
Abstract
Background:
Individuals experiencing homelessness face increased morbidity and mortality. The Canadian Toronto-based Palliative Education and Care for the Homeless (PEACH) program was launched to better support those experiencing homelessness with life-limiting illness.
Objective:
To describe the population served by PEACH.
Methods:
A chart review of deceased clients from 2014 to 2017 was conducted.
Results:
Sixty-three individuals were included in the analysis. 85.7% were male and the median age was 60 years. 35.4% resided in shelters, 26.2% in supportive/transitional housing; only 3.2% were sleeping on the streets. Cancer was the most common diagnosis (61.9%). 58.7% of clients had mental health diagnoses and 61.9% endorsed substance use. Locations of death included palliative care unit and hospice (44.4%), hospital (23.8%), supportive housing (12.6%), and shelter (7.9%).
Discussion:
PEACH serves diverse clientele with unique care needs. This study will inform further palliative care research and interventions for those experiencing homelessness.
Introduction
Individuals experiencing homelessnes ssuffer from increased and early mortality due to several factors, including the adverse social determinants of health. This is often compounded by comorbid complex mental health and substance use disorders.1,2 Life expectancy among homeless persons has been shown to be near half that of the general population. 3 Health care utilization patterns also illustrate the increased disease burden among those experiencing homelessness. They are nine times more likely to access the emergency department, with higher rates of hospital admission and ambulatory facility use compared with age- and gender-matched individuals. 4
Early integration of palliative care has been shown to improve quality of life, symptom burden, patient satisfaction,5,6 and in some cases, life expectancy. 5 However, there are significant barriers to the incorporation of palliative care services for structurally vulnerable and marginalized populations. 7 Previous studies have identified several reasons for this access gap, including mistrust of the health care system, 8 challenges in palliative care delivery, 9 hostel and shelter staff burden, 10 and health care workers' biases and lack of comfort in providing appropriate care. 1
Despite the challenges identified, support for the delivery of palliative care to those experiencing homelessness and precarious housing is increasing in Canada. Established programs exist in four major cities: Victoria, Calgary, Toronto, and Ottawa. 11 As this national network grows, so does the pressure to increase institutional support to further enhance services offered. To better understand the population these programs support, a retrospective chart review of the Toronto-based Palliative Education and Care for the Homeless (PEACH) Program was conducted. This is the first study aiming to assess a palliative care outreach program for homeless individuals in Canada.
Methods
The PEACH program was established in 2014 as an outreach intervention aiming to provide symptom management and psychosocial supports through a harm reduction and trauma-informed care lens. The team consists of palliative care physicians, care co-ordinators, nurses, and health navigators embedded within the publicly funded home care system. A retrospective chart review was conducted of PEACH. Research ethics approval was attained from the St. Michael's Hospital Research Ethics Board (REB # 18-027). The period of inclusion was from the program's inception to 2017. The study population included all deceased clients of PEACH. Clients without a documented date of death were excluded. Variables collected included demographic information, referral details, palliative diagnosis, comorbidities, substance use status, health care utilization, and resuscitation status. Data were analyzed using descriptive statistics.
Results
Demographics
From 2014 to 2017, 70 PEACH clients died; 63 were included. Fifty-four (85.7%) identified as male and 9 (14.2%) as female. Median age at death was 60 years (range 28–84). Housing data are described in Table 1. Housing categories were based on the Canada Mortgage and Housing Corporation (CMHC) “Housing Continuum.” 12
Housing Status of Clients at Time of Referral and Time of Death
Referral information
Health care providers, including physicians, nurse practitioners, care co-ordinators, and social workers, made 74.6% of PEACH referrals. 15.8% came from individuals working in social services, including shelter staff, outreach workers, and case managers. 9.5% of cases had an unknown referral source. Most common reasons for referral were palliative planning (79.4%) and symptom management (68.2%). Median survival time after referral was 98 days (range 12–1023).
Health status and care preferences
Cancer was the most common palliative diagnosis (62%) followed by chronic nonmalignant (35%) and infection (3%). Further detail about palliative diagnoses is found in Table 2. Palliative performance scale (PPS) at first visit was recorded for 52 clients. 13.5% had a PPS ≥70, 17.3% had a PPS of 60, 57.7% had a PPS of 50, and 11.5% had a PPS of 40. No initial PPS were <40. Mental health and substance use comorbidities were also assessed. Depression was the most common diagnosis (25.4%), followed by psychotic disorder (15.9%), anxiety (12.7%), post-traumatic stress disorder (7.9%), and bipolar disorder (6.4%). 41.3% of clients had no documented mental health diagnosis, 41.3% had 1, and 17.5% had >1. Tobacco was the most commonly used substance (47.6%), followed by alcohol (46.0%), other drugs (30.2%), and opioids (7.9%). 38.1% of clients endorsed using no substances, 41.3% reported using 1, and 20.4% reported used >1. Resuscitation status was the main care preference evaluated—results are illustrated in “Figure 1.”
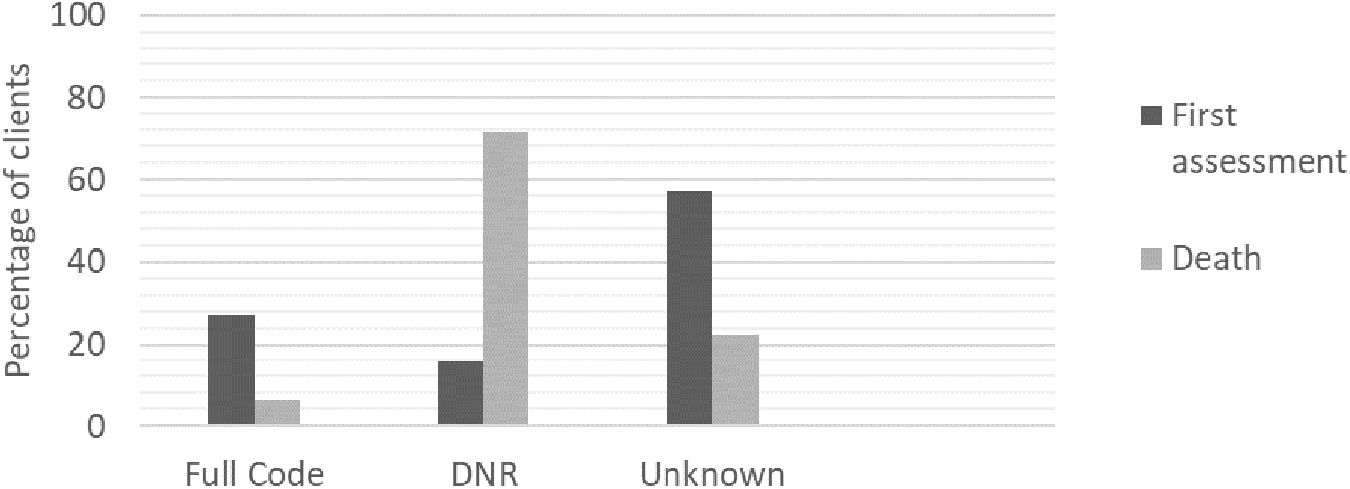
Resuscitation status at time of first visits and time of death. DNR, do not resuscitate.
Primary Palliative Diagnosis of Clients
Health care utilization
Most clients (81.0%) received care from a physician with specialization in their palliative diagnosis (e.g., oncologist); 15.9% had no documented specialist care, whereas specialist involvement was unknown for 3.2%. In terms of acute care utilization after referral, 39.7% of clients had no documented emergency department (ED) visits, 33.3% visited once, 4.8% visited twice, and 20.7% had ≥3 visits. 38.1% of clients had no documented hospital admissions, 46.0% had 1, 6.3% had 2, and 7.9% had ≥3 admissions.
Discussion
This is the first retrospective chart review of a Canadian outreach-based palliative care program for individuals experiencing homelessness. This article aims to address gaps in the literature about homeless and vulnerably housed populations with palliative care needs.
Most PEACH clients identified as male. Interestingly, the percentage of males in the study is higher than the proportion of males experiencing homelessness in Toronto (54%) based on a 2018 Street Needs Assessment. 13 This may relate to initial locations of practice for the program—a high number of referrals originally came from Toronto men's shelters. Over time, as awareness has grown and referrals have come from new sources, more female clients have received support from PEACH.
The PEACH program did provide care to individuals in diverse settings along the “housing continuum”; only 41.3% were living in shelters or sleeping on the streets at time of referral. The remaining 58.7% resided in varying degrees of precarious housing. These data reflect the wide variability in housing quality and security experienced by those with a history of homelessness. Furthermore, clients residing in different settings have differing support needs. This is especially noted when reviewing place of death. Most clients died in hospital (23.8%) and palliative care unit (PCU)/hospice (44.4%). Furthermore, only 20.8% of individuals initially living in shelters died in shelters. Although the study did not capture preferred place of death, it is likely that more individuals died in institutions because of the challenges in providing palliative care within nontraditional housing settings. Barriers to palliation outside of hospital or PCU are well documented in the literature 1 and include, but are not limited to, lack of social supports, variable access to home care, and financial burden. However, support from the PEACH program (such as through the facilitation of home care supports, education and support for shelter staff, and effective symptom management) likely enabled clients to spend more time outside of hospital and PCU.
Similar to other Canadian palliative care populations, most PEACH clients had a malignant diagnosis. However, a much larger proportion was receiving palliation for chronic nonmalignant disease when compared with inpatient palliative care populations. 14 In addition, the median age in our study was lower than that of other palliative care populations. These findings are consistent with other research identifying an earlier onset of chronic nonmalignant illnesses and lower life expectancy among individuals experiencing homelessness when compared with those who are housed. 3 Mental health and substance use comorbidities were prevalent among PEACH clients. Depression and psychotic disorder were the top two mental health diagnoses, whereas tobacco and alcohol were the most used substances. Furthermore, almost two-thirds of clients reported a history of nontobacco substance use. Individuals with mental health and/or substance use disorders often face barriers to care from institutions and health care providers for reasons, including strict abstinence-based policies, risk and safety management, and limited implementation of harm reduction techniques. 15
The establishment of trusting long-term relationships is crucial in providing palliative care that is person-centered, compassionate, and dignified. One area of the study this may be reflected in is end-of-life care preferences. Although at the beginning of the study 57.1% of individuals had “Unknown” resuscitation statuses, this number decreased to 22.2% by the end of the study. Resuscitation preference is only one element of an individual's goals of care. However, previous research has identified the unique challenge of exploring death and dying among people experiencing homelessness. 16 PEACH providers are well equipped to facilitate conversations about goals of care, particularly given the importance placed on building trust and establishing longitudinal relationships with clients.
The main limitation of the study is variability in medical record documentation among PEACH providers. Subsequently, some subjectivity was required to interpret and classify data that were not clearly described in patient charts. Certain variables were omitted for this reason, including ethnicity. There was also a lack of patient data from before PEACH program involvement. This impacted the ability to examine health care utilization over time.
Conclusion
Although the PEACH program plays a critical role in providing palliative care to individuals experiencing homelessness, its existence also epitomizes the fact that the needs of this population are not taken into consideration when mainstream palliative care programs are designed and implemented. The results of this study will inform further research exploring the challenges and opportunities for palliative care provision for the homeless. As well, these data will be used to guide the development of future interventions aimed at improving the lives of this diverse population.
Footnotes
Authors' Contributions
E.S. and N.D. conceived of the study idea. N.D. helped with accessing the medical records used for the review and supervised E.S. throughout the study development, data collection, and interpretation. E.S. wrote the article with support from N.D.
Acknowledgments
Our sincere thanks to Dr. Kosalan Akilan and Dr. Daniel Kapustin for their assistance with the chart review. We also thank Amanda Pereira for her assistance in refining the literature review and discussion. Finally, we are grateful to all those who have worked with and continue to support the PEACH program.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.