
Abstract
Introduction:
The emergency department (ED) is a primary entry point of hospitals but does not have a system to identify and consult palliative care (PC) early in patients who meet criteria.
Objectives:
To determine the measurable effects of an ED PC consultation on patients who meet criteria, hypothesizing that ED PC consultation would lead to decreased average length of stay (ALOS), average direct cost per patient, decreased number of surgeries, and radiological tests performed per patient.
Materials and Methods:
A physician-led data-driven evidence-based algorithm was designed and piloted with implementation in two hospitals during January–March 2019 in Orlando, FL. A retrospective review of health record data was completed, comparing patients receiving PC consultation ordered in the ED versus those ordered after admission.
Results:
ED patients (n = 662) met PC criteria. PC consultation was ordered in ED for 80 (12.1%) cases. The following outcomes were lower for patients who received ED PC consultation than those who did not: ALOS by 6.4 days (6.74 vs. 13.14 days; p < 0.001), in-hospital mortality (12.5% vs. 19.1%; p = 0.11), surgery (11% vs. 37%; p < 0.01), radiological tests per patient (4.01 vs. 10.57; p < 0.001), and average direct cost per patient ($7,193 vs. $22,354). However, 30-day hospital revisit rates were relatively higher in those who did receive ED PC consultation than those who did not (20% vs. 13% p = 0.15).
Conclusions:
In this pilot project, PC patients can be identified in the ED with an algorithm that leads to earlier consultation and improved patient outcomes. Larger research trials are needed to replicate this strategy and results.
Introduction
Though the fundamentals of emergency medicine (EM) focus on the diagnosis and care of acute medical conditions, the emergency department (ED) serves as a hub for both acutely and chronically ill patients. Among those with chronic conditions, patients with a variety of advanced diseases frequently present to the ED, many of whom may benefit from early involvement of palliative care (PC). In addition, many patients with incurable worsening diseases fail to receive early in-hospital PC,1,2 and because of the nature of their complex medical conditions, they can often fall victim to lengthy hospital stays and high hospital costs.
A sector of those involved in EM education has already attempted to improve early recognition of ED PC with part of the American College of Emergency Physicians (ACEP)'s 2013 “Choosing Wisely Campaign” emphasizing the importance of early intervention of palliative and hospice services to patients with “chronic and/or incurable diseases”. 3 Some training programs have also introduced simulation-based PC education into resident training to increase awareness. 4 Early identification and palliative medicine consultation have been shown to lead to better overall collaborative care of these patients with studies suggesting that when an emergency clinician initiates a palliative medicine consultation in the ED, patients benefit from a decreased hospital average length of stay (ALOS)5–9 as well as a higher degree of hospice utilization. 8
In addition, studies have also shown a general relationship between early involvement of palliative services being associated with a decrease in both costs of care10–12 and intensive care utilization. 12 Not only do ED PC consultations potentially decrease overly aggressive futile care during the proximate subsequent days, they also improve the likelihood that care will be optimized to the patients' and family members' preferences and advanced directives.13,14
Approximately 5000 patients present to AdventHealth coded with International Classification of Diseases 10 code Z51.5 (encounter for PC) each year with 4000 of these patients being seen in the ED. Of those patients, ∼77% are on Medicare or Medicaid. The 2015 Pepper Institute on Aging and Public Policy predicts that by the year 2030, 27% of the state population will be over the age of 65 years. Also, the number of those above the age of 85 years is predicted to increase from 5.9 million in the year 2012 to 18.2 million in the year 2030. 15 These statistics suggest that the number of patients who meet PC criteria will likely increase as well.
Since the ED is the primary entry point of care within the system, it is vital that patients are targeted to the correct floors, units, and health care services.
At AdventHealth, a group of strategic pathways termed AdventHealth Clinical Transformation (ACT) are designed and piloted to assist ED providers in identifying placement for patients to receive best care in the hospital. As PC is a new service in the hospital, an ACT was created to assist providers on how to best use PC services. Without this pathway, there is no existing objective system in place to identify palliative patients, often leading to a delay in consultation due to the decisions being left to the individual providers' clinical judgment. In this study, we seek to show that ACT can lead to ED initiation of PC consults with multiple potential benefits. Implementing a formal system to increase awareness would likely be beneficial in EDs across the country since it is well known that ED physicians often fail to involve palliative services early in patients' hospital stays.1,5,7,13
Materials and Methods
Study design and setting
A multidisciplinary team of EM physicians, PC physicians, nursing leadership, and other support staff from the Clinical Innovation Department was formed to design and develop the ACT pathway. After a thorough review of current state and organizational values, an algorithm detailing the consensus-backed “standard of care” was drafted and implemented in two major sites of AdventHealth (Fig. 1).
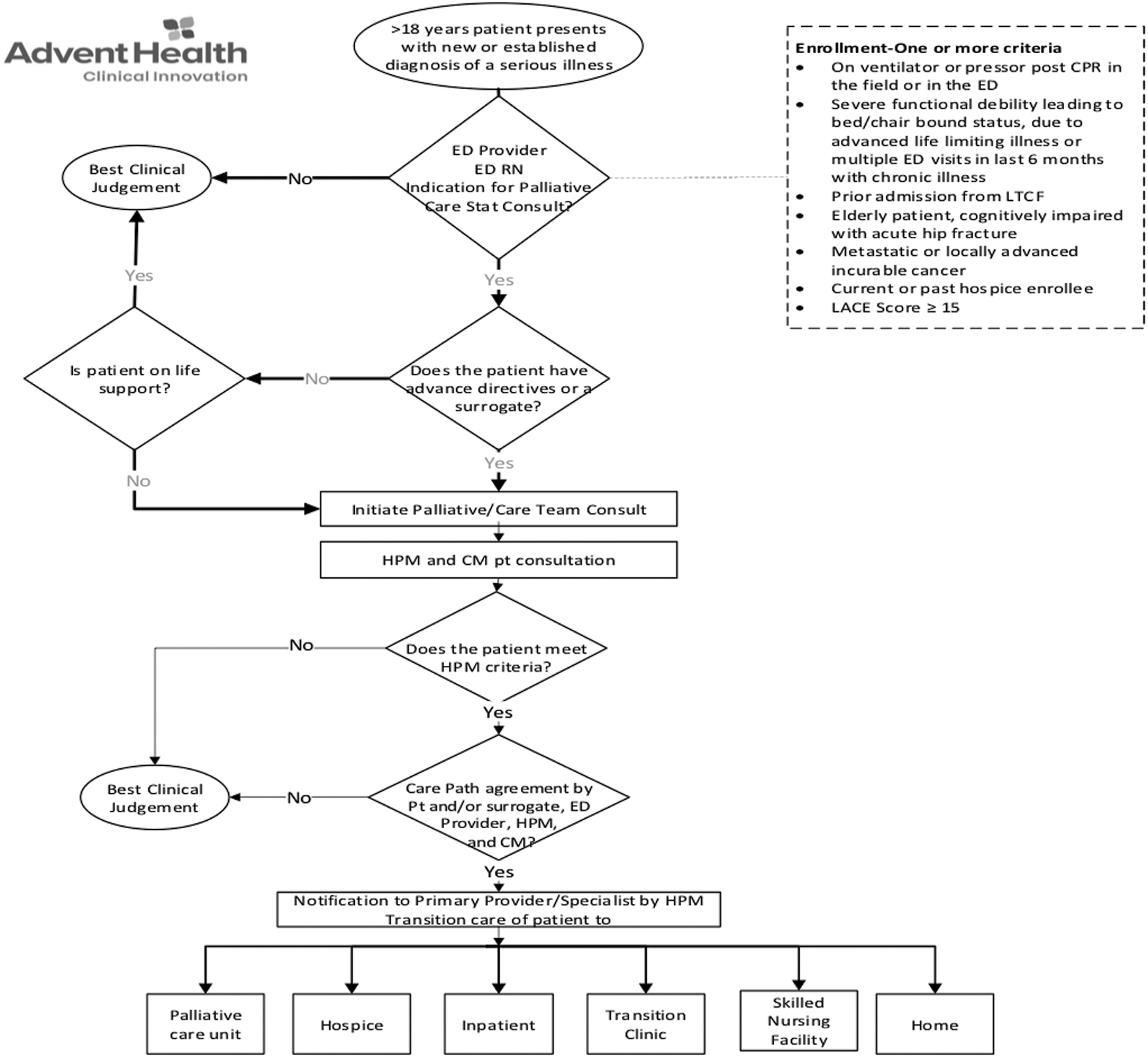
ED PC pathway. ALOS, average length of stay; Avg, average; CM, care management; ED, emergency department; CPR, cardiopulmonary resuscitation; HOC, hospice of the comforter; HPM, hospice palliative medicine; IP, inpatient; LACE, length of stay, acuity, comorbidities, ER visits; LTCF, long-term care facility; Obs, observation; PC, palliative care; Pt, patient; RN, registered nurse.
Ethics approval
This study is classified as quality improvement, which is allowed by our institutional review board (IRB), and no patient consent was required.
Study algorithm and patient selection
Elements in the algorithm include (Fig. 1) Identification: Early identification of adult patients presenting to the ED with a new or established diagnosis of a serious illness or life-limiting disease; Indication: Best clinical judgment by the provider when given the following enrollment criteria: on a ventilator or pressor postcardiopulmonary resuscitation in the field or in the ED, severe functional debility leading to bed/chair bound status due to advanced life-limiting illness, multiple ED visits within six months due to chronic illness, prior admission from a long-term care facility, elderly patient cognitively impaired with acute hip fracture, metastatic or locally advanced incurable cancer, current or past hospice enrollee, or LACE (length of stay, acuity, comorbidities, ER visits) score ≥15; Stratification: If the patient met the criteria and/or maintained documented advanced directives, the patient was eligible for PC enrollment from the ED; Action: Recommend initiating PC consult order in the ED.
A pilot study of the clinical pathway was conducted between a three-month period of January 2019 through March 2019 aimed at evaluating the efficacy of early initiation of PC consult orders in the ED. Data were collected from two different EDs: a large tertiary care center in downtown Orlando, FL, with an approximate volume of ∼100,000 patients per year, and a smaller community hospital in Winter Park, FL, with an approximate yearly volume of ∼37,000 patients.
To educate ED providers and nursing staff about the logistics of this pilot project, the ACT team met on multiple occasions at formal ED meetings before the initiation. During the three-month period, ACT members would visit the ED in real time to reiterate study objectives, as well as answer questions regarding the pilot study.
After the three-month period, retrospective chart reviews were conducted by the ACT team on each patient who had a PC consult ordered in the ED during that period. Extensive review and consideration were given for analyzing patient demographics for the following: age, gender, marital status, ethnicity, ALOS, reason for visit, principal diagnosis, time until palliative consult, hospice order, number of procedures, radiology studies ordered, and 30-day revisit rates. The primary endpoint was a comparison of outcomes between those patients who received an ED PC consultation order with those who received a PC consultation order after inpatient admission. The palliative team met with the patient and family either in the ED or after hospital admission based on their schedule.
Outcome measures and data analyses
Data were extracted from the electronic health record using PowerInsight (Business Objects). The population criteria included adult patients presenting to the ED who had a PC consult ordered during their stay. Procedural direct cost data were received from AdventHealth's Financial Planning Department. Cost data reflect average figures and were extrapolated to reflect average direct costs per patient. We performed statistical tests using the “Two Proportions” method, and the p-values were calculated using two-sample t-tests through Minitab. p-Values of <0.05 were considered statistically significant.
Results
Characteristics of the study subjects and main results
A total of 662 ED patients who met the PC criteria were analyzed at two EDs of our AdventHealth system. An ED PC consultation was ordered in 80 of the 662 patients (12.1%) with similar demographic distribution and percentage of patients with an oncological diagnosis between patients who received PC consults within and outside of the ED (Tables 1–3). As given in Table 4, when comparing patients who received the ED PC consultation order with those who did not, ALOS was decreased by 6.4 days (6.74 vs. 13.14 days, respectively; p < 0.001).
Demographics of Patients with Palliative Care Ordered in the Emergency Department
ED, emergency department; PC, palliative care.
Demographics of Patients with Palliative Care Ordered Outside the Emergency Department
Percentage of Patients with Palliative Care Order Placed in Emergency Department versus after Admission with an Oncological Diagnosis
Outcomes of Palliative Care Order Placed in the Emergency Department versus after Admission
ALOS, average length of stay; Avg, average; IP, inpatient; Obs, observation; Pt, patient.
Patients who received an ED PC consultation order also saw decreases in the following secondary outcomes: in-hospital mortality rate (12.5% vs. 19.1%; p = 0.11), surgeries (11% vs. 37%; p < 0.01), radiological tests per patient (4.01 vs. 10.57; p < 0.001, Table 4, Fig. 2), and average direct cost per patient ($7,193 vs. $22,354, Fig. 3). However, 30-day hospital revisit rates were relatively higher in those who did receive ED PC consultation versus those who did not (20% vs. 13% p = 0.15), though with a p-value of 0.15 this may not be statistically significant (Table 4).
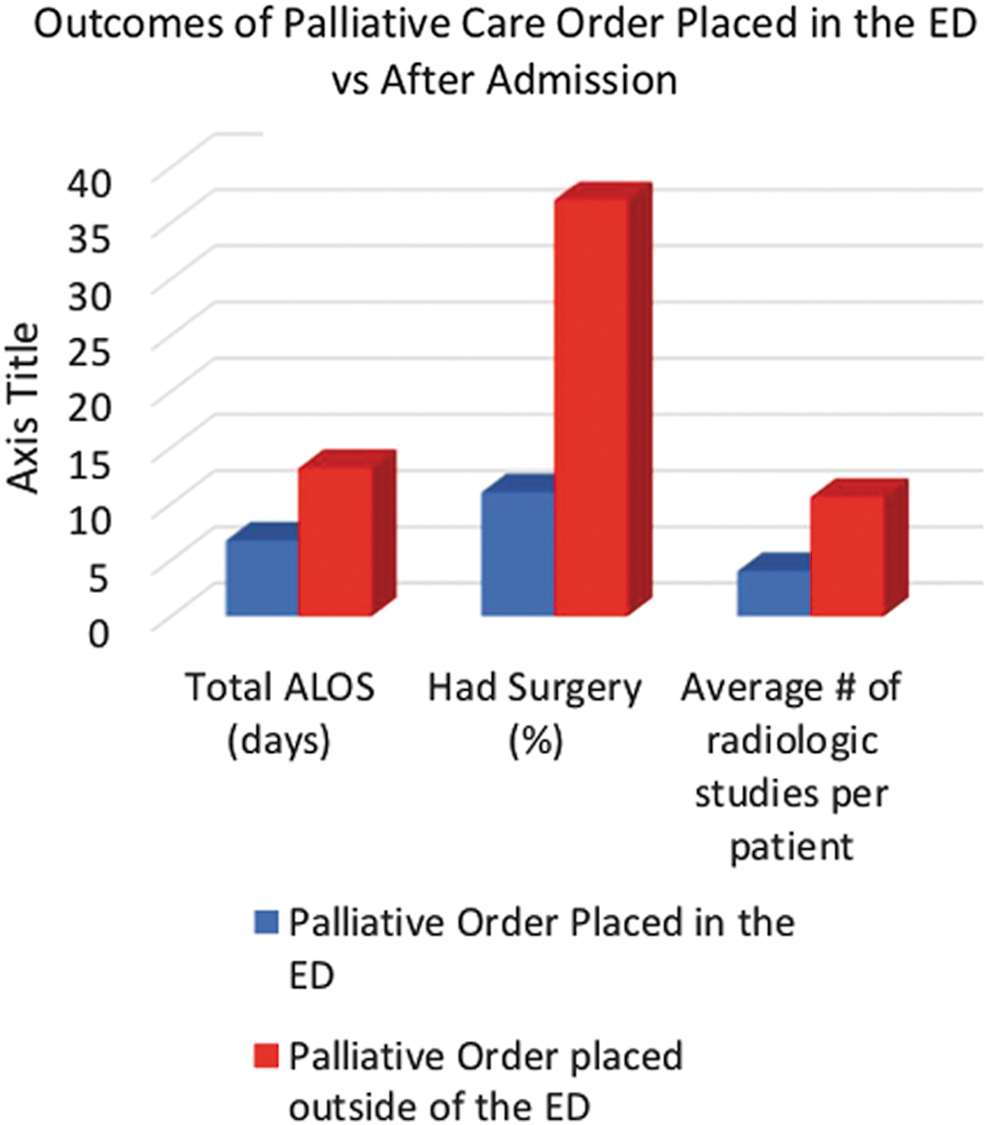
Outcomes of PC order placed in the ED versus after admission. Color image is available online.
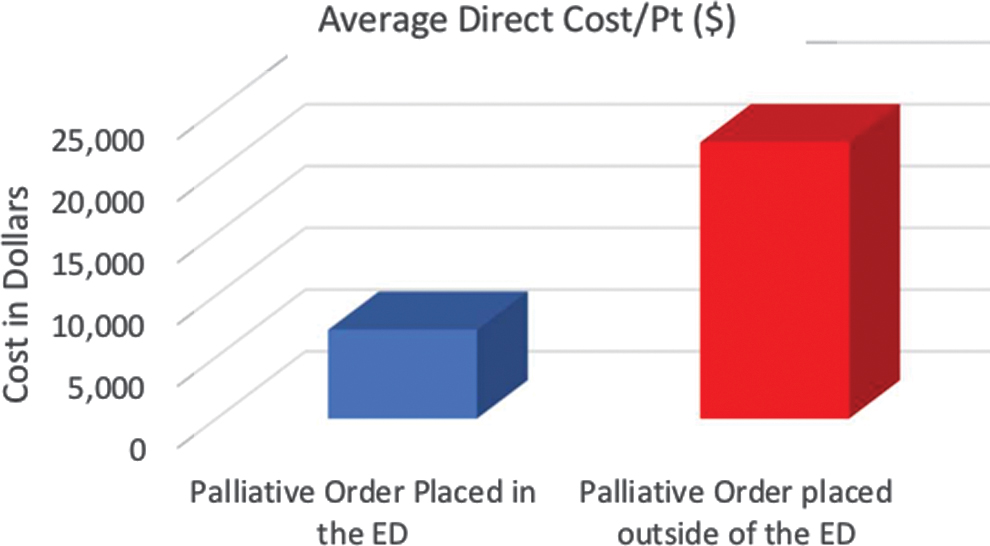
Average direct cost per patient of patients with PC order placed in the ED versus after admission. Color image is available online.
Table 5 summarizes similar results within the subgroup analysis. Overall, within all subgroups, patients who received an ED PC consult showed decreased ALOS, underwent fewer surgical procedures, and had decreased cost associated with their hospital admission. Patients with an oncological diagnosis (ALOS 7.65 vs. 13.18, surgeries 11% vs. 37%, costs $8,339 vs. $17,649): patients with a LACE score ≥15 (ALOS 4.32 vs. 14.28, surgeries 23% vs. 42%, costs $3,519 vs. $17,921): patients from a long-term care facility (ALOS 4.98 vs. 11.82, surgeries 0% vs. 34%, costs $4,566 vs. $30,147), and patients with greater than two ED visits in the past six months (ALOS 6.61 vs. 13.91, surgeries 15% vs. 39%, costs $7,531 vs. $30,757).
Palliative Care Order Placed in the Emergency Department versus after Admission by Subgroup
LACE, length of stay, acuity, comorbidities, ER visits; LTCF, long-term care facility; O/S, outside.
Discussion
This pilot study shows that early ED PC involvement can possibly lead to multiple benefits for both patients and hospital systems. EM clinicians have a significant opportunity to impact downstream care by simply recognizing patients who may benefit from PC consultations. Specifically, our patients identified in this pilot study experienced a shorter hospital stay and underwent fewer surgical procedures and radiographic studies, which resulted in overall decreased costs.
The goal was to promote the early involvement of the palliative team and guide patient care in accordance with their personal goals. ED recognition of these patients facilitated this process and allowed the palliative team to initiate goal-directed conversations early in the patients' hospital stays. These conversations resulted in a shift to hospice care, discontinuation of chemotherapy, and family selection to not move forward with procedures such as a feeding tube.
The ACT pathway is different than prior studies since its broader criteria accommodate for a wider variety of PC conditions (Fig. 1). Specifically, many PC studies focus primarily on oncological patients.10,16,17 Our pilot study included additional indications such as cardiac arrest, functional disability, cognitive impairment, and patients with high LACE scores. The complex nature of these inclusions casts a wider net to include a higher number of patients who would benefit from palliative services.
There has been a traditional misunderstanding in the ED of PC as a specialty. The creation of this pilot study attempted to remedy issues in the AdventHealth campuses regarding the under-recognition of patients appropriate for palliative intervention. The difficulty in our hospital mirrors previous research that elucidates confusion of the initiation of PC early in a disease state. 18 This may explain the disconnect between the support for PC among large specialty organizations and the lack of a consistent palliative referral process in the ED.19–21
The concept of a PC specialist as a rounding team member on complex patients in the acute care arena is integral to the evolution of hospital-based medicine, and allows enhanced patient-centered decision making in relation to acute care interventions involving those with chronic illnesses. 22 EM, as a specialty, still under-recognizes the importance of involving a palliative team early,1,2,5,6,8,13 even though many leaders in the specialty have been touting the importance of this concept for several years.3,4 Our pilot study was an attempt to mitigate this problem.
In addition, the cost of health care in the United States is closely scrutinized. Hospitals are searching for cost-saving methodologies, and initiating the PC process in the ED serves as a potential method to accomplish this strategy. ED PC consultation showed the above-mentioned patient-centered improvement in care, while also reducing cost per patient (Fig. 3).
ED clinicians should strive to provide optimal medical care and respect the treatment goals of patients that can minimize unnecessary lengthy hospital stays and invasive procedures. The pilot study showed that involving a PC team early in a patient's course gives that patient the best chance to discuss care options and realize their goals. In addition, clinicians must recognize the benefits of PC are not limited to those acutely dying from incurable diseases. By focusing ED efforts on expanding routine PC to a wider group of patients suffering from chronic illness, patients will benefit earlier, as a PC team may focus on “quality of life” as much as “quantity of life.” As a secondary benefit, decrease in cost goes hand-in-hand with promoting goal-directed care. We hope that this pilot study acts as springboard to expand these efforts.
The only potential negative trend that we found using the ED PC protocol was a trend toward increased hospital revisit rates in the ED PC group. The reason for this is unclear. Additional studies are needed to investigate this further.
Limitations
This study's main limitation was the low percentage of eligible patients enrolled (12.1%, Table 6). As this study was a pilot project designed to promote a larger research trial, the decreased sample size was felt to be something that could be rapidly improved upon as this pathway expands. Among factors affecting our sample size, the biggest issue continues to be a need for stronger education regarding PC in the ED with a greater advertisement of the PC ACT program to ED providers.
Limitations of Sample Size
EM, Emergency Medicine.
Furthermore, the complex inclusion criteria may have acted as another barrier. Providers with limited experience in PC may struggle to recognize and remember which patients qualify to use the PC pathway during our pilot study rollout, especially in the fast-paced ED environment. We hope that as this pathway expands, investment into further training for ED providers will allow for greater recognition of patients meeting PC criteria. Although these factors led to a decrease in the overall power of the study, it is interesting that the findings did show a decrease in ALOS as well as the fewer surgeries and radiological tests per patient (p < 0.01). Based on our results, we theorize that larger randomized control studies would validate these findings.
Conclusions
In this study, we piloted a PC pathway for the early identification of a broad spectrum of palliative patients within the ED. The goal was to provide a better collaborative and goal-directed care through early ED PC consultation. Our study showed that those patients who received a PC consultation order in the ED experienced a decreased ALOS, fewer surgeries and radiology studies, and a concordant decrease in cost. From our findings, we were encouraged that integrating PC into the principles of EM resulted in measurable improvements in care. The time is now for ED clinicians to increase the partnership with their PC colleagues.
Footnotes
Authors' Contributions
C.J.D., Y.D., D.J.P., P.B.O., J.K., S.A., and K.H. conceived the study design and its implementation, data review and analyses, data interpretation, and article writing. C.J.D., D.J.P., P.B.O., J.L., and J.K. supervised the conduct of the study and data collection. D.J.P., Y.D., J.L., S.L., D.B., and M.M. participated in the data collection, management, analyses, interpretation (including quality control), statistical advice, created graphs and tables, and helped writing the draft. C.J.D. and Y.D. performed peer-reviewed literature search, scientific discussion, data interpretation, created tables, and drafted the article for publication, and all authors contributed substantially to its revision. D.J.P., P.B.O., and J.K. oversaw the project operation. C.J.D., Y.D., and P.O.B. take responsibility for the article as a whole.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.