
Abstract
Background:
Understanding challenges of family caregivers within specific palliative care contexts is needed.
Objective:
To describe the challenges of family caregivers of patients with cancer who receive outpatient palliative care.
Methods:
We summarized the most common and most challenging problems for 80 family caregivers of cancer patients receiving outpatient palliative care in the midwestern United States.
Results:
Caregiver worry and difficulty managing side effects or symptoms other than pain, constipation, and shortness of breath were most common. “Financial concerns” was cited most as a “top 3” problem. Almost half of caregivers reported “other” problems, including family members, patient physical function, care coordination, and patient emotional state.
Conclusions:
The most common and most challenging problems of family caregivers of cancer patients receiving outpatient palliative care may differ from those experienced in other serious illness care contexts. Comparative studies on caregiver problems across the cancer care continuum can help develop and refine interventions.
Introduction
Palliative care is specialized holistic medical care for people living with a serious illness. 1 It is delivered by a specially trained team of health care providers who partner with a patient's primary physician and other specialists to provide additional support spanning the psychosocial, physical, and spiritual needs of the patient and their family members. 2 Palliative care is available for patients of all ages and at any stage in a serious illness. The goal of this type of care is to improve quality of life for patients and family members by managing patient symptoms, providing patients relief from the side effects of treatment, and helping patients and families navigate the stress that accompanies the illness journey. 1
Palliative care in cancer
Palliative care is beneficial to the health and well-being of cancer patients and their family caregivers. Research demonstrates that integrating palliative care with standard oncology care soon after a diagnosis of advanced cancer can improve a patient's quality of life and emotional health, and may prolong survival.3,4 Although the impact of palliative care services on cancer family caregivers has been studied to a lesser degree than its impact on patients, research suggests that family caregivers benefit in a number of ways, including improvements in addressing unmet needs while actively caregiving, and in grief outcomes during bereavement. 5 Palliative family caregivers have also reported feeling more satisfied with patient care overall compared with their counterparts whose patients were receiving standard oncology care.6,7
Despite the benefits palliative care offers family caregivers of cancer patients, it is relatively unknown what caregiving challenges these caregivers face. Research on the subject of palliative family caregiving has suffered from several important methodological limitations: heterogeneity of patient diagnoses, broad or imprecise operationalization of palliative care, failure to specify or distinguish delivery settings, and reliance on proxy reports or secondary analysis of qualitative data. Although research has been published on caregiving challenges in hospice, 8 the caregiving challenges of palliative family caregivers whose patients are receiving supportive care—but are not yet receiving hospice services—are rarely studied. This gap in the literature is notable given the ample evidence that family caregiving at the end of life is not a uniform experience.9,10 Thus, understanding the cancer caregiving experience within specific palliative care delivery settings (e.g., outpatient palliative care, inpatient palliative care, and home-based palliative care) may benefit health care systems as the need for increased personalized customizable support for patients and family members grows.
Study purpose and research questions
The purpose of this exploratory study was to describe the challenges faced by family caregivers of cancer patients who receive outpatient palliative care. Specifically, we sought to answer the following research questions: (1) what are the most common problems reported by family caregivers of cancer patients who receive outpatient palliative care and (2) which problems are most challenging for family caregivers of cancer patients who receive outpatient palliative care?
Methods
We conducted a secondary analysis of data provided by family caregivers who participated in a small randomized clinical trial (RCT) of a cancer caregiver support intervention. The intervention was offered through the outpatient palliative care clinic of an academic health center in the midwestern United States between October 2015 and February 2017 (R21CAXXXXXX; Principal Investigator: Washington). RCT participants were adult family caregivers of adult patients with a cancer diagnosis (any type or stage) who were receiving palliative care either concurrent with disease-directed treatment or as a stand-alone service. Anyone who identified as a “family caregiver” was deemed eligible to participate in the study, independent of their biological or legal relationship with the patient. More than one caregiver per patient could enroll in the study provided they were substantially involved in providing patient care. Detailed information on the original RCT, which was approved by the University of Missouri institutional review board, has been published elsewhere.
Data source
Before randomization to either the control or intervention group, all RCT participants completed baseline measures, including a demographic questionnaire and a problem checklist that had been created specifically for the study based on a review of the literature and our team's prior research (Fig. 1). Family caregivers completing the problem checklist indicated which of 11 common caregiving problems (e.g., managing patient pain and financial concerns) they had experienced in the prior two weeks. One item allowed caregivers to add symptoms that were not specifically included on the list. They were also given the option of writing in up to three “other” problems. Family caregivers then indicated which three problems had been the most challenging for them during the prior two weeks, selecting the most challenging, second most challenging, and third most challenging problems.
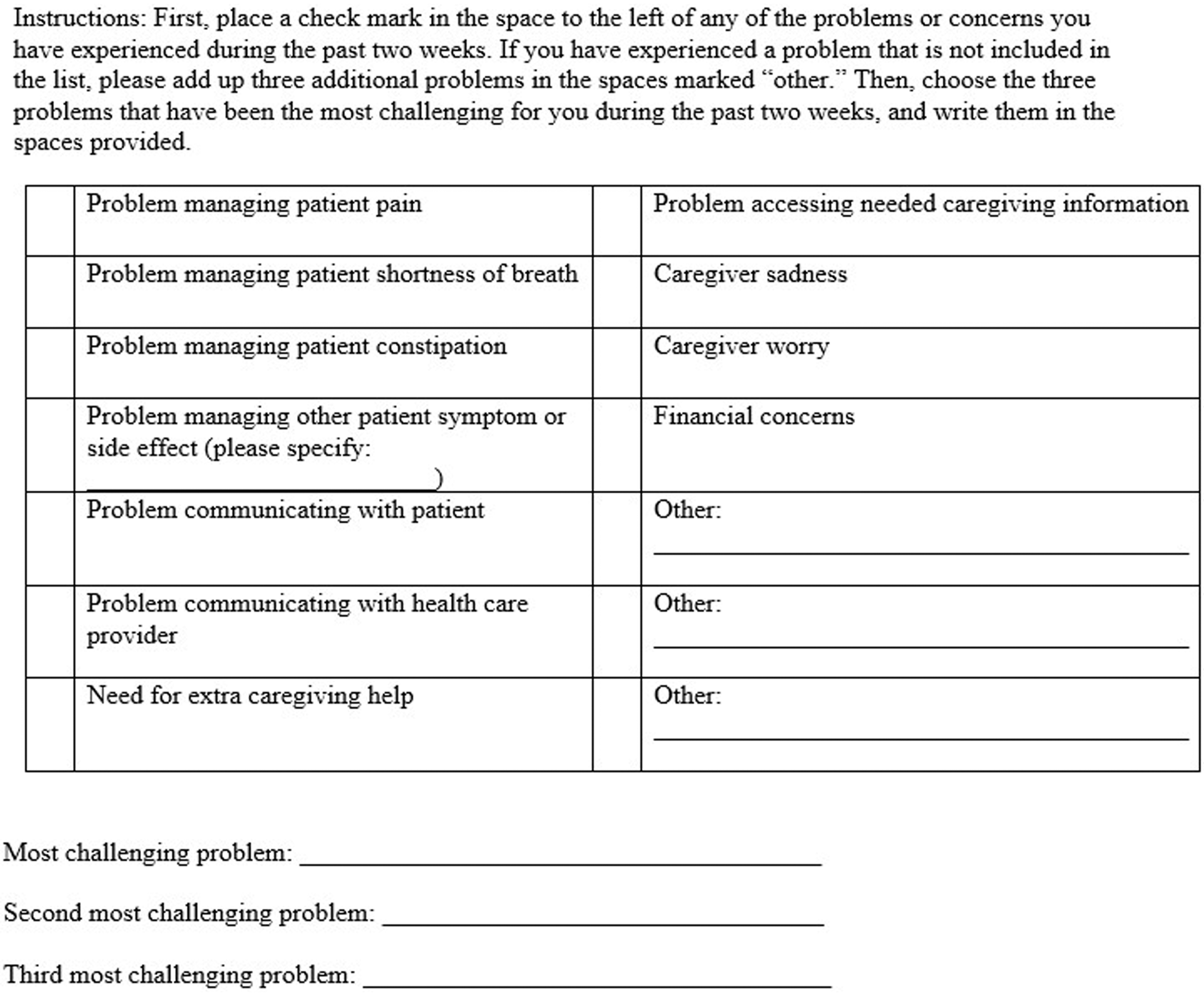
Checklist instrument.
We included RCT participants who completed a full set of baseline measures. We excluded two caregivers who cared for multiple patients, resulting in a final analytic sample of 80 caregivers and 69 patients for the present study (demographic characteristics are provided in Table 1).
Characteristics of Caregivers (n = 80) and Patients (n = 69) Who Participated in a Randomized Trial of a Cancer Caregiver Support Intervention
Due to rounding, percentages might not total 100.
GED, Graduate Educational Development test; SD, standard deviation.
Data analysis
Caregivers' responses were entered in a spreadsheet. We grouped family caregivers' “other” problems into 10 categories that, when combined with the 11 problems originally included in the problem checklist, resulted in a list of 21 possible caregiver problems. Data were imported into SAS for Windows v 9.4 (SAS Institute, Cary, NC), which was used for all analyses. To determine the prevalence of various caregiver problems, we ran basic descriptive statistics to quantify the number of family caregivers who reported experiencing each of the problems in the two weeks before study enrollment. To better understand the problems' relative intensity, we calculated the number of times family caregivers cited each of the problems as one of their three most challenging.
Results
Table 2 summarizes the problems encountered by caregivers during the previous two weeks and the number of times caregivers cited a problem as one of their “top 3” problems. Difficulty managing side effects or symptoms other than pain, constipation, and shortness of breath (separately reported on the checklist) was the most commonly cited problem, endorsed by approximately two-thirds of participants. Of the “other” side effects or symptoms written in, nausea and/or vomiting (n = 9), loss of appetite (n = 7), cognitive problems (n = 6), and fatigue (n = 6) were most commonly mentioned. Caregiver worry, financial concerns, and caregiver sadness were endorsed by at least half of participating caregivers, whereas problems managing the patient's pain and communicating with the patient were cited by at least one-third of participants. Notably, 42 of the 80 caregivers provided a response in the space provided for “other” problems. Of these, challenges related to family members other than the patient, the patient's physical function, care coordination, and the patient's emotional state were the most common additional problems written in. Financial concerns were listed most frequently among “top 3” problems (n = 35), followed by managing other side effects or symptoms (n = 27), managing patient pain (n = 24), and caregiver worry (n = 24).
Frequency with Which Cancer Caregivers Cited Problems and Listed Problems as a “Top 3” Challenge (N = 80)
Number of caregivers who selected or reported the problem as one of their “top 3” most challenging caregiving problems in the past two weeks.
Discussion
One of the most common and challenging problems cited by the family caregivers in this study was “managing other side effects and symptoms,” indicating that the cancer symptoms and treatment side effects previously believed to be most common and/or challenging to manage—patient pain, patient constipation, and patient shortness of breath—may indeed be less common or concerning to family caregivers of cancer patients receiving outpatient palliative care. However, it is not clear whether other side effects and symptoms were seemingly more common and problematic than managing patient pain, constipation, and shortness of breath because patients suffered from these problems less often, or because caregivers already felt sufficiently competent and well supported to handle these problems, as might be the case given that they were all receiving palliative care services. Nevertheless, palliative care teams should be mindful of not neglecting to address nausea/vomiting, loss of appetite, cognitive problems, and fatigue when discussing cancer patient problems with their family caregivers. In addition, although financial concerns were not among the mostly commonly reported problems overall, they had the highest prevalence among the top 3 recent problems, underscoring the need for substantial support for families struggling financially.
Consistent with the broad literature on family caregiving, caregiver worry and sadness were frequently cited problems. This finding was unsurprising, considering the high prevalence of anxiety and depression found among cancer caregivers, 11 yet its persistence despite study participants' receipt of palliative care suggests need for enhanced caregiver support in outpatient palliative care settings.
Study limitations
This study was limited by its small sample and the lack of diversity in the sample, including the fact that all participants were recruited from one cancer center. Because data were cross-sectional, we were not able to determine whether/how caregiver problems changed over time. The problem checklist measure utilized in this study was not a standardized instrument at the time of use, although it has been extensively used in family caregiving research,12,13 thus, other caregivers in this study may have also had those problems but neglected to identify them without a prompt.
Conclusion
The problems that family caregivers of cancer patients receiving outpatient palliative care face may differ from those experienced in other serious illness care contexts.
Footnotes
Authors' Contributions
Drs. Benson, Washington, and Kruse contributed to the conceptualization and analysis of the study. For the larger study from which these data were obtained, Drs. Washington, Demiris, and Parker Oliver contributed to the conceptualization, implementation, and data curation. Dr. Kruse performed the majority of analyses. Drs. Benson, Washington, Kruse, Parker Oliver, Rolbiecki, and Demiris participated in article writing.
Acknowledgments
The authors acknowledge the invaluable contributions of Diane Huneke, RN; Mary L. Cunningham, RN, AOCNS; Tammy Reeder, RN, BSN; Anna Hulbert, MD; and the family caregivers who generously volunteered their time to participate in this study.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the study's funder.
Funding Information
This study was supported by the National Cancer Institute Research Award Number R21CA191165 (Principal Investigator: Washington).
Author Disclosure Statement
The authors have no competing or personal financial interests to disclose. No organization will gain or lose financially from the publication of this article, nor will any recent, current, or anticipated employment by an organization.