
Abstract
Background:
Pain from advanced cancer can greatly reduce patients' physical, emotional, and spiritual well-being.
Objective:
To examine the feasibility and acceptability of a behavioral pain management intervention, Meaning-Centered Pain Coping Skills Training (MCPC).
Design:
This trial used a single-arm feasibility design.
Setting/Subjects:
Thirty participants with stage IV solid tumor cancer, moderate-to-severe pain, and clinically elevated distress were enrolled from a tertiary cancer center in the United States. The manualized protocol was delivered across four 45- to 60-minute videoconference sessions.
Measurements:
Feasibility and acceptability were assessed through accrual, session/assessment completion, intervention satisfaction, and coping skills usage. Participants completed validated measures of primary outcomes (i.e., pain severity, pain interference, and spiritual well-being) and secondary outcomes at baseline, post-intervention, and four-week follow-up.
Results:
Eighty-eight percent (38/43) of patients who completed screening met inclusion criteria, and 79% (30/38) consented and completed baseline assessment. Sixty-seven percent (20/30) of participants were female (mean age = 57). Most participants were White/Caucasian (77%; 23/30) or Black/African American (17%; 5/30) with at least some college education (90%; 27/30). Completion rates for intervention sessions and both post-intervention assessments were 90% (27/30), 87% (26/30), and 77% (23/30), respectively. At the post-intervention assessment, participants reported a high degree of intervention satisfaction (mean = 3.53/4.00; SD = 0.46), and 81% (21/26) reported weekly use of coping skills that they learned. Participants also showed improvement from baseline on all primary outcomes and nearly all secondary outcomes at both post-intervention assessments.
Conclusions:
MCPC demonstrated strong feasibility and acceptability. Findings warrant further evaluation of MCPC in a randomized controlled trial. ClinicalTrials.gov Identifier: NCT03207360
Introduction
Pain is a prevalent and debilitating symptom in patients with advanced cancer. 1 Nearly two-thirds of patients experience pain, 2 and many report suboptimal pain control. 3 Higher pain levels are consistently associated with worse physical, emotional, and spiritual well-being.4,5 Unfortunately, optimal pain management for patients with advanced cancer can be complicated by existential concerns that are heighted when facing life-threatening illness.6,7
One of the most salient existential concerns for patients with advanced cancer is maintaining a sense of meaning.8,9 A sense of meaning is a core facet of existential and spiritual well-being and is defined as the degree to which a person believes that their life has worth, significance, and coherence.10,11 Meaning-making theories12,13 and previous research with medical populations14–16 suggest that persistent pain is especially debilitating since it often reduces a patient's sense of meaning. Poorly controlled pain can negatively impact a patient's sense of meaning in multiple ways, such as disrupting roles and responsibilities, interfering with valued activities (e.g., time with family), and increasing feelings of hopelessness about the future. A sense of meaning is notable because it is a facet of spiritual well-being that is relevant to religious and nonreligious patients and, importantly, is amenable to intervention. 17
Multiple clinical trials with patients with cancer have tested psychosocial interventions that address spiritual and existential concerns.17,18 One of the most efficacious approaches is Meaning-Centered Psychotherapy. 19 Developed by Breitbart 20 and inspired by Viktor Frankl's seminal work, 21 Meaning-Centered Psychotherapy aims to help patients with advanced cancer enhance their sense of meaning. This approach entails education on sources of meaning (e.g., historical, attitudinal, creative) and experiential exercises that assist patients in identifying and connecting with meaning in their lives. 19 Four randomized controlled trials (RCTs) support the efficacy of Meaning-Centered Psychotherapy for increasing patients' sense of meaning 22 and overall spiritual well-being and reducing their depressive symptoms, hopelessness, and desire for hastened death.23–26 However, similar to other existentially-focused interventions, 17 Meaning-Centered Psychotherapy does not address skills for coping with pain.
The Institute of Medicine report 27 and American Pain Society guidelines for cancer pain 28 recommend that psychosocial interventions to enhance pain coping be routinely utilized. Cognitive-Behavioral Therapy (CBT) is one of the most well studied approaches; meta-analyses of over 20 RCTs support the efficacy of CBT-based interventions for reducing cancer pain severity, pain interference, and psychological distress.29–31 One CBT-based approach is Pain Coping Skills Training,32–34 which involves systematically teaching patients skills (e.g., guided imagery) to improve pain-related thoughts, emotions, and behaviors. 35 This approach is informed by Social Cognitive Theory,36,37 such that it emphasizes modeling, guided skill practice, and mastery experiences to increase patients' self-efficacy (i.e., confidence) for coping with pain. 38 A key focus is on practicing learned skills in social situations and other contexts where pain is problematic. Pain Coping Skills Training can reduce cancer pain,29,32 but it does not address existential concerns that are common in patients with life-threatening illness.
To address pain and associated existential concerns in patients with advanced cancer, we recently developed an integration of Meaning-Centered Psychotherapy and Pain Coping Skills Training. This novel approach, called Meaning-Centered Pain Coping Skills Training (MCPC), seeks to enhance patients' sense of meaning while systematically teaching them CBT-based pain management skills. In a preliminary qualitative study, 39 we conducted in-depth interviews with 12 patients with advanced cancer and pain to refine the protocol. After reviewing MCPC's session content, participants described how it resonated with their experience. Specifically, many participants coped with their pain and poor prognosis by relying on frameworks (e.g., spiritual beliefs) that provided them with a sense of meaning. They also expressed interest in learning skills to cope with their pain and some suggested adding additional skills (e.g., problem solving). Nearly all participants described concerns about attending in-person intervention sessions, primarily due to travel difficulties. We refined the manualized protocol based on these suggestions and chose to deliver the intervention using secure videoconferencing technology.
The next phase in our development of MCPC was to test the feasibility and acceptability of the protocol in a sample of patients with advanced cancer. In this study, we used a single-arm clinical trial design to initially test the protocol and inform future randomized trials. Participants completed validated self-report measures of primary outcomes (i.e., pain severity, pain interference [i.e., disruption in activities and mood due to pain], and spiritual well-being [i.e., meaning, peace, and faith]) and secondary outcomes (i.e., anxiety symptoms, depressive symptoms, hopelessness, fatigue, meaningfulness despite pain [i.e., finding life meaningful even when experiencing pain], and quality of life) at baseline, post-intervention, and four-week follow-up. Feasibility and acceptability were assessed using benchmarks established a priori for study accrual, session and assessment completion, intervention satisfaction, and coping skill usage. Changes in primary and secondary outcomes were explored.
Methods
Participants
Participant eligibility criteria included: (1) stage IV solid tumor cancer diagnosis, or stage III pancreatic or lung cancer diagnosis; (2) at least moderate pain (worst pain severity in past week ≥4/10) at screening 40 ; (3) clinically elevated distress (distress thermometer ≥3/10) at screening 41 ; (4) Eastern Cooperative Oncology Group (ECOG) score ≤2 at screening; (5) ability to speak and read in English; and (6) age ≥18 years. Exclusion criteria included: (1) significant cognitive impairment; (2) untreated serious mental illness; and (3) patients with primary brain tumors. All participants provided written informed consent.
Procedures
The Duke University Institutional Review Board approved this study (IRB number: Pro00083582; ClinicalTrials.gov: NCT03207360). Participants were recruited between November 2018 and November 2019 from the Duke Cancer Institute in Durham, NC. The study team determined initial eligibility through electronic medical record review and, following provider approval, mailed study recruitment letters. Patients were called for eligibility screening. Interested and eligible patients were scheduled for an in-person meeting to complete informed consent. Participants were given session handouts and loaned a tablet computer for completing assessments and intervention sessions through Skype with 256-bit encryption. Assessments were completed using REDCap 42 at baseline, post-intervention, and four-week follow-up. Participants were compensated $20 per assessment.
Measures
Demographics and medical characteristics
Study staff collected basic demographic and medical information from participants' medical records. At baseline, participants reported additional demographics (e.g., religious preference), cancer treatment history, and pain medication usage.
Feasibility and acceptability
We specified a priori benchmarks for treatment feasibility and acceptability informed by previous psychosocial intervention trials.32,33,43 Benchmarks for feasibility included: (1) reaching target accrual (N = 30) within the 24-month study period and (2) <30% study attrition, defined as the percentage of participants who completed the post-intervention assessment (primary end point). Benchmarks for acceptability included: (1) ≥80% of participants reporting intervention satisfaction (i.e., Client Satisfaction Questionnaire 44 mean ≥ 3.00/4.00) and (2) ≥75% of participants reporting use of coping skills or ideas from the intervention. 32
Primary outcome measures
All outcome measures have previously shown evidence of strong psychometric properties (see citations for information on reliability and validity). Pain severity and pain interference were assessed with the Brief Pain Inventory-Short Form; four items assessed the severity of pain, and seven items assessed the degree to which pain interfered with activities and mood. 45 Spiritual well-being was assessed with the 12-item Functional Assessment of Cancer Therapy—Spiritual Well-Being scale, which includes three subscales: meaning, peace, and faith.46,47
Secondary outcome measures
Pain self-efficacy was assessed with the five-item Chronic Pain Self-Efficacy Scale. 48 Anxiety symptoms were assessed with the seven-item Generalized Anxiety Disorders scale. 49 Depressive symptoms were assessed with the eight-item Patient Health Questionnaire. 50 Hopelessness was assessed with the eight-item Hopelessness Assessment in Illness Questionnaire. 51 Fatigue was assessed with the four-item Fatigue Symptom Inventory. 52 Meaningfulness despite pain was assessed with a subscale from the Pain Solutions Questionnaire. 53 Health-related quality of life was assessed with the 16-item McGill Quality of Life Questionnaire, which includes four subscales: physical, psychological, existential, and social well-being. 54
Intervention
A PhD-level clinical psychologist skilled in behavioral symptom management delivered the manualized protocol over four 45- to 60-minute videoconference sessions. An overview of study sessions is presented in Table 1.
Meaning-Centered Pain Coping Skills Training Session Topics
Session 1
The session began with the therapist building rapport and gathering information about the participant's cancer and pain. Next, the therapist shared with the participant a definition of meaning (i.e., worth, significance, and coherence) and collaboratively explored how cancer and pain can impact meaning.10,11,19 Using the neuromatrix theory of pain, 55 the therapist discussed with the participant how thoughts, emotions, and behaviors can influence pain. The rationale for guided imagery was introduced and emphasized fostering distraction, relaxation, and the reexperiencing of meaningful moments. The therapist led an imagery practice and then asked the participant about any impact of the imagery on thoughts or emotions related to meaning or pain. Home practice included using guided imagery three to four times. Participants were also asked to write about a time when they felt most alive and connected to life (i.e., a meaningful moment). 19
Session 2
The therapist reviewed the participant's response to the meaningful moment question and then reviewed, reinforced, and problem solved around the participant's imagery practice. Common sources of meaning were then discussed, including connecting with life through love, relationships, beauty, art, nature, and humor. 19 The therapist led an exercise to help the participant identify and schedule two meaningful activities (e.g., visiting a friend) or experiences (e.g., savoring a sunset). The therapist then presented activity-rest cycling as a skill that helps patients build up their tolerance for and engagement in meaningful activities. To learn this skill, the participant was asked to select an activity/experience they find meaningful. Working collaboratively, time limits were set for periods of activity and rest. Over time, the length of activity periods was gradually increased and rest periods reduced. Activity-rest cycling enables patients to build up activities in a way that reduces the likelihood that activities will lead to extreme pain. Home practice included use of imagery, two meaningful activities/experiences, and at least two uses of activity-rest cycling.
Session 3
After reviewing home practice, the therapist led a discussion on suffering (physical, emotional, and spiritual) and responding to limitations. 19 The participant was encouraged to consider how cancer and pain caused suffering in their life. The therapist then explored how unhelpful thoughts can increase suffering because they negatively impact emotions, behaviors, and pain. 35 The therapist worked collaboratively with the participant to develop coping statements to use when they identify unhelpful thoughts or experience increased pain. Specifically, the participant was asked to remember a time when they were brave, took control of things, or made a commitment to something they cared about. 19 A coping statement was developed that drew on the thoughts they had in that situation. Following, the therapist trained the participant in how to use brief relaxation practices (e.g., 30 second muscle scan) to keep pain and muscle tension at lower levels throughout the day. Home practice included continued use of previous skills, coping statements, and five brief relaxation practices per day.
Session 4
The final session began with a brief relaxation practice and then homework practice review. The therapist guided a discussion on the idea of a living legacy, one that has a past, present, and future. 19 The participant was asked to reflect on what aspects of life (e.g., values, traditions) impacted who they are today and what will endure beyond their lifetime. Building on this discussion, the therapist introduced value-based goal setting. Working collaboratively, a value-based goal was set for the upcoming week. Problem solving was then presented as the final coping skill. The participant identified a current pain-related concern and was then guided through problem solving steps (i.e., problem identification, brainstorming solutions, and selecting an approach) that emphasize autonomy. Maintenance of coping skill practice was discussed, and the participant was encouraged to continue pursuing what brings their life meaning.
Analysis
Descriptive statistics were calculated using the statistics program SPSS Version 26. 56 Paired samples t tests were computed to explore changes in outcomes using the R Project based program JASP. 57 Cohen's d was used to quantify the magnitude of change. 58 Because this was a small feasibility study, p-values were not reported and effect sizes were solely exploratory.
Results
Study flow
The study flow is presented in Figure 1. The study team mailed recruitment letters to 98 patients, of whom 56% (55/98) were excluded before completing screening because they could not be contacted through phone (11%; 11/98), were found to be ineligible (18%; 18/98), or declined participation (27%; 26/98). Primary reasons for declining participation were lack of interest (n = 9) or feeling too sick (n = 8). Only four patients declined because of technology concerns. Sixty-two percent (43/69) of potentially eligible patients who could be contacted agreed to screening. Eighty-eight percent (38/43) of those screened met inclusion criteria, and 82% (31/38) consented for participation. One consented participant withdrew before baseline.
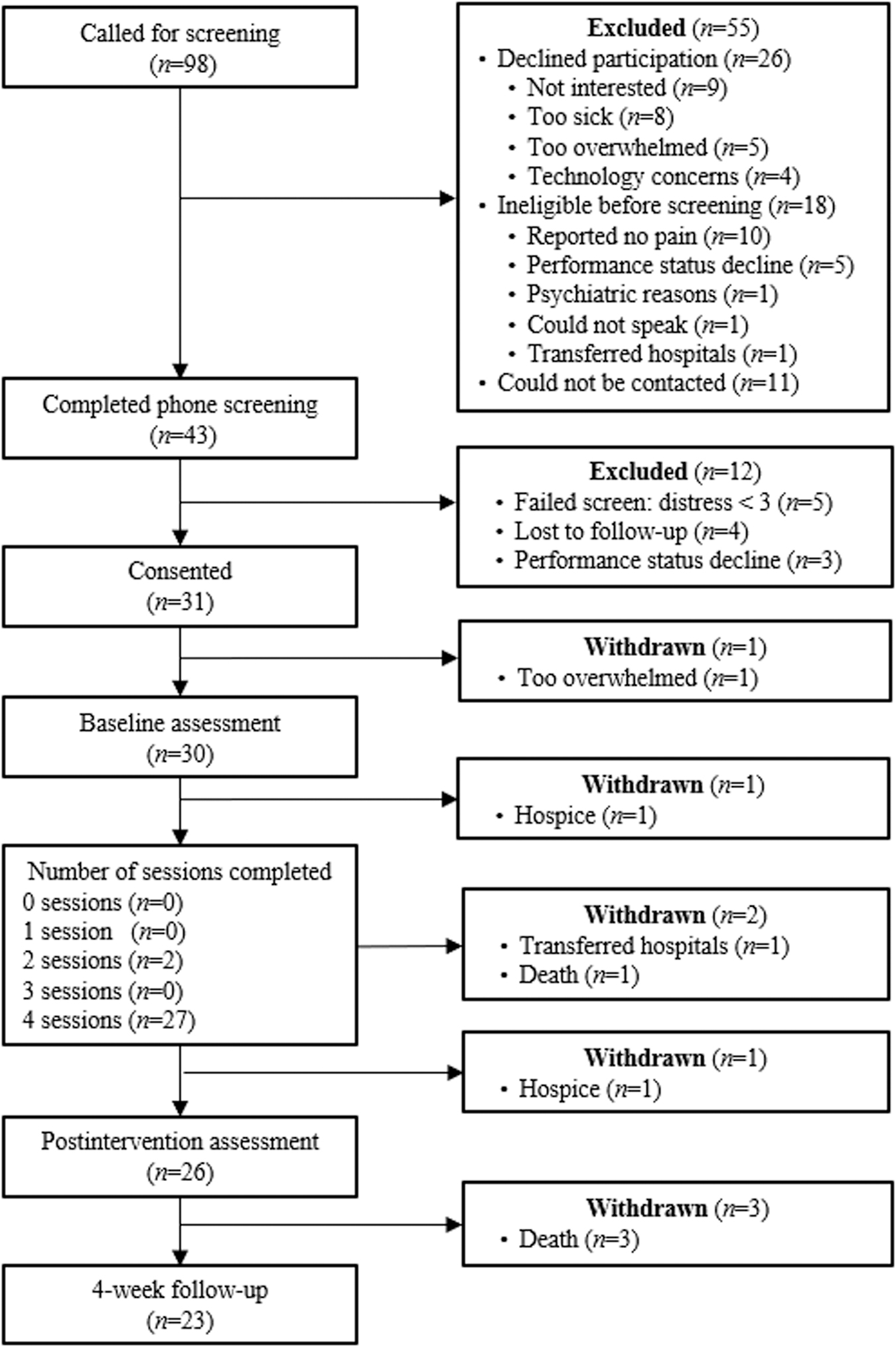
Study flow diagram.
Participant characteristics
Participant (N = 30) characteristics are presented in Table 2. Sixty-seven percent of participants were female (mean age = 57, SD = 9). Participants identified as non-Hispanic (90%; 10% declined response) and White or Caucasian (77%), Black or African American (17%), American Indian (3%), or declined response (3%), and most had some college education (90%). The most common cancer types were gastrointestinal (37%), breast (23%), and lung (23%).
Baseline Demographic and Medical Characteristics (N = 30)
Cancer type, stage, and years since diagnosis were determined based on medical record review. All enrolled patients had an oncologist confirmed diagnosis of stage IV solid tumor cancer based on American Joint Committee on Cancer (AJCC) and Union for International Cancer Control (UICC) tumor (T), nodes (N), and metastases (M) classification.
ECOG, Eastern Cooperative Oncology Group.
Feasibility and acceptability
The intervention met all feasibility and acceptability benchmarks. The accrual goal (N = 30) was reached after 12 months of recruitment, ahead of the 24-month study period. Retention was high and surpassed the goal of <30% attrition by post-intervention; specifically, 90% (27/30) of participants completed all four sessions, 87% (26/30) completed post-intervention assessment, and 77% (23/30) completed the four-week follow-up. Sessions were an average of 50 minutes long (SD = 5.39) and completed within four weeks (SD = 1.41).
Intervention satisfaction ratings are presented in Table 3. Participants reported a high degree of satisfaction (mean = 3.53/4.00, SD = 0.46). Ninety-two percent (24/26) reported an average satisfaction score ≥3.00, exceeding our benchmark of 80% satisfaction. At post-intervention, 81% (21/26) reported using the skills and/or ideas from the intervention “several days” (58%; 15/26) or “almost every day” (23%; 6/26), exceeding our benchmark of ≥75% reporting skills/idea usage.
Intervention Acceptability (n = 26)
Items were modified to specifically reference pain, and two questions were added regarding understanding of pain and coping skills. Items were rated on a scale from 1 to 4, with higher scores signifying greater satisfaction. Responses of 3 (e.g., good) or 4 (e.g., excellent) were considered satisfactory responses.
Changes in outcomes
Scores on outcome measures are presented in Table 4. Participants reported improvement from baseline to post-intervention on all primary outcomes (5/5), including pain severity (d = −0.39, confidence interval [95% CI]: −0.79 to 0.01), pain interference (d = −0.43, 95% CI: −0.82 to −0.02), and spiritual well-being subscales of meaning (d = 0.21, 95% CI: −0.19 to 0.62), peace (d = 1.00, 95% CI: 0.50 to 1.49), and faith (d = 1.07, 95% CI: 0.56 to 1.57). Effect sizes ranged from small to large in magnitude. Nearly all secondary outcomes (9/10) improved from baseline to post-intervention, with effect sizes ranging from small to moderate. One exception was meaningfulness despite pain, which worsened from baseline to post-intervention (d = −0.22, 95% CI: −0.61 to 0.17) but improved from baseline to four-week follow-up (d = 0.23, 95% CI: −0.19 to 0.64). Social and physical well-being slightly worsened from baseline to four-week follow-up (d = −0.09, 95% CI: −0.51 to 0.33; and d = −0.02, 95% CI: −0.43 to 0.39, respectively). All other outcomes (13/15) improved from baseline to four-week follow-up, although effects were generally smaller than those from baseline to post-intervention.
Outcome Measures Overtime
Post = immediately post-intervention. Follow-up = four-weeks post-intervention. t = t-value from paired sample t test. d = Cohen's d, quantified using benchmarks of small (≤0.49), medium (0.50–0.79), and large (≥0.80) effects. Variation in sample size due to missing data. Higher scores reflect more of each construct.
CI, confidence interval.
Discussion
In this study we examined the feasibility and acceptability of MCPC, a psychosocial intervention for patients with advanced cancer and pain. To our knowledge, MCPC is the first behavioral cancer pain intervention protocol to address patients' sense of meaning. MCPC exceeded a priori benchmarks for feasibility and acceptability, and exploratory estimates suggest that participants improved from baseline on most outcomes. These promising findings support the continued evaluation of this intervention.
MCPC demonstrated strong feasibility and acceptability. Sixty-two percent (43/69) of potentially eligible patients agreed to screening, 88% (38/43) met inclusion criteria, and 79% (30/38) consented/completed baseline assessment. Retention was excellent—90% (27/30) of participants completed all four intervention sessions. In a systematic review of psychosocial interventions for patients with advanced cancer, session completion rates for CBT-based interventions ranged from 36% to 100%. 59 Brief remotely delivered interventions may be particularly beneficial for patients who face barriers (e.g., immune suppression) to attending in-person appointments.32,39,60 Participants also found MCPC to be acceptable, and many (81%; 21/26) reported weekly use of the skills/ideas from the intervention. These findings build on our qualitative work 39 and reinforce the importance of addressing meaning in the context of coping with cancer pain.
Exploratory effect size estimates suggest that participants improved from baseline to both post-intervention time points on nearly all outcome measures. Primary outcomes of pain severity, pain interference, and spiritual well-being showed small to large effect sizes, consistent with previous trials of psychosocial pain management interventions 29 and Meaning-Centered Psychotherapy.23–26 Interestingly, participants showed improvement on two key facets of spiritual well-being: feelings of peace and reliance on faith. During MCPC sessions, participants often incorporated their religious faith or spiritual beliefs into their coping skill practice (e.g., using imagery to meditate on a pain-free afterlife). MCPC's session content included flexible language that, when appropriate, allowed the therapist to encourage participants to lean on their religious/spiritual beliefs.
Study limitations and future directions warrant consideration. Effect size estimates were highly variable and difficult to interpret without a control group. Nearly all (90%; 27/30) participants were non-Hispanic and had some college education. Only limited information was collected from participants' medical records; additional details about cancer (e.g., location of metastases) and pain (e.g., treatment related, tumor related, remittable) should be collected. Moreover, the results (e.g., high retention rate) may have been influenced by our selection criteria. Patients who were capable of only limited or no self-care (i.e., ECOG >2) were excluded from the study; future studies should consider including caregivers and/or inpatient delivery. Furthermore, MCPC was designed to be relevant across multiple cancer and pain types so that, if it proves to be efficacious, it could be widely disseminated. A limitation of this broad approach is that certain patient populations may benefit from tailored content. Future qualitative studies should explore how patients' perceived meaning of pain (e.g., whether the pain is related to disease progression or surgery) relates to their emotional well-being and whether MCPC's content should be modified for specific cancer/pain types. This work would help determine if MCPC should remain broad in its approach or adapted (e.g., supplemental modules) for specific populations. We will further evaluate MCPC with a larger more demographically/medically diverse sample using an RCT design with post-intervention qualitative interviews.
Conclusions
This study provides promising findings regarding the feasibility and acceptability of MCPC. This intervention may provide an important avenue for alleviating suffering in patients facing pain from advanced cancer.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and data analysis and interpretation were performed by J.G.W., K.R., S.A.K., and T.J.S. The first draft of the article was written by J.G.W., and all authors commented on previous versions of the article and approved the final article.
Acknowledgments
The authors thank the study participants and D. Mark Waters, ANP-BC, Jason A. Webb, MD, R. Morgan Bain, MD, and Rebekah M. Winger, BS, for their assistance with this study. Results from this study were accepted for presentation at the Society of Behavioral Medicine 42nd Annual Meeting and Scientific Sessions.
Funding Information
This study was funded by a postdoctoral fellowship awarded to J.G.W. from the American Cancer Society 130526-PF-17-054-01-PCSM. J.G.W.'s work was also funded, in part, by a Kornfeld Scholars Program Award from the National Palliative Care Research Center. W.S.B.'s work was funded, in part, through the NIH/NCI Cancer Center Support Grant P30 CA008748 and NIH/NCI Meaning-Centered Psychotherapy Training Program for Cancer Care Clinicians Grant 2 R25 CA190169-06.
Author Disclosure Statement
No competing financial interests exist.