inclusion criteria were used:
a. In terms of design, we included cohort studies, case–control studies, systematic reviews, and meta-analyses. b. With regard to characteristics, we considered cost–benefit, cost–consequence, cost–opportunity, cost–utility, and cost analysis. c. Regarding the indication of IPC, patients with MPE were included regardless of the etiology. d. Only studies with a sample size of at least 10 IPC-treated patients were included. e. IPC placement was performed according to the standard outpatient procedure unless the patient was hospitalized. f. Only articles in English or Spanish were included.
Studies that met any of the following criteria were excluded:
a. Publications on pleurodesis used in combination with IPC or other intrapleural treatments such as fibrinolytics or chemotherapy.
b. IPC used for the treatment of benign pleural effusion.
c. With respect to the study type, mathematical analyses, and cost evaluations based on mathematical models were excluded.
d. Study information insufficient to establish the quality of the analyses.
Two authors (M.B.-R. and C.R.-H.) independently screened the abstracts to determine the eligibility of the studies, excluding those which did not meet the inclusion criteria. Discrepancies were resolved by third-party arbitration (A.F.-V.). Eligible studies were obtained in full and reviewed independently by two authors (M.B.-R. and C.R.-H.).
Summarizing of the information and cost–effectiveness assessment
The following information was recorded for each of the publications included: clinical–epidemiological characteristics of the patients included in the studies and reason for IPC placement, classified as failure of pleurodesis, trapped lung, as first line, due to severe comorbidity, contralateral IPC, severe respiratory failure, or low life expectancy. To analyze the cost–effectiveness of the treatment, the number of drainage bottles, costs derived from hospitalization or subsequent admissions related to pleural effusion, costs derived from scheduled and unscheduled medical consultations, and/or additional tests were taken into account, and possible indirect costs estimated, for example, based on where the drainage procedure was performed and by whom: in consultation or at home, by a nurse, relative, or the actual patient. Whether the IPC was inserted on an inpatient or outpatient basis was also taken into account. Other main variables recorded included the number of effective spontaneous pleurodesis procedures (defined as removal of the drain without recurrence of MPE), need for subsequent pleural procedures for the control of MPE, reason for IPC removal (including duration of IPC placement), and complications related to the procedure. The outcome of IPC treatment was compared with the standard option, pleurodesis in this case. All costs were expressed in Euros, taking into account the exchange rate in studies conducted in countries with different currencies. With regard to symptoms, the improvement in dyspnea and/or quality of life was taken into account. The relevant information from each study was collected using tables to provide the reader with a simple but global overview of the scientific evidence available on this therapeutic option and its costs.
Assessment of the quality of included studies
The quality of the studies was rated based on the level of evidence and grades of recommendation described in the scientific guidelines, 14 and 27 items of the PRISMA statement were checked for systematic reviews and meta-analyses while writing this article. 13 After reviewing the articles, due to their high heterogeneity it proved impossible to perform a meta-analysis; a qualitative summary of the results was therefore prepared. This article is exempt from IRB approval.
Results
Overview of the studies reviewed
The search returned 29 potentially eligible articles. After excluding 4 articles, 2 for referring to patients with benign pleural effusion and 2 for using a pleural drainage method other than IPC, 25 were retained for reading. Eighteen articles were excluded after reading the abstract, as they were basically reviews of the management of the MPE or reviews in IPC, so that only seven articles were read in full. After careful review of the full text, three studies were excluded on the grounds that they were cost analyses based on mathematical models,11,12,15 so that four articles were ultimately included in the pooled analysis.16–19 Figure 1 shows the study selection flow chart.
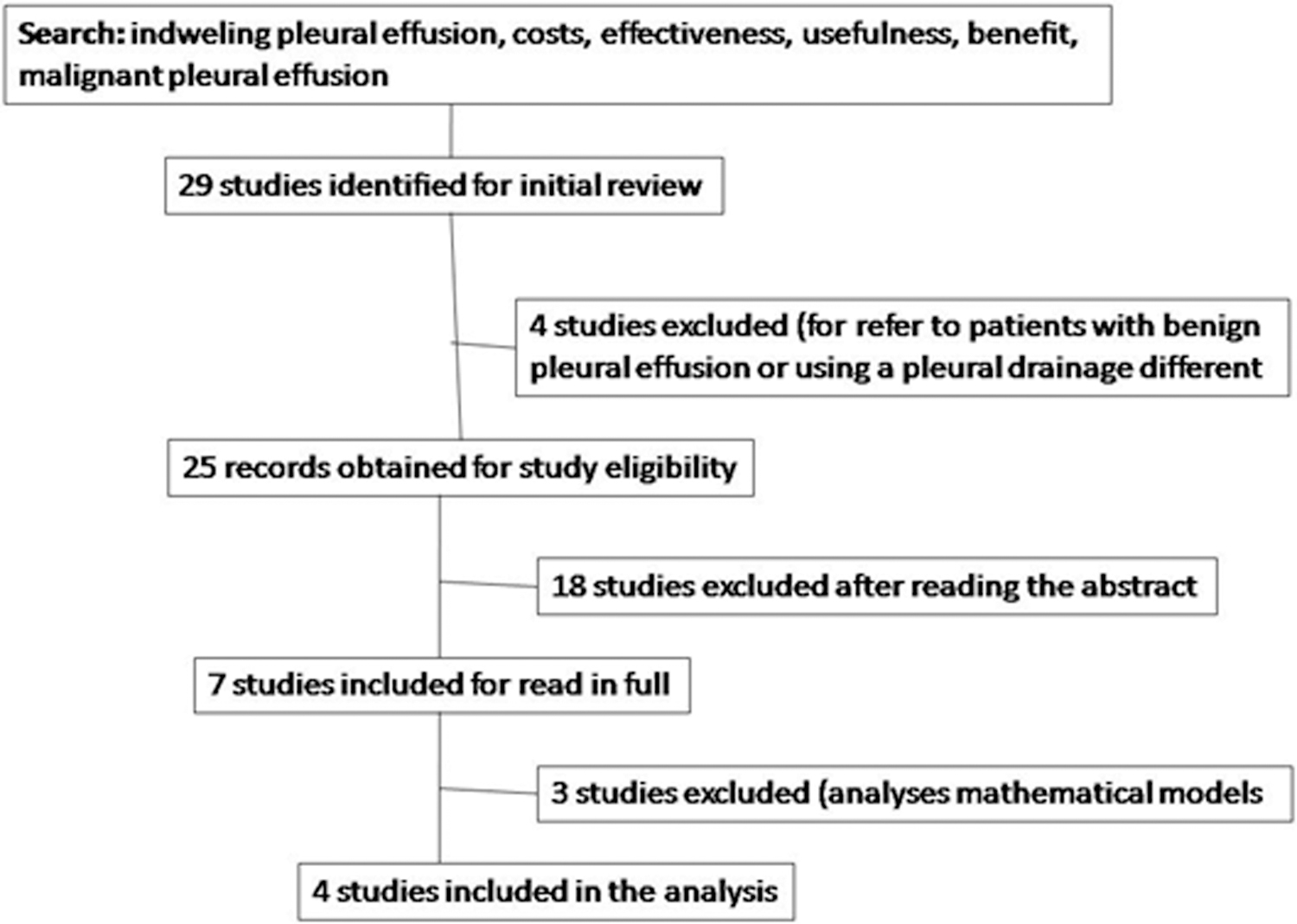
Flowchart of included studies.
Of the four studies that met the inclusion criteria, two were based on a multicenter clinical trial carried out in the United Kingdom (Table 1).18,19
Studies Included in the Analysis
IPC, indwelling pleural catheter.
Patient characteristics
A total of 152 patients were included and 159 IPCs placed. The main indications for IPC placement are described in Table 1. Seventy-three (48%) of the patients were men, with a variable age (range 30–83 years). Lung cancer, which affected 50 (32.9%) patients was the most common cause of MPE (Table 2).
Patients Characteristics
CI, confidence interval; IQR, interquartile range; SD, standard deviation.
Only one study referred to 24 (53.3%) patients being treated for cancer 17 and only the study by Rial et al. 16 mentioned ECOG scale performance status, which was grade 3 (capable of only limited selfcare; confined to bed or chair more than 50% of waking hours) in most cases (30 patients, 54.5%).
Survival was variable (Table 2). Patients with mesothelioma had a survival of 294 days compared with patients with breast or lung cancer, with 58 and 45 days, respectively. 17 Longer survival was also observed in the group that received chemotherapy compared with the group that did not (median survival of 104 days vs. 39 days p = 0.007). 16
Effectiveness of the procedure
Rial et al. reported a median duration of use of IPC after placement of 37 (range: 2–78.5) days. 16 Boshuizen et al. reported a similar duration, noting that the median time from IPC placement to death was similar in the group in which talc pleurodesis had previously been attempted and the group that received IPC as the first-line treatment (43 days vs. 35 days, p = 0.621). 17
Rial et al. described an improvement in dyspnea in more than 87% of patients. 16 Compared with pleurodesis, there were no differences in outcomes related to dyspnea or quality of life.18,19
Of the 66 patients from whom the drain was removed, 57 were due to pleurodesis, but 3 cases experienced a recurrence of MPE and required reintervention. The percentage of effective pleurodesis in the group of patients from whom the drain was removed was 81% (54/66) (Table 3).
Effectiveness of the Procedure: Outcome and Complications
Table 3 details the complications observed and subsequent hospital admissions, mainly for complications. A total of 15/159 (9%) of patients were admitted for complications.
Only 3/159 (1.8%) patients from the TIME2 clinical trial required subsequent pleural procedures: 2 for the placement of other pleural tubes and 1 for pleural effusion drainage by thoracentesis. 7
Costs
Table 4 shows the main findings of the cost analysis. In the study by Boshuizen et al., indirect costs derived from complications, admissions, or the need for home care/drainage were recorded, but not analyzed. Approximately 75% of the patients required no particular home care. 17
Cost of Treatment Malignant Pleural Effusion with indwelling Catheter Pleural
Only cost of catheter kit and drainage bottles.
Cost of the first visit, day-case visit, diagnostic imaging (ultrasound), and complications.
Cost of hospitalization, day-case visit, diagnostic imaging (radiography), and complications.
DND, data not available.
While the mean cost of IPC also differed depending on the type of cancer, being higher in patients with mesothelioma (€4,028 for mesothelioma vs. €1,146 for lung cancer and €2,204 for breast cancer), daily costs did not (total cost/duration of drainage). 17
Significant differences were also observed with regard to total costs and when analyzing the costs derived from complications and tests required during follow-up in the group where IPC placement was performed during hospitalization versus on an outpatient basis. 14
Table 5 compares the cost of IPC versus talc pleurodesis, but only according to studies based on the TIME2 clinical trial.18,19 Compared with chemical pleurodesis, the cost of IPC was significantly lower when patient survival was <14 weeks, but not when survival was longer or nursing care was required.
Discussion
Although it is accepted that the cost of IPC is lower because the procedure does not require hospitalization, our study shows that no conclusive results are available. IPC is associated with good control of MPE and a significant absence of need for subsequent procedures, but with a certain rate of complications requiring hospital admission, implying an increase in costs indirectly related to this treatment option. Although managing MPE on an outpatient basis could reduce treatment costs, these have been found to be directly related to the type of cancer and patient survival when compared with standard pleurodesis.
The study by Boshuizen et al. showed a substantial difference in costs depending on the nature of the primary tumor, ranging from €1,146 for lung cancer to €4,028 for mesothelioma. 17 Mesothelioma is a very aggressive cancer with a poor prognosis compared with other metastatic pleural tumors. The cost of IPC may also be related to the type of cancer treatment received, ECOG scale performance status, or patient comorbidities, but these data were not routinely analyzed.
Although survival varied widely between the studies included in this pooled analysis, when it was <6 or 14 weeks, depending on the study, costs were lower, regardless of the intensity of nursing care required for drainage.17,18
Survival predictions in patients with MPE are changing. Clive et al. recently demonstrated that pleural effusion volume, ECOG grade, pleural fluid lactate dehydrogenase levels, serum neutrophil:lymphocyte ratio, serum NT-proBNP, and MPE type, all affect survival. 20 These findings resulted in the development of the LENT score, a tool which can be very useful to estimate patient survival, and which helps guide decision making when choosing the best available treatment. Proper development and application of prognostic scores is expected to help better personalize treatment decisions.
The only Spanish study published 16 found the cost of outpatient IPC placement to be greater versus inpatient IPC placement, with a higher survival rate. 16 It seems clear that IPC is favored for the treatment of MPE mainly for survival reasons, not because it can be performed on an outpatient basis.
One theory that has been put forward is that the shorter duration of drainage afforded by early pleurodesis may allow the catheter to be removed earlier and reduce the potential costs of outpatient treatment. Pleurodesis can be achieved sooner with more frequent drainage or instillation of talc through a IPC.21,22 A study was recently published which aimed to perform a cost–effectiveness analysis comparing three drainage strategies after IPC placement 23 : symptom-guided drainage, daily drainage, and talc instillation through the IPC. For patients with MPE and an expandable lung, talk instillation through the catheter is the most cost-effective alternative to symptom-guided drainage. Daily drainage through an IPC is not a cost-effective strategy. 23
A recent systematic review, 10 which included 5 randomized clinical trials with a total of 545 patients compared the efficacy of IPC versus chemical pleurodesis for the control of MPE. Comparison of chemical pleurodesis or IPC found the latter to be associated with shorter hospital stays and a lower requirement for subsequent pleural procedures, but with a higher rate of minor complications. The authors themselves recommended assessing patients on a case-by-case basis, taking into account their preferences and costs when deciding between IPC and pleurodesis. The analysis published this year in the Cochrane review came to the same conclusion. 6
While complications represent an increase in cost, they occurred in a total of 30% of treated patients, only 9% of whom required inpatient hospital treatment.
Studies based on mathematical models were excluded from this review; however, analysis of these studies yielded conclusions similar to ours. Since IPC is more cost effective than chemical pleurodesis through a chest tube, it would appear to be the best option for patients with MPE and low life expectancy.11,12 Compared with repeated thoracentesis, it is the least effective option. 15
This study has limitations. This systematic review included only published evidence on cost–effectiveness not directly based on mathematical models, with a small number of studies. The studies reviewed were not homogeneous; indeed, depending on the design, they included the direct cost of medical care, medical consultations, drugs, surgery, hospitalization, and diagnostic tests. The economic implications of IPC treatment may therefore not be altogether accurate, and while outpatient management is generally accepted to cost less than hospital management, other than retrospective studies and mathematical models, there are no definitive studies of the cost–effectiveness of IPC. What does seem clear is that IPC treatment is more cost effective in patients with an expected survival of <14 weeks, particularly when no outpatient nursing care or visits are required. Another limitation could be that the results of cost–effectiveness studies may not be applicable to all clinical pictures.
The results of this review could have an impact in the future, and although the latest recommendations describe IPC treatment as cost effective, large randomized studies appear necessary to confirm these findings. Patient preferences and the financial impact of the choice of treatment must be considered when making a choice between IPC or pleurodesis.
Conclusions
The use of IPC is associated with good control of MPE and seldom requires many subsequent procedures; however, it is also associated with a certain rate of complications, which may increase costs. While ambulatory management may help reduce costs, these are directly related to the type of tumor, the duration of survival, and the need for specialized treatment.
Footnotes
Authors' Contributions
Conception and design: M.B.-R., C.R.-H. Administrative support: V.L.-F., A.F.-V. Provision of study materials or patients: M.B.-R., C.R.-H., I.L.-R., C.R.-R. Collection and assembly of data: M.B.-R., C.R.-H., I.L.-R., C.R.-R. Data analysis and interpretation: M.B.-R., C.R.-H., A.R.-R. Article writing: All authors. Final approval of article: All authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.