
Abstract
Background:
Communication skills are crucial for personal support workers (PSWs) to foster therapeutic relationships with the residents and their families in the long-term care (LTC) setting.
Aim:
To evaluate the impact of the Communication at End-of-Life (CEoL) Education Program on the competency and confidence of PSWs working in LTC to communicate about palliative and end-of-life care, and factors affecting their involvement in palliative and end-of-life care.
Setting/Participants:
PSWs from 35 LTC homes in Ontario, Canada, who participated in the CEoL Education Program between January and March 2019.
Design:
Mixed-methods evaluation using pre- (n = 178) and post-workshop (n = 113) surveys capturing the attitudes and beliefs toward death and dying; relationships with residents and families; and PSWs' participation in end-of-life care. Follow-up interviews were conducted between February and March 2019 with 21 PSWs to examine facilitators and barriers that affected their confidence in engaging in palliative care.
Results:
We observed significant improvements in all three domains, with the greatest increase (11%, p < 0.001) in the proportion of participants who responded “Often” or “Always” in the participation in end-of-life care domain. Specifically, we observed PSWs' elevated confidence in speaking with families of the residents about end-of-life, discussing goals and plans with the residents, and realizing that a “good death” is possible. Time constraints and staff shortages were recurrent themes that hindered many participants' ability to provide resident-centered care.
Conclusions:
This evaluation demonstrates that CEoL Education Program was associated with improved PSW competency and confidence in supporting palliative and end-of-life care in LTC settings.
Background
The integration of palliative care into continuing education for nonpalliative care specialists and nonphysician providers 1 has the potential to expand the health care system's capacity to provide palliative care that are not limited to hospices and inpatient palliative care units.2,3 This is particularly important in long-term care (LTC). In Ontario, Canada, where this study is situated, the need for a palliative care approach in LTC homes (also known as nursing homes or LTC facilities in other countries such as United States) is increasing.4,5 The majority of residents in LTC homes, at the time of entry, are over the age of 85 years and have reduced life expectancy owing to the prevalence of multimorbidity and limited physical function.4,6 More recently, the importance of high-quality palliative and end-of-life care for frail elderly residents in LTC homes was accentuated by the devastating impact of the COVID-19 pandemic on this population.7,8
Typically, in Canada, palliative care for LTC residents at the end of their life is delivered by an interdisciplinary team of nonspecialist health care providers working in the LTC homes, including family physicians, nurses, personal support workers (PSWs), and other allied health professionals. 1 This is distinct from the delivery of hospice palliative care in U.S. nursing homes, where care for residents who are at the end of life may be provided in small hospice units within the home, where they are supported by nursing staff with specialized training in hospice palliative care, or it may be contracted out to home health agencies or independent community-based hospices. 9
Care provided by PSWs represent almost 60% of the total hours of care received by residents in Ontario's LTC homes, 10 and PSWs are often the first point of contact for residents and their families. 11 As a largely unregulated health care workforce, 12 there is wide variation in their titles, roles, and tasks across jurisdictions and health care settings. In some regions, PSWs may be known as health care aides, home support workers, and nursing aides. 13 While the scope of practice of PSWs have traditionally focused on assistance with activities of daily living (e.g., assistance with grooming, dressing, lifts and transfers, and personal hygiene), over time, their roles have shifted toward a greater involvement in providing emotional help to residents and delivering palliative care and end-of-life support.1,11,13,14 With this evolution, enhancing communication skills15–17 in PSWs is crucial to providing holistic care. Previous international evidence has shown that palliative or end-of-life care-related educational programs can effectively improve nursing assistants' application of palliative or end-of-life care skills and knowledge,18,19 and that communication is associated with improved end-of-life care delivery. 20 Despite the importance of PSWs' role in LTC residents' day-to-day care,15–17 they are often excluded from continuing education programs, which are often developed to target regulated health care providers such as physicians and nurses.1,16,21
In 2017, the Ontario Centers for Learning, Research, and Innovation (CLRI) in LTC at Bruyère collaborated with Algonquin College (a vocational school in Ontario) to develop and deliver a Communication at End-of-Life (CEoL) Education Program to improve PSWs' communication skills, awareness, and understanding pertaining to the provision of palliative and end-of-life care. The program covered concepts related to palliative care, which focuses on comfort and support care earlier in the dying trajectory, as well as end-of-life care (e.g., expectations for and management of pain and symptoms in the final weeks and days of life, dealing with grief and bereavement, etc.). This program was rolled out in two stages: the first stage (Wave 1) took a train-the-trainer approach delivering materials in two-day workshops to delegates from LTC homes across Ontario. The goal of Wave 1 is to augment capacity within the LTC sector to provide future training on how to engage in conversations about topics relevant to the end of life. Trainers were equipped with educational resources (e.g., facilitator guide and slides of modules) for delivering communication skills training to PSWs working with residents who have palliative care needs living in LTC. A summary of the training modules can be found in Supplementary Appendix Table S1 in Supplementary Appendix SA. A total of 257 trainers from 135 LTC homes were selected to participate in Wave 1 between September and October 2018. In the second stage (Wave 2), 35 LTC homes that completed Wave 1 training were supplied additional funding and 4 hours of structured coaching. The structured coaching comprised of individualized sessions to meet the needs of the trainers and their LTC homes. Following the receipt of structured coaching, the trainers then provided two-day workshops for PSWs in their LTC homes. A total of 783 PSWs participated in Wave 2 workshops provided by in-home trainers between January and March 2019.
The objectives of this evaluation were to assess PSWs' knowledge and confidence in delivering palliative and end-of-life care after their participation in the CEoL Education Program, and to identify factors that facilitated or hindered PSWs' capacity to engage in palliative and end-of-life care in LTC homes.
Materials and Methods
Ethics Approval
The study protocol (Bruyère REB # M16-19-003) was reviewed and determined by the Bruyère Research Ethics Board (REB) as constituting a program evaluation within normal educational requirements used exclusively for assessment, management, or improvement purposes, and did not constitute research for the purposes of the Tri-Council Policy Statement 2. Therefore, approval from the Bruyère REB was not required.
Study design and setting
In this evaluation, we undertook a mixed-methods approach using pre/post surveys administered to participants in the Wave 2 program (between January and March 2019) followed by one-on-one interviews with PSWs from different LTC homes across Ontario who received training.
Data collection
Pre/post workshop surveys
The surveys were developed based on a literature review of practice guidelines pertaining to communications at the end-of-life,22–25 which captured the domains of: (1) attitudes and beliefs toward death and dying,23,25 (2) relationships with families and residents, 25 and (3) active participation in end-of-life care.22,25 The concepts captured within each domain can be found in Supplementary Appendix Table S2 in Supplementary Appendix SA. The survey was given to participants by the in-home trainers before and within four to six weeks of their completion of the Wave 2 workshop to assess the immediate change associated with their training. The statements presented in the survey were scored on Likert scales ranging from “Never” to “Always.”
One-on-one interviews
One-on-one semistructured interviews were conducted by one of the study's female authors (A.H.S.), who was a research assistant with the Ontario CLRI at Bruyère, between February and March 2019. The interviewer did not have preexisting relationships with the recruited interviewees. The semistructured interview guide (Supplementary Appendix SB) was developed based on themes identified in previous studies on PSWs' involvement in palliative and end-of-life care.11,26–28
In addition to the semistructured interview, a questionnaire capturing select sociodemographic characteristics (e.g., age, sex, and education) and prior training in palliative care was administered to the interviewees (Supplementary Appendix SC).
Participant recruitment
We used a purposive sampling approach to select interviewees from Wave 2 LTC homes from across Ontario, and ensured that any geography-related barriers and benefits (e.g., access to other training opportunities or resources) would be reflected in our evaluation. We considered the following characteristics when selecting the homes: facility size (small: <98 beds, medium: 99–159 beds, large: >160 beds); home ownership type (for-profit, not-for-profit, or municipal/government owned); and location (rural or urban). The recruitment process began with an initial e-mail sent to the administrators of these homes, outlining the purpose and estimated duration of the interviews, and the number of PSWs we intended to recruit. Six LTC homes consented to participate in our evaluation. Unfortunately, interviews could not be completed at one prospective location due to an unexpected gastrointestinal disease outbreak during the study period. In the end, a total of 21 PSWs from 5 LTC homes were interviewed. Among the five participating homes, one was considered as small, two were medium sized, and the remaining two were large facilities. Three operated under not-for-profit ownerships, one home was municipal/government owned and one was for-profit. Interviews were conducted at participants' LTC home; interviewees were informed that the conversation would be audiorecorded and verbal consent was obtained. At the beginning of each interview, participants were informed of the role and workplace of the interviewer, purpose, process, and estimated duration of the interview. The duration of interviews ranged from 30 to 50 minutes.
Statistical and qualitative analyses
Quantitative data were analyzed descriptively and presented as means, standard deviation, frequencies, and proportions (specifically, to describe changes in the responses between the pre- and post-workshop surveys). In addition, we performed chi-square tests to determine whether responses between pre- and post-workshop surveys were statistically significant, which was set at p < 0.05. All quantitative analyses were performed in R Studio Version 1.3.959. 29
For qualitative analyses, we conducted an inductive content analysis of the audiorecorded interviews30,31 and followed the reporting guidelines of the COnsolidated criteria for REporting Qualitative research (COREQ). One of the study's authors (A.H.S.) led the analysis by, first, condensing audio recordings into meaningful units such as words, phrases, or sentences and identified key codes inductively. We analyzed the manifested content without interpreting the latent intentions of the recording and transcribed text. 30 Then, two of the study's investigators (A.H.S and A.T.H.) sorted and grouped the codes into major themes based on the frequency of their reoccurrence in the interview recording.30,32
Results
The pre/post workshop surveys
Of the 783 PSWs who completed Wave 2 training, 178 preworkshop (23%) and 113 post-workshop (15%) surveys were completed. Figure 1 summarizes the proportion of participants who had responded “Often” or “Always” to questions in each of the three domains before their training and the percentage point increase in these responses following Wave 2 training. We observed statistically significant improvements in all the three domains, with the largest increase in the domain of active participation in end-of-life care, where there was a 11% (p < 0.001) increase in the proportion of participants who responded “Often” or “Always” to statements in this domain. This was followed by a 10% increase (p < 0.001) in building therapeutic relationships with families and residents and a 7% increase (p < 0.001) toward a more open attitude about death and dying.

Percent of PSWs who responded “Often” or “Always” in each domain† in the preworkshop survey and the percentage point increase in these responses in the post-workshop survey. * Denotes statistical significance at p < 0.05. † An exception to this was made for the statement “I feel guilty if a resident dies when I am involved in caring for them,” where an increase in the proportion of participants who responded “Rarely” or “Never” was coded as an indication of improvement. PSW, personal support worker.
Attitudes, beliefs, and personal thoughts on death and dying
As shown in Figure 2, after the receipt of training, the most notable increase was observed in the statement regarding the possibility of having a “good death” in LTC (16%, p = 0.003). This was followed by an increase of 11% of respondents who felt that they were more comfortable showing their feelings at work after a resident had died. However, this change was not statistically significant (p = 0.06). We did not find a statistically significant change in the remaining five statements, although improvements were noted in all.

Percent of PSWs who responded “Often” or “Always” to questions† related to the domain of attitudes, beliefs, and personal thoughts on death and dying in the preworkshop survey and the percentage point increase in these responses in the post-workshop survey. * Denotes statistical significance at p < 0.05. † An exception to this was made for the statement “I feel guilty if a resident dies when I am involved in caring for them,” where an increase in the proportion of participants who responded “Rarely” or “Never” was coded as an indication of improvement. PSW, personal support worker.
Ability to establish relationship with residents and families
Figure 3 presents results from the domain of relationships with families and residents. We observed statistically significant improvements in PSWs' confidence in speaking with the residents' families about end-of-life (21%, p < 0.001), ability to communicate with the residents and families in a manner that builds a therapeutic relationship (12%, p = 0.02), and comfort in being direct with residents when talking about the end of life (12%, p = 0.03). Before their training, PSWs were more confident in speaking with residents (69%) than speaking with family members (<50%) about end-of-life care. After their training, this gap narrowed (to 79% and 65%, respectively). The percentage of respondents who reported that they were “Often” or “Always” approached by families and residents to talk about end-of-life care decreased, but not significantly (1%, p = 0.90), when they were surveyed four to six weeks after the workshop.
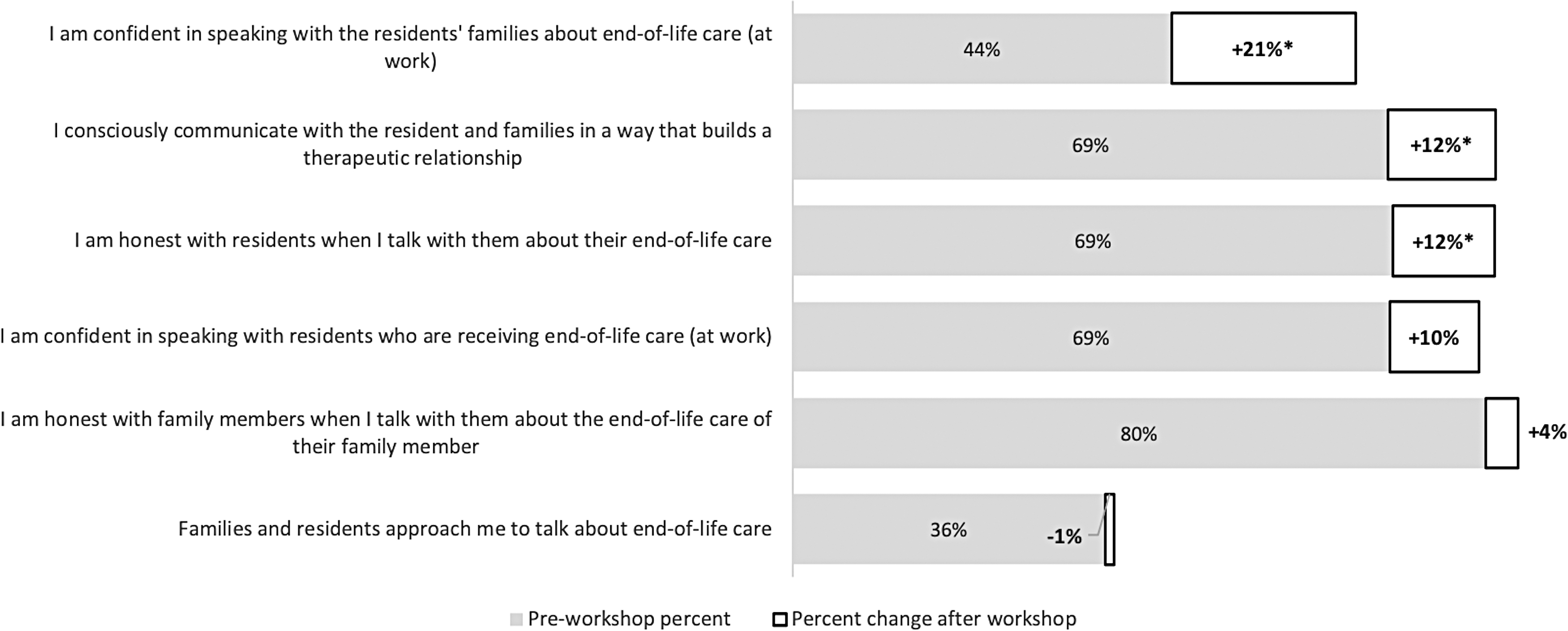
Percent of PSWs who responded “Often” or “Always” to questions related to the domain of establishing a therapeutic relationship with families and residents at the end-of-life in the preworkshop survey and the percentage point increase in these responses in the post-workshop survey. * Denotes statistical significance at p < 0.05. PSW, personal support worker.
Participation in end-of-life care
Finally, in the domain of active participation in end-of-life care (Fig. 4), the most prominent increase was observed in the PSWs' confidence in discussing goals and plans with residents and families about end-of-life care (25%, p < 0.001). The proportion of PSWs who felt that they “Often” or “Always” knew what to do when a resident has died also increased, by 14% (p = 0.004). We also observed increased agreement with statements pertaining to the PSWs' confidence in meeting the physical needs of residents at the end of life (4%, p = 0.39) and whether they would want to be on duty when a resident they are caring for dies (2%, p = 0.68). However, these improvements were not statistically significant.

Percent of PSWs who responded “Often” or “Always” to questions related to the domain of participation in end-of-life care in the preworkshop survey and the percentage point increase in these responses in the post-workshop survey. * Denotes statistical significance at p < 0.05. PSW, personal support worker.
Perceived barriers and facilitators to providing palliative and end-of-life care
Participants' characteristics
A total of 21 PSWs who received Wave 2 training participated in our follow-up interview; their age ranged between 24 and 64 years (Table 1). Only 2 of the 21 (9.5%) participants were male. Most PSWs (85.7%) received their training outside of Canada. Based on their years of work experience, the majority have been working in the LTC sector for most of their health care career, with an average time working in health care being 14.6 ± 8.0 years and time in LTC being 13.4 ± 7.3 years. In terms of education level, 47.6% of participants had a bachelor's degree (mostly received from their country of origin), followed by participants who received a nonuniversity certificate or diploma from a community college or vocational school (33.3%).
Sociodemographic Characteristics of the Participants
CEGEP, collège d'enseignement général et professionnel; SD, standard deviation.
Findings from the semistructured interviews highlighted several challenges and facilitators to the PSWs' role in providing palliative and end-of-life care in an LTC home.
Theme 1: feeling time constraint and staff shortage
Time and staffing shortages were a recurrent theme identified by almost all participants. Many PSWs have cited time and staffing shortage as a notable challenge to providing good palliative and end-of-life care in LTC homes:
I guess we don't have enough staff, sometimes. You wanna spend time with the residents. You wanna sit down and, you know, just make sure they are comfortable and well taken care of. You don't have the staff sometimes so it's like a rush-rush. And then you feel bad because you just want to make sure that the resident is one hundred percent taken care of. (Interview 9, a PSW from a large, urban for-profit LTC home)
Theme 2: difficulty communicating with family members
While none of the participants felt uncomfortable providing care to residents, some expressed discomfort in working with the family members of residents in their care. For example, several participants stated that family members sometimes found it hard to accept the resident was dying:
Sometimes the family doesn't accept the fact that the resident is dying—they could be in denial. [I find it challenging] to actually talk to them sometimes… to help them understand what's going on, to help them with what is happening. (Interview 11, a PSW from a small, urban not-for-profit LTC home)
PSWs also found it challenging to communicate with some family members to help them understand what was happening to the residents:
You not only have to deal with the dying person, but you have to deal with the relatives—the family members … your relationship with the resident is different from that with the [family]. I may feel closer to the resident, but not with their family. (Interview 12, a PSW from a small, urban not-for-profit LTC home)
Theme 3: need of raise in cultural sensitivity and awareness
The need to enhance cultural sensitivity and awareness was cited by some participants, who expressed that a deeper understanding of the residents' culture could enable them to build better relationships with residents and family members and remain unbiased even when the beliefs and cultures of patients were different from their own. For example, from interviews conducted in homes where a large proportion of the residents belonged to an ethnic minority or indigenous populations, participants expressed their difficulty in providing better palliative and end-of-life care due to a language barrier:
I had one resident I was actually working when he passed away … I think he could have benefited from a palliative care approach if we had someone who actually spoke his language. Since he was Cree—he was from Moosonee or Moose Factory—but it was really hard to see if he was in pain or [know] what he wanted, because I don't speak Cree. I don't understand it … He just screamed and grabbed onto you, and spoke to you in Cree. But, you didn't know. We had little pictures of water, food and [to ask] if he had to go to the bathroom … but with him having dementia—some type dementia or Alzheimer's—was he comprehending what we were saying? We don't know. But, [good palliative care was provided] to the best that we could, with the resources and information that we had. (Interview 20, a PSW from a large, rural municipal LTC home)
Theme 4: lack of grief counseling
While many of the PSWs recognized the importance of meeting the physical, spiritual, emotional, and social needs of the residents, they also expressed a lack of grief counseling for staff in their work place. Some PSWs expressed difficulty helping family members through the bereavement process while dealing with their own grief when residents die. As a result, some PSWs expressed feeling sad or emotionally exhausted when a resident has died:
You cannot control your emotions when dealing with people who are dying, and that is the hardest part … Every death is different. When the person dies, you could be grieving outwards, and sometimes it's just inwards. (Interview 12, a PSW from a small, urban not-for-profit LTC home)
Theme 5: access to palliative care resources and additional training
The level of support from team members and resources within the LTC homes can also affect PSWs' level of comfort in providing palliative and end-of-life care. For example, some LTC homes have created palliative care boxes containing supplies to support the personal needs of family members and care tools for the residents, which the PSWs found to be helpful. Additionally, among many of our interview participants, support from their coworkers when providing palliative and end-of-life care was instrumental:
The teamwork is good. We know if someone forgot [to perform a task], “Oh, we didn't reposition her. Did you do it?” We communicate. (Interview 3, a PSW from a medium, urban non-for-profit LTC home)
Many of the participating PSWs were able to recognize signs of residents being at the end of life. Participants noted health changes and functional decline as part of palliative care approaches to help identify needs early on. For example, some noted observable changes in physiology (e.g., skin color, breathing, fingers turning blue, toes turning black, weight loss), loss of appetite, reduced level of energy, lack of communication or “whispering words,” and depressive moods. Despite this, many PSWs expressed that further guidance on when palliative care should be initiated, specifically, clarification on the distinction between palliative and end-of-life care (in the form of care protocols or policies) could help them identify when they should start to more actively engage in conversations about the goals of care at the end of life. Furthermore, participants who are internationally educated nurses but were working as PSWs in Canada were more likely to express an interest in additional training in clinical aspects to increase their capacity to provide palliative care.
Discussion
Main findings
This study demonstrated that PSWs working in LTC homes were more confident and comfortable engaging in palliative and end-of-life care approaches after receiving training from the CEoL Education Program. Specifically, more PSWs believed that achieving a “good death” is possible; felt comfortable speaking with residents about the end-of-life; and were able to confidently discuss goals of care and advanced plans with residents and families. These observations are consistent with prior studies examining the effectiveness of educational end-of-life communication interventions for health care professionals.20,33
Notwithstanding these positive observations, our follow-up interviews with the participants revealed several challenges to PSWs' capacity to apply their learning in their current environment. One of the foremost challenges to providing good quality of palliative and end-of-life care is the shortage of staff in LTC homes, which limits the amount of time that each PSW may be able to spend with a dying resident. Other studies also found that time constraint affects PSWs' capacity to provide more resident-centered care. 11
Many participating PSWs expressed a desire to gain more clinical content knowledge, which they believe could empower them to be more comfortable with identifying LTC residents who might need palliative and end-of-life care. This highlights a potential opportunity for the inclusion of more basic clinical content in future curriculum development targeting PSWs. Additionally, many PSWs expressed that they could benefit from more frequent training to maintain their knowledge and skills. With a train-the-trainer model, there may be opportunities within LTC for self-propagation and further communication at the end-of-life education provided by the trainers who have completed Wave 1 of the program.
Finally, there is evidence indicating that cost is a major barrier for unregulated health care workers to access educational programs. 16 Often, PSWs receive less professional or accredited training compared with registered nurses, which may have contributed to the perception that PSWs are ill prepared and lacked the knowledge or skills to support LTC residents at end of life. 1 In 2014, the Government of Ontario released a report outlining the proposal for a standardized PSW training curriculum, in which communicating effectively to develop relationships with patients and their families during routine care is a required competency. 34 Findings of this study demonstrated the CLRIs CEoL Education Program aligns well with the movement toward standardizing the PSW training provincially and internationally.3,34–37
Strengths and limitations
This evaluation has some limitations. First, we used a purposive sampling method to select interviewees among Wave 2 participants. This may expose our evaluation to the risk of selection bias. While there may be misgivings in using this approach, we found it was more realistic in the LTC setting, where there are irregular workflows, and allowed us to interview PSWs without interfering with the activities in the LTC home. 38 Second, we acknowledge that our approach using inductive content analysis may have limited external validity. 39 Unfortunately, as both pre- and post-workshop surveys were completed anonymously by participants, we were unable to link each participant's responses to examine pre/post changes at the individual level. Finally, the response rates for both pre- (23%), and post-surveys (15%) were low. This may be attributed to two possible reasons: first, survey response rates for multisite studies tend to be lower than single-site study. This has been observed in similar evaluations of educational programs for LTC staff.40,41 Second, the completion of these surveys was not mandatory for the LTC homes' participation in the training program.
Despite these limitations, our study is strengthened by the mixed-methods approach to further understand barriers that PSWs may encounter in applying the knowledge and skills they had gained from the program. In future evaluation, we aim to expand the perspectives captured, to include the experiences of the palliative care trainers and LTC home administrators in implementing palliative care approaches in LTC homes.
Conclusions
Findings from this evaluation demonstrated that Ontario CLRIs CEoL Education Program improved PSWs' confidence and competency in their communication regarding palliative and end-of-life care with residents and their families in LTC homes.
Footnotes
Authors' Contributions
Study concept and funding: Z.O. and A.T.H. Study design: M.C. and A.T.H. Data acquisition: M.C., Z.O., and A.H.S. Data analysis and interpretation: A.H.S. and A.T.H. Article drafting and revising: all authors. Final approval to publish was obtained from all authors.
Acknowledgments
The author(s) would like to acknowledge the contributions of the long-term care homes that participated in the evaluation. This research would not have been possible without the palliative care champions within long-term care who participated in the Communication at End-of-Life Program, as well as all the team members within long-term care homes who are committed to high-quality palliative and end-of-life care.
Funding Information
This work was supported by the Government of Ontario through the Ontario Centers for Learning, Research, and Innovation in Long-term Care at Bruyère and through the Communications at the End-of-Life Training Fund for long-term care.
Author Disclosure Statement
The author(s) declared no competing interests. M.C. completed this work during her employment with the Ontario Centers for Learning, Research, and Innovation in Long-Term Care at Bruyère. She is now employed at the Canadian Foundation for Healthcare Improvement (CFHI), and CFHI has no role in the study funding, design, or the oversight of this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.