
Abstract
Background:
Physicians' estimate of life expectancy in patients with spine metastasis frequently impacts treatment decisions regarding surgery, radiation techniques, dose, and fractionation.
Objective:
We aimed to identify predictors of survival and generate a stratification schema that could guide clinical decision making.
Materials and Methods:
We identified 269 patients who have undergone surgery and/or radiation for spine metastasis from 2002 to 2013 at an academic medical institution in the United States. A univariate survival analysis was carried out using the Kaplan–Meier method. Differences in survival by histology were assessed using the log-rank test. Multivariate analysis was performed using the Cox proportional hazards model, then using the same variables, recursive partitioning analysis (RPA) was conducted to determine risk groups associated with survival.
Results:
The median overall survival was 4.76 months. Twenty percent, 40%, and 57% of patients died within one, three, and six months of radiation treatment, respectively. RPA analysis resulted in three classes; class I included patients with Karnofsky Performance Status (KPS) ≥80. Class II included patients with KPS <80 and radioresistant or favorable histologies. Class III included all other histologies. Median survival in months was 11.4, 6.3, and 2.0, respectively.
Conclusion:
We developed a stratification schema predictive of survival in patients with spine metastasis. This RPA classification should be validated in independent patient populations from several institutions and may ultimately identify patients who are good candidates for more complex treatment regimens, such as stereotactic body radiotherapy.
Introduction
In patients with cancer, the incidence of spinal metastases is ∼30% at autopsy and ∼10%–30% of new cancer diagnoses per year present with spine metastases.1,2 These metastases can be a source of significant pain, neurological compromise, and overall diminished quality of life. The mainstays of treatment for spinal metastases include surgery and radiotherapy (RT). 2 Stereotactic body radiation therapy (SBRT) is a modality that can provide significant relief with fewer side effects than traditional radiation. To identify patients who would benefit the most from SBRT, we sought to first identify prognostic factors and through recursive partitioning analysis (RPA) develop a stratification schema to aid clinicians in clinical decision making.
Materials and Methods
We retrospectively reviewed consecutive patients who have undergone surgery and/or radiation for spine metastasis from 2002 to 2013 at our institution. Exclusion criteria were subjects with primary spine tumors, multiple myeloma, lymphoma, and germ cell tumors. A total of 269 patients were included in this study.
A retrospective chart review was conducted, from which details were extracted from the electronic medical record (EMR). The following variables were collected: age, gender, vital status, histology, Karnofsky Performance Status (KPS) at time of diagnosis, number of vertebral bodies involved at time of diagnosis, epidural involvement, additional metastases other than spine, stability of systemic disease, whether or not RT and/or surgery was performed, dose, fraction, time from diagnosis to RT, time to RT completion, time interval from diagnosis to RT, and whether patient received repeat RT or RT at various vertebral levels on separate occasions. This retrospective review was approved by institutional review board (IRB).
Survival curves were generated using the Kaplan–Meier method. Differences in survival by histology and by time between diagnosis and metastases were assessed using the log-rank test. RPA was then performed to identify any association of the following variables with overall survival (OS) after RT: histology, gender, age, KPS, control of systemic, extraosseous metastases, time from primary diagnosis (TPD), extent of spine disease, epidural only, bone and epidural, and bone only. RPA was performed using the Classification and Regression Trees (CART) software. Kaplan–Meier curves were generated based on the risk groups. Finally, multivariate analysis was performed using the Cox proportional hazards model using all the variables selected for RPA.
Results
Of the cohort of 269 patients, 70 (26%) were female and 199 (74%) were male, as described in Table 1. Fifty-six (21%) patients underwent surgery and 213 (79%) did not. Six (2%) patients did not receive RT and the remaining 263 (98%) did. Among the 263 patients, 257 (98%) completed treatment and 6 (2%) did not. The median age at the beginning of RT was 63 years (range 19–94), median radiation dose was 30.0 Gy (range 3–60), median survival time 4.76 months, and median follow-up time was 4.6 months. Median KPS at initiation of RT was 70 with 86 patients (32%) having a KPS <70. At time of analysis, 30 patients (11%) were living and 239 (89%) were deceased.
Demographics and Clinical Characteristics of Patients
Radioresistant histologies include renal cell, melanoma, and sarcoma.
Other histologies include adrenal, bladder, bone, brain, colon, esophageal, gallbladder, liver, lung, squamous cell carcinomas, neuroendocrine, ovarian, pancreatic, gastric, thyroid, uterine.
Favorable histologies are defined as breast and prostate.
Including visceral, brain, and bone metastases other than in the spine.
KPS, Karnofsky Performance Status.
In regard to histology, 90 (33%) were considered to be favorable (breast and prostate) and 30 (11%) were radioresistant (renal cell, melanoma, and sarcoma) compared with all other histologies, 149 (55%).
A total dose of 30 Gy over 10 fractions was the most common radiation regimen, received by 111 patients (42%). Of remaining patients who received radiation 106 (40%) received <30 total Gy, and 41 (16%) received >30 Gy.
The median OS from completion of RT was 4.9 months. Patients who died within one, three, and six months of treatment completion were 20%, 40%, and 57%, respectively. The one- and two-year OS were 32% and 19%. Kaplan–Meier curves by histology (Fig. 1) show median OS for breast and prostate histologies as 8.9 months, melanoma, renal cell and sarcoma as 7.7 months and 2.7 months for all other histologies (p = 0.0007). In regard to TPD to metastases, those who were diagnosed with metastases more than one year later had the greatest median OS of 5.6 months, followed by diagnosis 6–12 months later with a median OS of 3.3 months (Fig. 2). Median OS for patients presenting with metastases or diagnosis of metastases <6 months was 2.8 months.
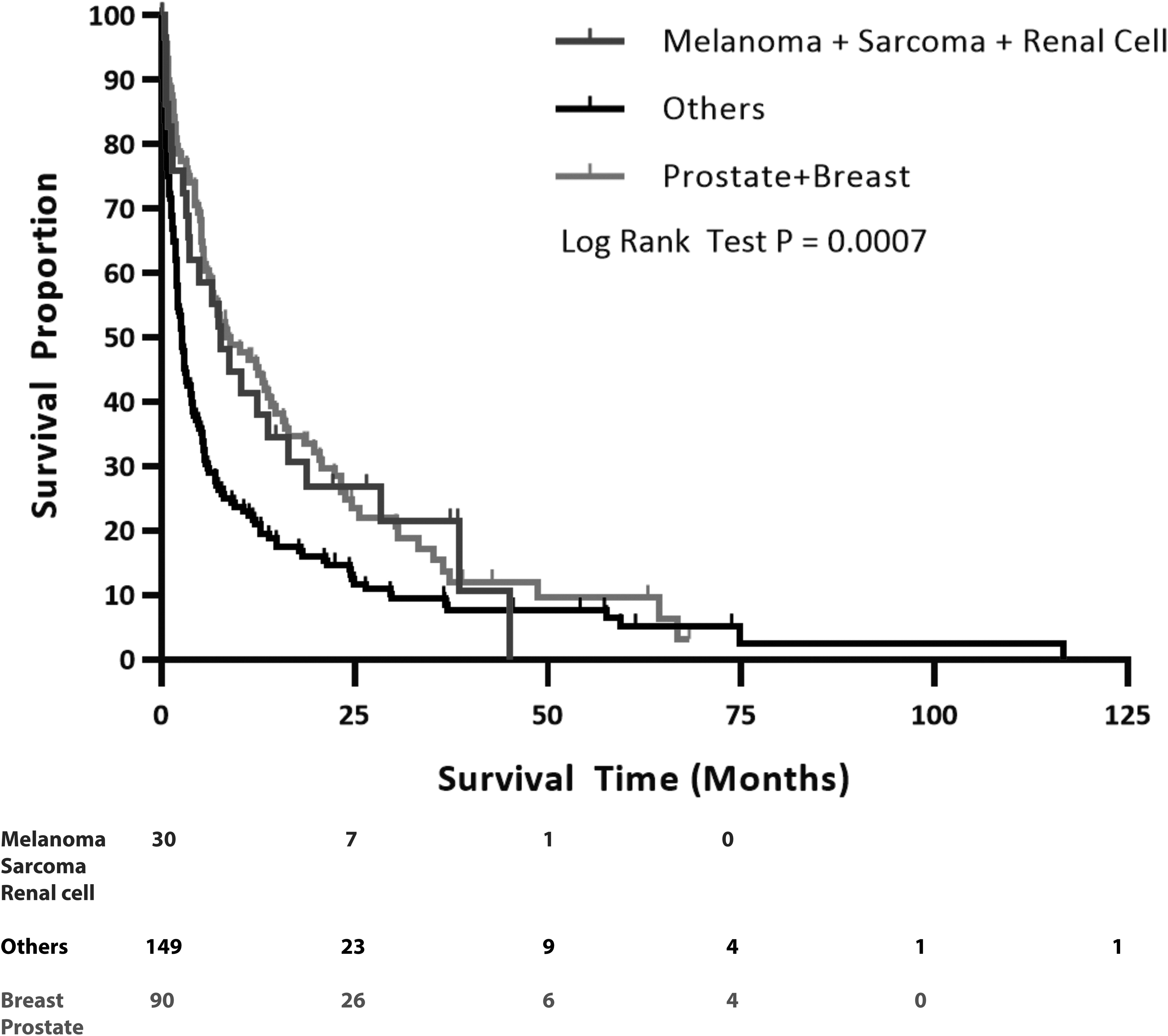
Kaplan–Meier curve of OS by histology. Median OS for favorable histologies (prostate and breast) was 8.9, 7.7 months for radioresistant (melanoma, sarcoma, and renal cell), and 2.7 months for all other histologies (p = 0.0007). OS, overall survival.
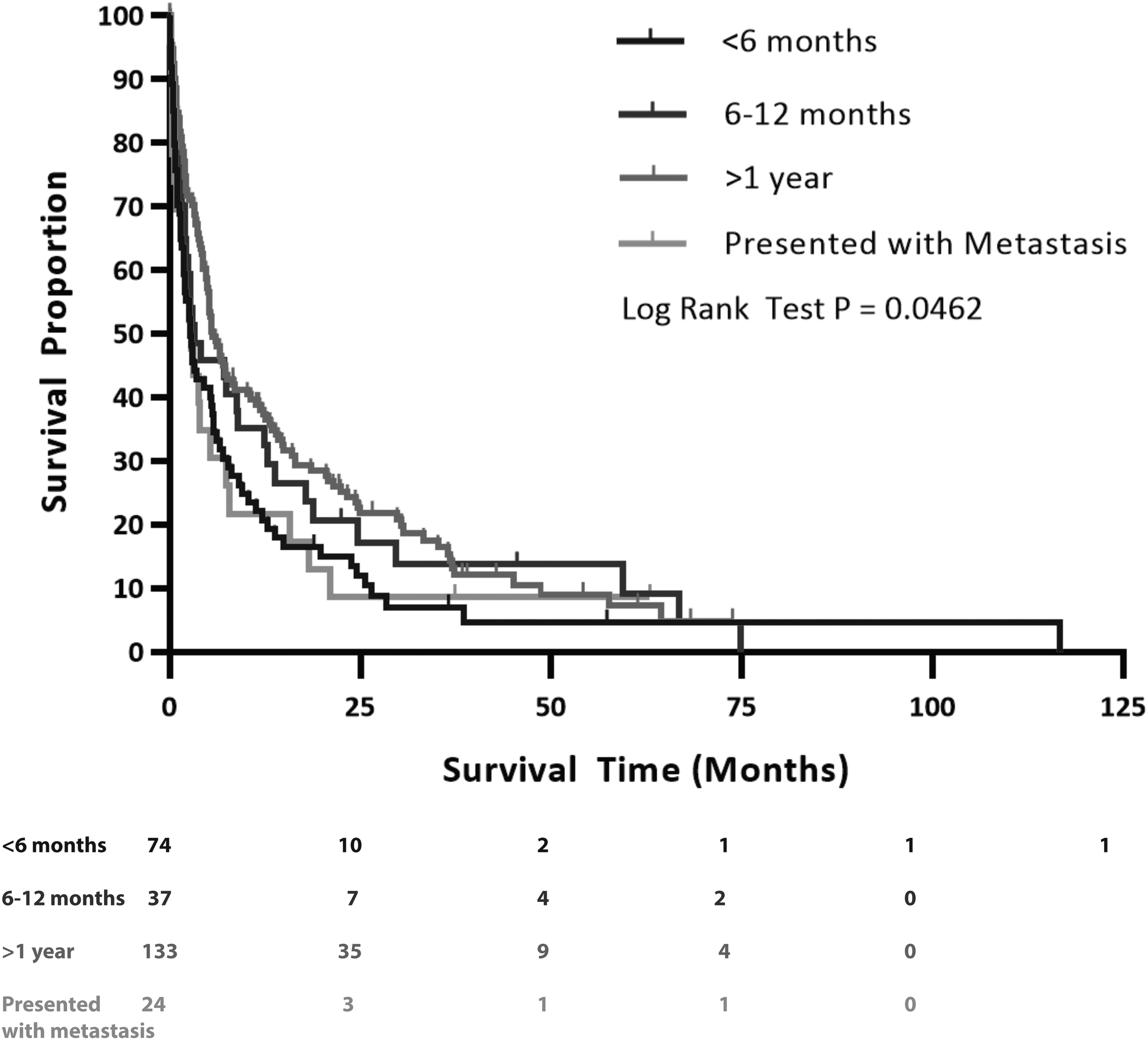
Kaplan–Meier curve of OS by time between primary diagnosis and diagnosis of spine metastases. Median survival time for those who presented with spine metastases was 2.8 months, metastases at <6 months was 2.8 months, metastases at 6–12 months was 3.3 months, and diagnosis of metastases at >1 year was 5.6 months (p = 0.0462).
RPA resulted in three distinct classes (Fig. 3) with significantly different survival curves (p < 0.0001, Fig. 4). The greatest median OS was associated with Class I at 11.4 months (range 0.03–116.70 months) and was defined as KPS ≥80. Patients with KPS <80 were classified based on histology. Class II included individuals with favorable or radioresistant histologies; median OS was 6.3 months (range 0.07–66.80 months). Class III was defined as having a histology other than favorable or radioresistant and median OS was 1.95 months (range 0.10–29.60 months).

RPA resulted in a tree with three classifications. Class I included patients with KPS ≥80. Patients with KPS <80 were classified based on histology. Class II included radioresistant and favorable histologies and all other histologies in class III. ‡Radioresistant histologies include renal cell, melanoma, and sarcoma. *Favorable histologies are defined as breast and prostate. †Other histologies include adrenal, bladder, bone, brain, colon, esophageal, gallbladder, liver, lung, squamous cell carcinomas, neuroendocrine, ovarian, pancreatic, gastric, thyroid, and uterine. KPS, Karnofsky Performance Status; RPA, recursive partitioning analysis.
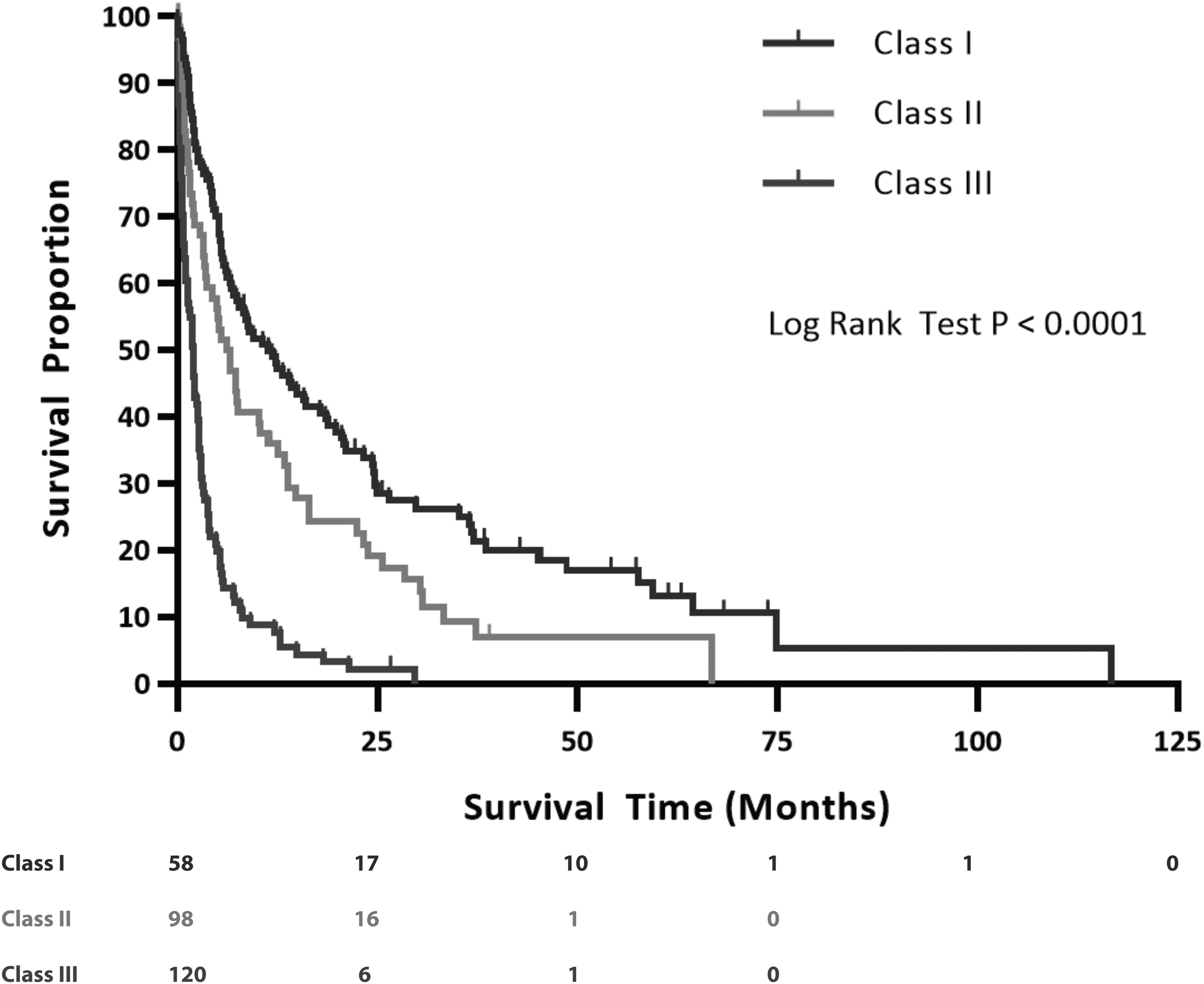
Kaplan–Meier survival curve based off of classes from RPA classification tree. Median survival time for Class I was 11.4 months, for Class II was 6.3 months, and for Class III was 1.95 months (p < 0.0001).
Multivariate analysis showed that KPS at time of RT (≥70 vs. <70; hazard ratio [HR] = 0.50, 95% confidence interval [CI] = 0.37–0.67, p < 0.001), histology (all other histologies vs. favorable, HR = 1.64, 95% CI = 1.20–2.24, p = 0.002) and stability of overall systemic disease at time of spine metastasis diagnosis (stable vs. unstable, HR = 0.54, 95% CI = 0.38–0.77, p < 0.001) were strongly associated with improved OS (Table 2). Age was borderline significant (HR = 0.68, p = 0.0479, 95% CI 0.47–1.0). Other factors, including gender, epidural involvement, number of vertebral bodies affected, and time between primary diagnosis and diagnosis of spine metastasis, were not predictive of survival.
Multivariate Cox Regression Analysis for Overall Survival (n = 269)
Radioresistant histologies include renal cell, melanoma, and sarcoma.
Favorable histologies are defined as breast and prostate.
Other histologies include adrenal, bladder, bone, brain, colon, esophageal, gallbladder, liver, lung, squamous cell carcinomas, neuroendocrine, ovarian, pancreatic, gastric, thyroid, and uterine.
N/A; VB, vertebral bodies.
Discussion
In our retrospective cohort study, we found that the factors most strongly associated with OS in patients undergoing RT for spine metastases were KPS, histology, and systemic disease stability. RPA resulted in three distinct classes: Class I with KPS ≥80, Class II with KPS <80 and favorable or radioresistant histologies, and Class III with KPS <80 and histologies other than favorable or radioresistant.
It has been well demonstrated that SBRT provides high rates of tumor control, regardless of the underlying primary histology, whereas sparing normal tissues, such as the spinal cord.3–7 Stereotactic radiation technology has been used for decades to treat brain tumors. In the past decade, it has become increasingly used in the treatment of extracranial tumors. This method of radiation provides a high level of target accuracy with minimal exposure to surrounding normal tissues 8 ; however, SBRT requires more time for planning, more personnel, and advanced technological resources than other forms of radiation therapy. When evaluating patients for candidacy for this modality of RT, we recommend triage based on the earlier outlined schema, weighing functional status/KPS as the most important prognostic factor. Primary tumor histology can be used for further prioritization with clinical judgment, as needed.
Many studies have evaluated prognostic factors for patients with metastases to the spine. In 1990, Tokuhashi et al. developed an assessment system of prognostication for patients with metastatic spinal tumors based on a review of 64 surgical cases. 9 Parameters evaluated included general condition, primary disease, extraspinal bone and major visceral metastases, extent of vertebral body involvement, and severity of cord palsy. The authors concluded that no one single parameter could predict prognosis, but when evaluated together, these factors could be used to guide treatment; however, in further evaluation, the authors found the predictability was only 63% in a study of 128 patients and they went on to describe a revised score system that takes KPS into account.10,11 The revised Tokuhashi et al. prognostic system focuses largely on triaging conservative versus surgical management of spinal metastases as do other similar scoring systems, including those by Tomita et al. and Bauer and Wedin.12,13 Similarly, the Spinal Instability Neoplastic Score (SINS) is a validated tool developed by Fisher et al. for identification of instability that may benefit from surgical management.14,15 Our prognostication model targets patients who have already been deemed suitable candidates for radiation. It has the advantage of a larger number of patients evaluated retrospectively and is overall more easily applied clinically.
In addition to prognostication for spinal metastases, schemas have similarly been developed for brain metastases. Gaspar et al. found that KPS and primary tumor control best predicted survival in their population, which included >1000 patients retrospectively reviewed. 16 In a smaller study of 181 patients, Combs et al. found KPS and primary diagnosis to be most predictive of prognosis in patient underdoing adjuvant radiation after surgical resection. 17
Previous studies have demonstrated RPA to be predictive of OS in patients receiving RT for metastatic disease16–19 ; however, these studies have focused on treatment of brain metastases, triaging surgical versus conservative management of spinal disease, or the use of SBRT as the only radiation modality. To our knowledge, our study is the first to use RPA to evaluate OS in patient received RT for metastatic disease to the spine.
Our study, as well as other literature, has consistently found KPS to be a significant prognostic factor, specifically when KPS is ≥70.16–18,20 Although age in our study was borderline significant, Chao et al. and Gaspar et al. demonstrated it to be prognostic.16,18 Gaspar et al. and Combs et al. also found histology to be strongly associated with OS, 17 although our classification of histologies into favorable, radioresistant, and other histologies provides additional insight for clinicians. Study by Gaspar et al. demonstrated that control of the primary tumor with the brain as the only site of metastases to be prognostic 16 ; we did not find the presence of other metastases to be significant, although stability of systemic disease was predictive of OS. We did not find that the TPD to be predictive of OS, which is inconsistent with other studies in the literature.16–18 It is possible that if this variable was a continuous variable in our analysis that our results would have been more consistent with the literature; however, our categorization of TPD into groups of six-month intervals was a limitation of our dataset.
Although our study demonstrated consistent findings with the literature, it is not without limitations. As a retrospective study, we were limited by the information available in our EMR. We used KPS to describe functional status; however, this does not directly address ambulatory status or SINS, as this information was not consistently available in EMR review. We were unable to control for potential confounders such as systemic treatment options and targeted therapy. During the years reviewed (2002–2013), there have been dramatic advances in the treatment of lung, kidney, prostate, and other cancers. For example, advances in immunotherapy, particularly for the treatment of melanoma, have advanced dramatically in recent years.21,22 Although overall the sample size in our study is a strength, the sample size of radioresistant histologies (renal cell, melanoma, and sarcoma) is small (n = 30), which may have influenced why radioresistant histologies appeared to do well. However, the term “radioresistant” is historic and with the advent of SBRT, tumors that were previously resistant to the standard low dose per fraction, are sensitive to radiation given in higher doses per fraction. Thus, better survival seen in the “radioresistant” group is likely associated with significantly improved systemic therapy.21,22 In addition, the survival ranges of the classes are somewhat large with a small overlap of the poorest survival times of class I and class II. Finally, because this is a single institution study, it may not be generalizable to other populations. Despite these limitations, our study contributes to the literature regarding clinical management of spine metastases and may aid physicians in identifying patients who may be suitable candidates for SBRT.
Future research should seek to have a larger dataset that not only incorporates histology, but also systemic therapy options and personalized medicine data, such as molecular genomics, to guide clinical decision making. Also, the inclusion of data from multiple institutions will help to improve generalizability to various populations.
Conclusion
We developed a stratification schema predictive of survival in patients with spine metastasis who receive radiation therapy. Patients with the best outcomes had a KPS ≥80 and should be considered good candidates for more complex treatment regimens, such as SBRT.
Footnotes
Authors' Contributions
The authors certify that each author meets the criteria for authorship as defined by the International Committee of Medical Journal Editor.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.