
Abstract
Context:
Some patients require continuous deep sedation (CDS) for refractory symptoms despite intensive palliative care. The principle of proportionality is proposed on the basis of clinical decisions, but no validated tools to assist such decision making are available.
Aim:
To develop a scoring system to determine whether CDS is proportionally appropriate.
Subjects and Methods:
A secondary analysis of a nationwide questionnaire survey of Japanese palliative care specialists was performed. Physicians were asked to rate the degree that they believed CDS to be appropriate in a total of 27 scenarios based on a combination of 3 factors with 3 levels: (1) the estimated survival (days, weeks, and months), (2) the patient's wish (clear and consistent, somewhat unclear and/or inconsistent, and unclear or inconsistent), and (3) confidence in refractoriness of the symptom (definite, probable, and unsure). Based on logistic regression analyses, a scoring system with two formulas (the proportionality score to determine that continuous deep sedation is appropriate [ProScoreCDS-appropriate] and proportionality score to determine that continuous deep sedation is inappropriate [ProScoreCDS-inappropriate]) to predict specialists' decision that CDS is appropriate or inappropriate was developed. The accuracy of the formulas was investigated.
Results:
Among 695 palliative care specialists, 469 returned the questionnaire (response rate, 69%) and 440 were analyzed. Logistic regression analyses identified that all three factors were significantly associated with physicians' decisions about the appropriateness of performing CDS. Using weighted value, the total score ranged from 3 to 67 for ProScoreCDS-appropriate, and 3 to 27 for ProScoreCDS-inappropriate. The area under the curve (AUC) values of ProScoreCDS-appropriate and ProScoreCDS-inappropriate were 0.88 (95% confidence interval [CI], 0.87–0.89) and 0.81 (95% CI, 0.81–0.82), respectively. Using cutoff points of 41 and 14, sensitivity and specificity were 68.6% and 88.9% for ProScoreCDS-appropriate and 67.7% and 76.0% for ProScoreCDS-inappropriate, respectively.
Conclusion:
A scoring system to determine whether CDS is proportionally appropriate can be constructed, and a further study to develop a clinical tool is promising.
Introduction
Imminently dying patients experience various distressing symptoms,1–5 and continuous deep sedation (CDS) is used for some patients whose symptoms become refractory despite intensive palliative care.6–8 As there is a critique that loss of consciousness means the end of a person's social life,9–13 the decision of whether the patient is a suitable candidate is of great importance.14,15
Ethical validity of CDS is based on the principle of proportionality.2–5 Although the principle of proportionality is used in many different contexts,2–5,16–18 in the double effect principle, if an action with a predicted bad effect is ethically justifiable, there should be proportional reasons. 16 In clinical practice of palliative sedation, the potential reasons can include refractoriness of the symptom, limited life expectancy, intensity of suffering, and the patient's wishes.19–23 If appropriateness of CDS could be quantified with a scoring system, it would help physicians to determine the indication of CDS. The primary aim of this study was thus to develop a scoring system to determine whether CDS is proportionally appropriate for the patient situation.
Subjects and Methods
This is a secondary analysis of a nationwide questionnaire survey of Japanese palliative care specialists on palliative sedation. 23 The nature of this study was exploratory and concept of proof, that is, our intention was to assess the prospect of constructing a scoring system, and not to validate a tool ready for clinical use. In that original study conducted from August to December 2016, certified palliative care specialists of the Japanese Society of Palliative Medicine were asked to rate the degree that they believed CDS is proportionally appropriate in a total of 27 scenarios. The responses were based on a 5-point Likert scale: I would definitely not perform CDS (1), probably not perform CDS (2), might perform CDS on a case-by-case basis (3), would probably perform CDS (4), and would definitely perform CDS (5). Each scenario was defined using three factors: (1) the estimated survival periods (days, weeks, and months), (2) the patient's wish for CDS (clear and consistent, somewhat unclear and/or inconsistent, and unclear or inconsistent), and (3) the confidence of the physician regarding refractoriness of the symptom (definite, probable, and unsure). Using all combinations of 3 factors, a total of 27 scenarios were generated. The presentation of refractoriness was accompanied by examples, literally, definite (e.g., dyspnea related to irreversible organ failure), probable (pain for which other intervention analgesics might be effective with uncertain success rate), and unsure (psychoexistential suffering).
Endpoint
The endpoint was the decision of the palliative care specialists about whether they regarded performing CDS as being appropriate for the patient's situation. For analyses, we divided each response into two categories: CDS is appropriate (response 4 or 5) and CDS is inappropriate (response 1 or 2).
Independent variables included in the model
Independent variables used were (1) the estimated survival, (2) the patient's wish for CDS, and (3) the confidence of the physician regarding refractoriness of the symptom.
Development of a scoring system to determine whether CDS is appropriate
To determine whether CDS is appropriate, we developed a scoring system using two formulas (Fig. 1). One determines whether CDS is appropriate, adopting the positive decision of the specialists that they would probably or definitely perform CDS. Another determines that CDS is inappropriate, and adopts their negative decision that they would probably or definitely not perform CDS. We called the former the “proportionality score to determine that CDS is appropriate” (ProScoreCDS-appropriate), and the latter the “proportionality score to determine that CDS is inappropriate” (ProScoreCDS-inappropriate). Using the two formulas, all patients could be classified into one of three categories: (1) proportionally appropriate, (2) controversial, and (3) proportionally inappropriate (Fig. 1). We decided to test this three-classification model, because setting a controversial category is beneficial to interpret the clinical situation, where a simple yes-no distribution paradigm is often unsuitable.
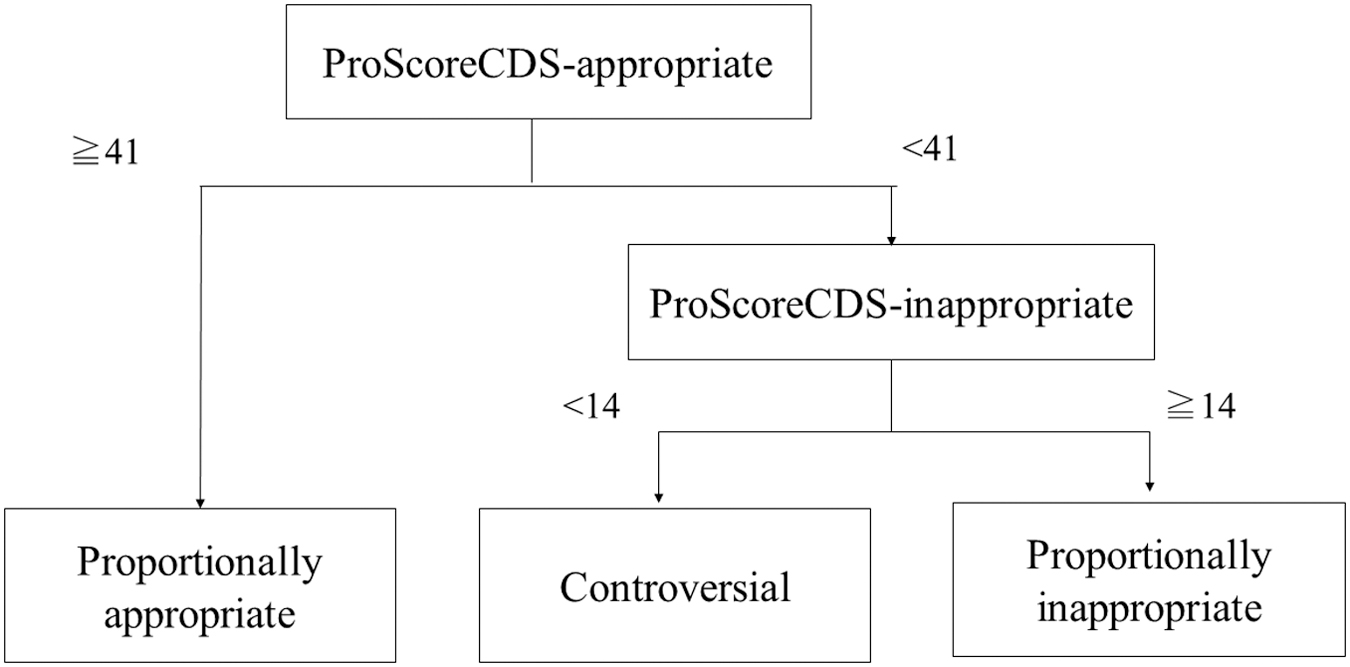
A scoring system to determine whether CDS is appropriate. When ProScoreCDS-appropriate is 41 or more, CDS is considered proportionally appropriate. ProScoreCDS-appropriate is <41 and ProScoreCDS-inappropriate is 14 or more, CDS is considered proportionally inappropriate. In other cases, CDS is controversial. Rationales for given cutoff points are shown in Results section. CDS, continuous deep sedation; ProScoreCDS-appropriate, proportionality score to determine that continuous deep sedation is appropriate; ProScoreCDS-inappropriate, proportionality score to determine that continuous deep sedation is inappropriate.
Statistical analyses
First, to identify the likelihood of a physician deciding that CDS is appropriate, two multiple regression analyses were performed. One used the responses of 4–5 (appropriate), and the other used the responses of 1–2 (inappropriate) as dependent variables. The partial score value was defined as the nearest integer obtained; thereafter, two proportionality scores were calculated by summing the partial scores. Second, we investigated the predictability of the model using receiver operating characteristic curves, and calculated the sensitivity, specificity, positive/negative predictive values, and overall accuracy for several cutoff points. All analyses were performed using IBM SPSS statistics (version 26; IBM, Tokyo, Japan)
Results
A total of 695 palliative care specialists were identified, and 469 returned the questionnaire (response rate, 69%). As 29 of them refused to participate, the remaining 440 were analyzed. Table 1 gives the background of the participants. The distribution of physicians' decisions on whether to perform CDS was definitely would not perform CDS in 31.6% (n = 3639), probably would not perform CDS in 32.1% (3705), might perform CDS on a case-by-case basis in 23.4% (2692), probably would perform CDS in 10.1% (1169), and definitely would perform CDS in 2.8% (320).
Background of the Participants (n = 440)
CDS, continuous deep sedation; SD, standard deviation.
Table 2 gives odds ratios for specialists' decisions on whether CDS is appropriate or inappropriate. All variables investigated were significantly associated with their decisions. Using the partial score values, the total score ranged from 3 to 67 for ProScoreCDS-appropriate and from 3 to 27 for ProScoreCDS-inappropriate. For example, if a patient's estimated prognosis was days, the patient's wish was clear, and the symptoms were probably refractory, ProScoreCDS-appropriate was 61 (29 + 29 + 3).
Odds Ratios for Physicians' Decision that Continuous Deep Sedation Is Appropriate or Inappropriate
p < 0.001.
The presentation of refractoriness was accompanied with examples, literally, definite (e.g., dyspnea related to irreversible organ failure), probable (pain for which other intervention analgesics might be effective with uncertain success rate), and unsure (psychoexistential suffering).
CI, confidence interval.
Figure 2 demonstrates the area under the curves (AUCs) for proportionality scores. The AUC values of ProScoreCDS-appropriate and the ProScoreCDS-inappropriate were 0.88 (95% confidence interval [CI], 0.87–0.89) and 0.81 (95% CI, 0.81–0.82), respectively. Table 3 gives the sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy with various cutoff points. When 41 was adopted as a cutoff point for ProScoreCDS-appropriate, physicians' decision that CDS was appropriate was predicted with a sensitivity of 68.6% and specificity of 88.9%. When 14 was adopted as a cutoff point for ProScoreCDS-inappropriate, physicians' decision that CDS was inappropriate was predicted with a sensitivity of 67.7% and specificity of 76.0%.

ROC curve of the ProScoreCDS-appropriate and ProScoreCDS-inappropriate. CDS, continuous deep sedation; ProScoreCDS-appropriate, proportionality score to determine that continuous deep sedation is appropriate; ProScoreCDS-inappropriate, proportionality score to determine that continuous deep sedation is inappropriate.
Sensitivity and Specificity of ProScoreCDS-Appropriate and ProScoreCDS-Inappropriate
Bold indicates recommended cut-off points.
ProScoreCDS-appropriate, proportionality score to determine that continuous deep sedation is appropriate; ProScoreCDS-inappropriate, proportionality score to determine that continuous deep sedation is inappropriate.
Discussion
This is the first attempt to develop a scoring system to determine whether CDS is proportionally appropriate. Using the decisions of palliative care specialists as a gold standard, we successfully developed a scoring system with two formulas including three components: expected prognosis, patient's wish, and physician's confidence in refractoriness of the symptoms. This scoring system enables experts' way of thinking to be visible and measurable for many clinicians. Nonetheless, caution is needed that the nature of this study was concept of proof, and use of the scoring system without adequate validation and education has a risk, especially for nonexperts, to incorrectly assess patient condition.
Expected survival is one of the most powerful factors influencing a physician's decision. A patient with a predicted survival of days is likely to be determined as being appropriate 29 times more than a patient with that of months, whereas CDS is regarded as being inappropriate for a patient with predicted survival of months 11 times more than those of days survival. These findings are consistent with the clinical guidelines, stressing that CDS should be reserved as a last resort for patients with very short survival, principally days or less.2–5
Another key factor was physician certainty regarding refractoriness of the symptoms, or symptoms are psychoexistential suffering. These findings are consistent with concerns that CDS can be a type of euthanasia if performed in patients with longer predicted survival suffering from psychoexistential suffering.24–26 Conceptual studies proposed clarification of psychoexistential suffering, that is, psychological symptoms as a direct result of the disease or existential suffering without biological pathology.17,26 Future studies should specify psychoexistential suffering in more detail.
The nature of this study is exploratory, and intrinsic limitations should be overcome in future studies. First, variables to be used were limited. Further study should consider more variables, such as the intensity of the symptom, nature of suffering (physical, psychoexistential defined in more detail, or a combination), opinions of families, and resources available.17,19–21,26 Second, this study did not determine the practical method for how each variable was rated in clinical settings, for example, how a clinician estimated patient survival (use of validated measures such as prognosis in palliative care scale [PiPS] model or clinical estimation. 27 Especially, how to score a patient with unknown wishes for sedation should be operationally clarified. Third, we used only performing CDS as an end point, a future study should test more broad concepts of palliative sedation. Fourth, we proposed multiple cutoff points, but the cutoff points should be finally determined according to the clinical aim, such as whether specificity or sensitivity is prioritized. Fifth, the accuracy was calculated within the sample, and independent validation is needed. Furthermore, all data were based on vignette surveys, and the use of actual patient data will be identical in further study. Sixth, although we believe that the response rate was high enough (69%), there may be some selection bias. Finally, the principle of proportionality has a broad meaning, and there may be some confusion in labeling this scale as a measure to quantify proportional appropriateness. Simple name such as a scale to determine the clinical appropriateness of CDS might be more suitable.
In conclusion, a scoring system to determine whether CDS is appropriate could be constructed using multiple variables. Further studies to develop a clinical tool may assist clinicians when they face a difficult situation related to CDS.
Footnotes
Authors' Contributions
T.M. and A.S.N. contributed to the conception/design of the study, the analysis, interpretation of data for the study, and drafting the study. K.I., M.I., J.H., H.A., Y.K., and S.T. contributed to interpretation of data for the study and revised it critically for important intellectual content. All authors provided final approval of the version to be published.
Ethical Approval
This study was approved at the institutional review board of Seirei Mikatahara General Hospital (18-58).
Consent to Participate
Return of the questionnaire was regarded as consented to participate.
Consent for Publication
The study was explained to each participant as a written material, and return of the questionnaire was regarded as consented for publication.
Availability of Data and Material
Data are available on reasonable request to the corresponding author.
Funding Information
This study was supported by JSPS KAKENHI Grant No. JP19H03869.
Author Disclosure Statement
No competing financial interests exist.