
Abstract
Background:
Scrambler therapy (ST) is a relatively new neuromodulation technique that is useful in treatment of medication-resistant pain syndromes, including chemotherapy-induced peripheral neuropathy and other chronic pain syndromes. Amyloidosis commonly leads to peripheral neuropathy, and although the mechanism is unclear, it is possibly related to amyloid deposits on the nerve.
Case Presentation:
In this case presentation, we describe the novel use of ST for a patient with 13 years of neuropathic pain related to amyloidosis and worsened by chemotherapy. The patient reported bilateral hand pain with burning and aching and bilateral numbness on the soles of her feet. Her upper extremities were treated with 4 days of 40 minute ST treatment sessions providing reduction in her pain scores to zero.
Discussion:
Current therapy for amyloid peripheral neuropathy aims at treating the underlying condition, and then medical management with gabapentinoids. This is first case presentation showing successful treatment with ST.
Introduction
Each year 1274 to 3200 U.S. patients develop immunoglobulin light chain amyloidosis (amyloid light [AL] amyloidosis) caused by deposition of AL chains produced by plasma cells, a prevalence of 2.5 per 100,000 people. AL amyloidosis has neural involvement in 20–34% of patients, and 7–12% of all primary amyloidosis patients present with an isolated neuropathy months to years before other manifestations of the systemic disease are evident. 1 Neuropathic pain is a common feature occurring in 17% to 35% of patients and can occur early in the disease course. 2 Treatment is often unsatisfactory with available agents such as gabapentin or pregabalin, and tricyclic antidepressants can worsen orthostatic hypotension.
Scrambler therapy (ST) is a relatively new neuromodulation technique 3 that is useful in treatment of medication-resistant pain syndromes, including chemotherapy-induced peripheral neuropathy4,5 and other chronic pains such as neuromyelitis optica spectrum disorder, 6 and central pain. 7 ST modulates the chronic pain signal by substituting “non-pain” information from five artificial neurons that capture surface receptors of the C nerve fibers. 8 Pairs of EKG electrodes are placed on the skin within the dermatome proximal to the area of pain and the stimulus adjusted to tolerance. There are now more than 55 ST citations listed in PubMed including 4 successful4,9–11 and 1 unsuccessful 12 randomized trials.
We used ST to treat a patient with AL amyloidosis and 13 years of severe refractory pain, which resulted in successful relief of her pain. The patient gave written informed consent for presentation of this case report.
Case Description
Ms. P is a 70-year-old woman with IgG lambda multiple myeloma and 13 years of painful neuropathy due to AL amyloidosis, worsened by chemotherapy. Her AL amyloidosis was diagnosed first with absence of taste, and pain with numbness extending above her malleoli. She was followed for smoldering myeloma for 10 years. When she developed frank myeloma she received treatment with lenalidomide and dexamethasone; daratumumab; and carfilzomib plus dexamethasone. These regimens put her myeloma into remission—but her pain remained. She reported constant bilateral hand pain with burning and aching from fingertips proximal to wrists. She had partial relief from pain medications and paraffin baths but no relief from diclofenac gel. She reported numbness on the soles of her feet and daily stabbing foot pain lasting 1–5 minutes, but no persistent pain. Her numerical rating scale pain scores were average 6 to worst of 10 without ever achieving a reduction to zero on her pre-ST analgesic regimen, which included duloxetine 30 mg daily, gabapentin 1200 mg three times daily, and oxycodone 10 mg as needed (1–3 × daily).
The patient hoped for better pain control in her hands/arm after ST treatment, with an improvement in her quality of life and functionality. She received four daily 40-minute ST treatments to the C 6, 7, and 8 dermatomes, placing the electrodes on her skin, proximal to the area of pain on her upper extremities (Fig. 1). Her upper extremity pain reduced to 0 (zero) and has remained there (Fig. 2). On follow-up, ∼8 months after her original treatment, her bilateral upper extremity neuropathy remained well controlled. She requested additional ST for her lower extremities due to worsening neuropathy there. She remained off treatment for her myeloma. Her post-ST analgesic regimen was similar to her previous regimen with only an increase in her duloxetine to 60 mg daily and continued gabapentin 1200 mg three times daily and oxycodone 10 mg as needed.

Position of ST electrode sets to cover dermatomes C6–8. Five sets available. Amyloid neuropathy C6, 7, 8 dermatomes on R; combined C6–7 and 7–8 on L. ST, scrambler therapy.
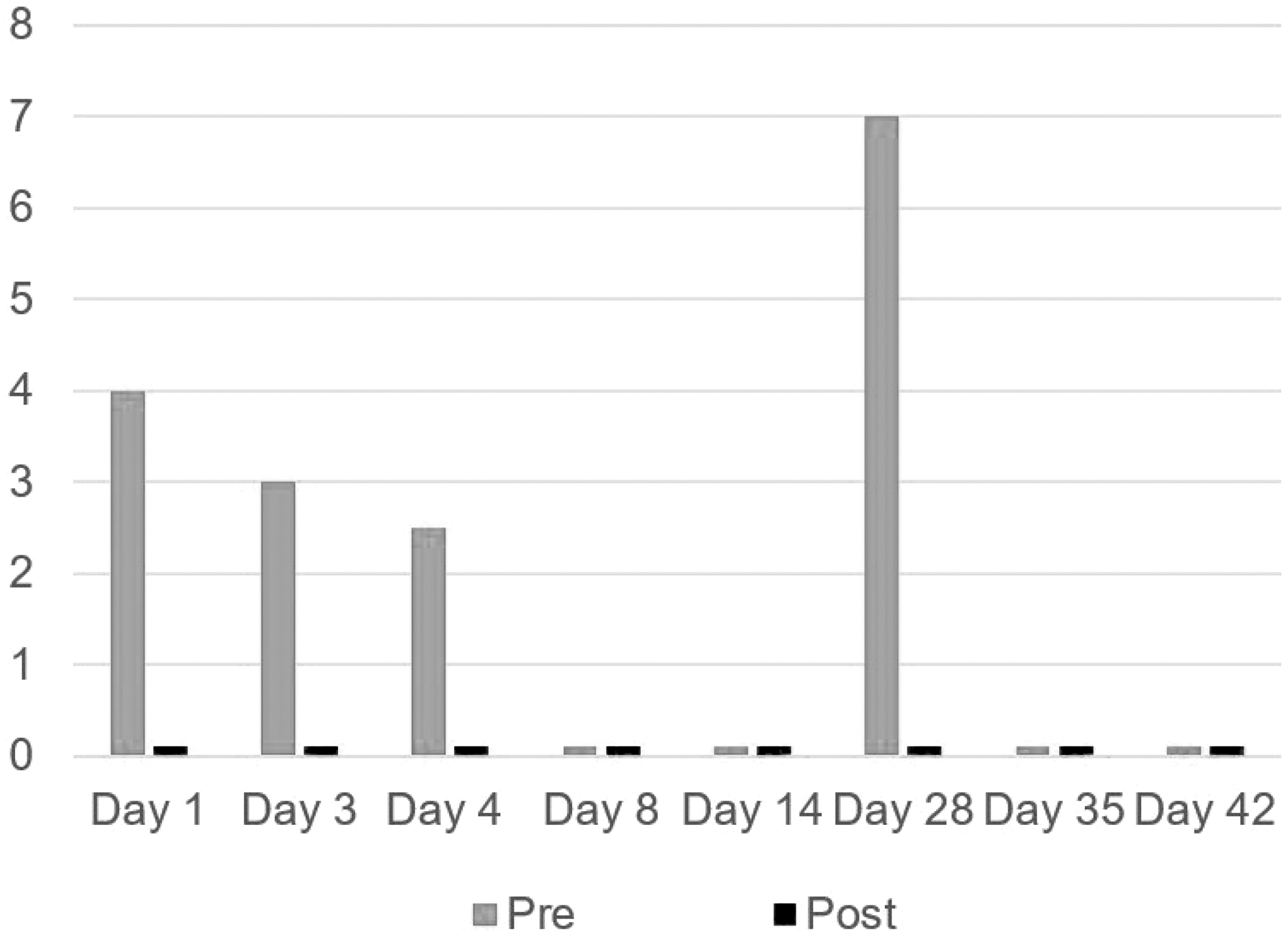
Pain scores pre- and post-ST, by days. “0” is represented by 0.1 to show on the graph.
Discussion
We describe the novel use of ST for a patient with 13 years of neuropathic pain related to AL amyloidosis and worsened by chemotherapy. Current treatments for AL amyloidosis neuropathy are aimed primarily at the underlying disease process, including autologous stem cell transplant, chemotherapy (corticosteroids, alkylating agents [melphalan and cyclophosphamide]), immunomodulatory drugs (thalidomide and lenalidomide), and proteasome inhibitors (bortezomib). 13 An autologous stem cells transplantation can achieve hematological and organ responsiveness and improve long-term survival as it may halt progression. In patients who are not eligible for stem cell transplant the alternative treatment options may be utilized (1). Secondarily, symptomatic therapy for neuropathic pain is similar to treatments for other neuropathic pain syndromes such as diabetic neuropathy and includes anticonvulsants (i.e., gabapentin/pregabalin) and serotonin norepinephrine reuptake inhibitors (e.g., duloxetine/venlafaxine) (2) as was currently being used by the patient in this scenario.
Our patient experienced immediate and prolonged relief from ST. The device is easy to use and typically well tolerated by patients. The main limitations of ST include time, lack of provider awareness of the intervention, cost of therapy, and the limited number of machines and providers trained in the use of the device. Novel therapies that decrease reliance on pharmacological interventions are necessary not only to improve pain, but also to limit the adverse effects of escalating doses of opiate and other pain medications. Further research is needed to determine if ST can be used more widely for patients experiencing AL amyloid neuropathy as an alternative or in conjunction with medical management. As more patients are treated with ST, we remain hopeful that its use will become increasingly mainstream in the treatment of complex cancer pain.
Footnotes
Funding Information
This study was supported by grants NCI grant P 30 006973; 1 R01 CA177562-01A1, PCORI IHS 1609-36518; the Harry J. Duffey Family Fund for Palliative Care; The Lerner Foundation, Washington DC (all TS).
Author Disclosure Statement
None of the authors have conflicts of interest to report. Johns Hopkins Health System has received two ST machines as gift to the institution. The first was in 2011, and the second was released to JHHS after we had rented it to use in the randomized sham-controlled trial of ST in neuromyelitis optica spectrum disorder.