
Abstract
Background:
There are racial/ethnic disparities in hospice use and end-of-life (EOL) care outcomes in the United States. Although the use of community health workers (CHWs) and patient navigators (PNs) has been suggested as a means of reducing them, CHW/PNs' attitudes toward a palliative care philosophy remain unknown. The purpose of this study was to examine how personal attributes affect a CHW/PN's attitude toward EOL care.
Methods:
CHWs/PNs were recruited from two state-wide organizations and invited to complete an online survey. We collected information on demographics, attitudes toward the palliative care philosophy, and comfort with caring for patients at the EOL.
Results:
Of the 70 CHWs/PNs who responded to the survey, 82.5% identified as female, 56.4% identified as black, and 56.2% had a four-year college degree or higher. The mean score on a validated scale to assess attitudes toward EOL care was 33.5 (SD = 4.9; possible range, 8–40). Eighty percent strongly agreed or agreed with being open to discussing death with a dying patient. Higher self-efficacy scores were associated with more favorable attitudes toward hospice (r = 0.306, p = 0.016).
Conclusions:
CHWs/PNs have an overall favorable attitude toward the palliative care philosophy and may be inclined to providing EOL care.
Introduction
Providing end-of-life (EOL) care in an equitable manner is a challenge for health care systems striving to deliver high-value care to all patient populations. 1 Although EOL care provides demonstrable improvement in patient satisfaction and decreased health care expenditures, it remains underused.2–4 For example, palliative care utilization for patients with advanced cancer may be less than 10%.5,6 Furthermore, palliative care use is much lower among minorities than the general population due to socioeconomic and cultural factors.7–10 Applying a sociocultural lens to focus on barriers that limit access has been identified as a strategy for facilitating EOL care access for minority patients.
One potential solution to reducing racial disparities in palliative care is the use of community health workers (CHWs)/patient navigators (PNs) in EOL care.11–13 While CHWs and PNs have different training and may work in different environments (community vs. clinic), they provide a range of patient-centered services, including addressing social determinants of health to improve access to the health care system.14–16 CHW/PN-delivered interventions are associated with improved patient-centered outcomes.17–19 In the context of terminal illnesses, CHWs/PNs are educators, advocates, and sources of empowerment for patients in need of palliative care.15–18,20
Despite the increased presence of CHWs/PNs in EOL, 21 the perceptions of their roles in this realm are unclear due to a lack of standardized definition of their roles and utilization in practice. 22 CHW/PNs' attitudes toward EOL care may directly influence their willingness to recommend this and advocate for this in their communities and with their patients.23–30 However, there is a gap in understanding CHW/PNs' beliefs regarding EOL care. 31 This gap is important to address since CHWs/PNs can augment patient access to EOL care but are not currently used frequently in this role.21,31,32 Our previous work and that of others have established the barriers to implementation of CHW programs in practice to improve components of EOL and culture change.31,33,34 These models depend on direct personnel involvement, and thus, our team recognized that an understudied area is that of the CHW/PN. Future work must consider how to adequately train these CHWs/PNs and thus understanding better those barriers (i.e., stress of care for patients with serious illness, baseline ability to manage) drove this work. To address these concerns, we examined self-reported stress, self-efficacy, and patient-centeredness among a cohort of CHWs/PNs to explore the extent to which these attributes influence their attitudes toward EOL care.
Methods
Study design
This is a cross-sectional survey to assess the attitudes of CHWs/PNs toward EOL care. The cross-sectional design allowed us to sample many participants in this descriptive study. This study was reviewed by the Johns Hopkins Medicine Institutional Review Board and was deemed to be exempt research under the Department of Health and Human Services regulations (IRB00186615). Participants received a description of the study with contact information for the study team at the beginning of the survey. Surveys were only linked to participants' e-mail addresses and all data were electronic and stored on secure institutional servers.
Population
An invitation to complete a self-administered electronic survey was e-mailed to all members of the two CHW/PN groups in Maryland (N = 350). All members of these two professional groups with a valid e-mail address were eligible to participate. Respondents completed the survey online through a personalized link using their e-mail address, between July 2019 and November 2019. The study team members (F.M.J. and C.A.I.) had developed relationships with these two groups and group leadership e-mailed their members regarding the study throughout the study period. Nonresponders were also sent electronic reminders until the end of the study. Pilot-testing of the survey allowed us to estimate the time of completion of 20 to 30 minutes. Participants were provided with a nominal gift card as compensation for their time.
Survey development and measures
Participants' demographic (age, sex, and race/ethnicity) and socioeconomic characteristics (education and household income) were collected. Validated instruments were used to assess attitudes toward palliative care and hospice philosophy, as well as self-reported stress, self-efficacy, and patient-centeredness. The Hospice Philosophy Scale (hospice philosophy score [HPS]; range 8–40) 35 was used to characterize CHW/PN attitudes toward providing support for palliative and EOL care. Higher HPSs measure how concordant a provider's EOL care beliefs are with the philosophies of hospice care. The internal consistency of the HPS, by Cronbach's alpha, was 0.855. 36 Two additional questions were adapted from the Self-Competence in Death Work scale 37 because these concepts were lacking from the HPS: “I can fully accept that I cannot completely control life, for example, the life and death of patient/service user” and “I am open to discussing death with a patient who is dying.”
The Perceived Stress Scale (PSS-4), 38 the General Self-Efficacy (GSE) scale, 39 and the Patient-Practitioner Orientation scale (PPOS) were also utilized. 40 The PSS-4 is a 4-item scale used to measure perceived stress in the last month with answers on a 5-point Likert scale from never to very often. Higher scores represent higher levels of stress with a possible range of 0 to 16. The PSS-4 was developed to better estimate an individual's perceived stress rather than the amount of objective stressors, such as life events, to help predict health outcomes. 38 The GSE measures self-efficacy, or confidence, in effectively performing across different tasks and situations, 39 via 8 items (possible total score of 1–5), and has been shown to be related to EOL care provider experience. 41 The GSE measures an individual's inherent ability to cope and sustain perseverance throughout a range of stressful life experiences. 42 The 18-item PPOS is used to assess preference for patient-centered medical care. Mean scores range from 1 to 6, with a higher score indicating a patient-centered view of medical care as exemplified by items such as “Patients should be treated as if they were partners with the doctor, equal in power and status.” 43 Lower scores on the PPOS represent a physician-centric preference for medical care, for example, “The doctor is the one who should decide what gets talked about during a visit.” The PSS-4, 44 GSE, 39 PPOS,45,46 and HPS 35 have been used to quantitatively compare traits between groups without defining absolute cutoffs. Due to the importance of communication in EOL decisions, we hypothesized that patient centeredness correlates with how open a provider is to palliative care philosophy. These measures were selected because we hypothesized that they may be related to EOL care attitudes. The internal consistency, as measured by Cronbach's alpha, of the PSS-4, GSE, and PPOS was 0.568, 0.920, and 0.704, respectively.
Statistical analysis
Descriptive statistics were used to characterize participants' responses. The analysis of variance or the Kruskal–Wallis test was used to compare mean values, as appropriate; age and PPOS were the only normally distributed quantitative measures. Two-sided alpha of 0.05 was used to determine statistical significance. We used Pearson correlation coefficients to compare continuous variables and developed multivariable linear regression models to identify predictors of favorable palliative care attitudes (i.e., outcome variable was HPS). The variables were selected a priori (i.e., we included PSS-4, GSE, and PPOS in the multivariable linear regression), using the scores from the validated instruments and adjusting for race, gender, income, age, and educational attainment. Observations with missing data were dropped from that individual measure but not the entire cohort (i.e., a survey with only a missing age was not included in the mean age calculation or any regression involving age). Statistical analyses were performed using R v3.4.1 in RStudio 47 and Stata release 15.1 (StataCorp, College Station, TX). 48
Results
Sample characteristics
Table 1 summarizes the characteristics of the study population. After soliciting participation from all registered members of the CHW and PN associations (350 members), 70 responded (response rate of 20%). The majority were female (82.5%) and the median age was 49 years (interquartile range, 18.5 years; Table 1). Approximately half of the respondents self-identified as non-Hispanic black or African American (56.4%), 25.8% identified as non-Hispanic white, and 11.3% identified as Hispanic. Respondents had diverse levels of educational attainment and household income. Almost one-third (29%) of the respondents had an annual household income of less than $50,000, and 22.5% of respondents had a household income greater than $100,000. Twenty percent had a graduate degree, 35.9% had a bachelor's degree, 35.9% had completed some college, and 7.8% had obtained a high school degree. All CHWs/PNs made referrals, conducted home visits, ran support groups, and recruited cases in their work (Fig. 1).
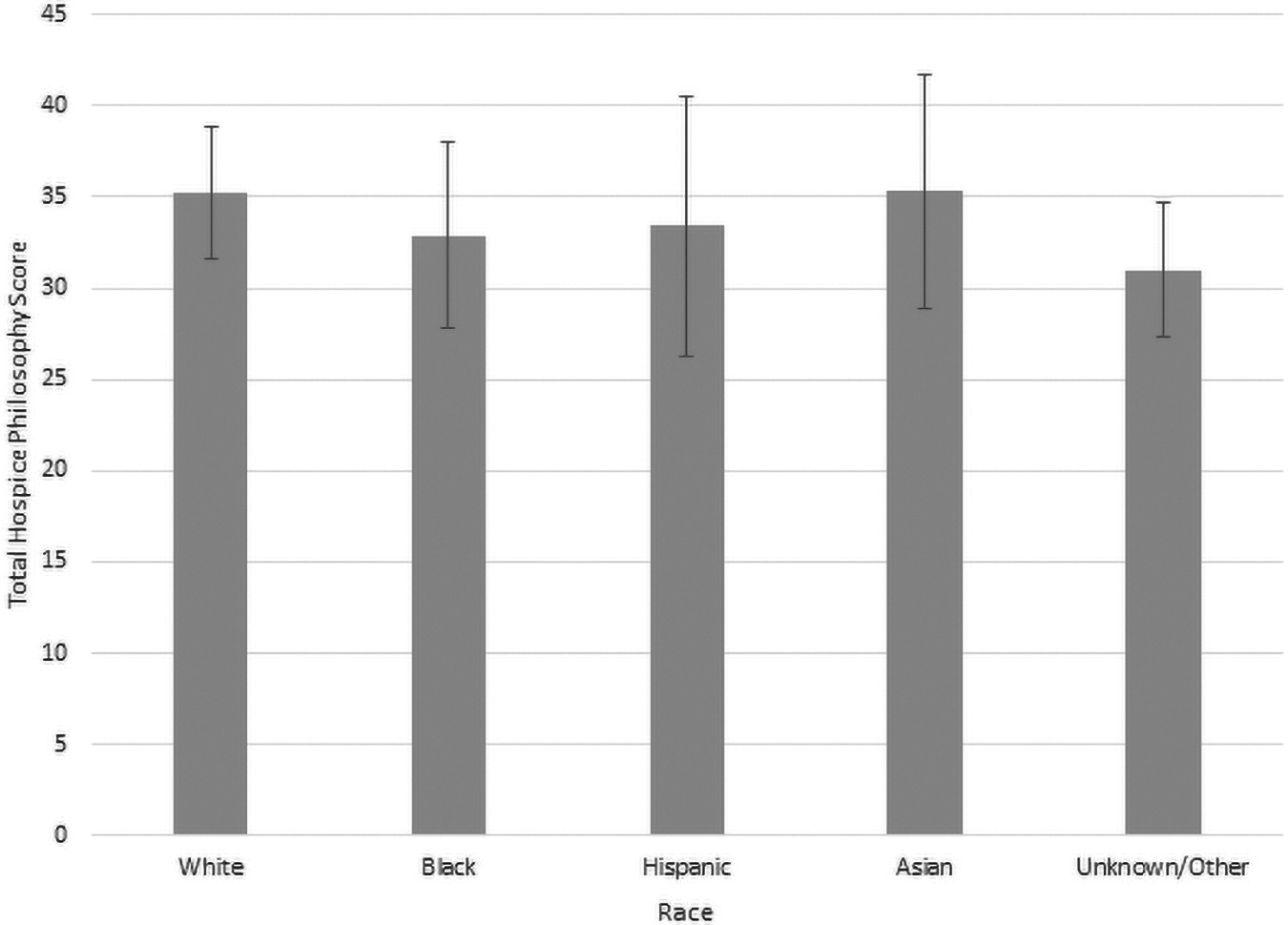
Total HPS by race. Total HPS by race/ethnicity. The difference in HPSs by race was compared with white race as the reference group. p-value >0.05. HPS, hospice philosophy scale; NS, nonsignificant.
Community Health Worker/Patient Navigator Demographic Characteristics
CHW, community health worker.
CHW/PN beliefs about EOL care
The mean HPS was 33.5 (SD = 4.9; Table 2). Table 3 and Figure 2 show that black and Hispanic CHWs/PNs had lower HPSs than white and Asian CHWs/PNs, although these differences were not statistically significant (p = 0.4). Almost all respondents (93.8%) strongly agreed or agreed with the statement “I can fully accept that I cannot completely control life, for example, the life and death of patient/service user.” Eighty percent strongly agreed or agreed with the statement, “I am open to discussing death with a patient who is dying” (Fig. 2).
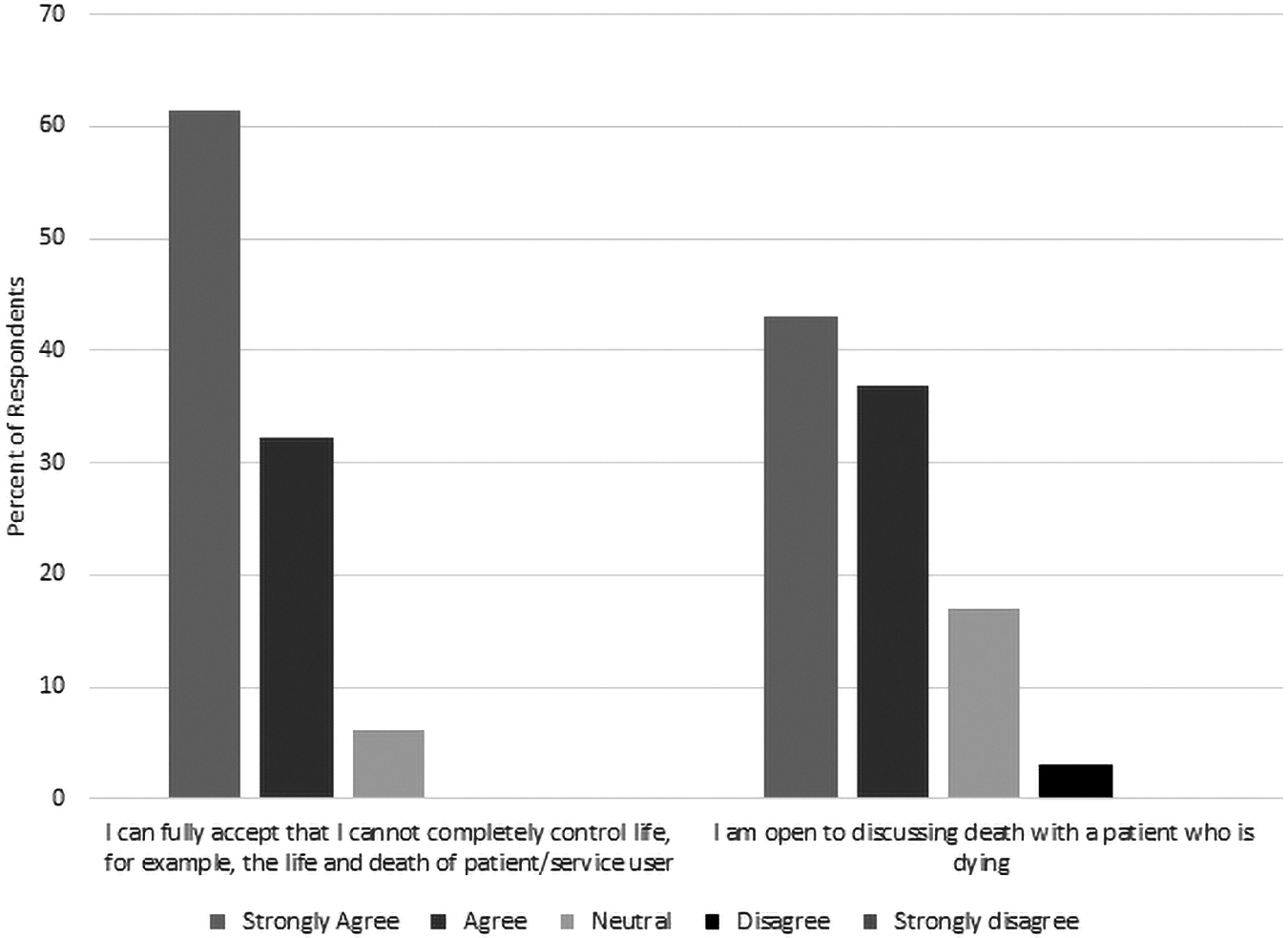
EOL care beliefs of patient navigators and community health workers. Participant responses to two questions asking about EOL beliefs not captured in the HPS. EOL, end of life.
Validated Scale Measurements of Community Health Worker and Patient Navigator Stress, Discrimination, Self-Efficacy, Patient/Physician Orientation, and Hospice Beliefs
GSE, general self-efficacy; HPS, hospice philosophy scale; PPOS, patient physician orientation scale.
Differences in Patient/Physician Orientation Scale and Hospice Philosophy Score Based on Race
Stress, self-efficacy, and patient/physician orientation in CHWs/PNs
Mean PSS-4 score was 5.24 (SD = 2.48), mean GSE was 4.27 (SD = 0.55), and mean total PPOS was 2.94 (SD = 0.53), with 85.7% of CHWs/PNs having low (practitioner-centered) scores, 1.4% with medium scores, and 12.9% with high (patient-centered) scores (Fig. 1). There were no racial differences in mean scores on the PPOS (Table 2).
Predictors of favorable attitudes toward palliative care philosophy
Higher patient-centered scores on the PPOS were associated with lower HPSs (r = −0.312, p = 0.015), while higher self-efficacy scores were associated with more favorable attitudes toward a palliative care philosophy (r = 0.306, p = 0.016) (Table 4). Neither race, age, income, gender, nor stress levels (PSS-4) were associated with HPSs in pairwise associations. In a multivariable model including PSS, PPOS, GSE, race, gender, income status, age, and education status, only GSE remained statistically significant (p-value = 0.01) related to HPS (Table 5).
Correlation Coefficients between Surveyed Scales
Correlation matrix of survey scales.
p-value <0.05, **p-value <0.01, and ***p-value <0.001. All values reported as the correlation coefficient r of a simple linear regression.
PSS-4, perceived stress scale 4.
Multivariable Linear Regression Output between Hospice Philosophy Score, Scales, and Demographic Variables
Multivariable linear regression relating HPS to other survey measures (PPOS, HPS). Null indicator variables = white, high school, or GED equivalency, $20,000–$34,999, and male. R2 = 0.3895 (p-value = 0.1234).
Discussion
We observed favorable attitudes toward the palliative care philosophy and a willingness to work with EOL patients at the EOL among a cohort of predominantly female, non-Hispanic CHWs/PNs. Demographically, our study population is similar to other CHWs/PNs in the United States.49,50
The majority of CHWs/PNs accepted their lack of control of whether a patient lives or dies and are open to discussing death with patients. In addition, the CHWs/PNs in this sample had an overwhelmingly favorable attitude toward the palliative care philosophy, as measured by HPS. We identified no racial differences in favorable attitudes toward palliative care. This is in contrast to the findings of Van Dussen et al., in which black adults had lower HPSs compared with white adults. 35 These racial differences were hypothesized to be the result of mistrust in the health care system. Our findings of no racial differences may be driven by our respondents being CHWs/PNs, who are more involved in the health care system and may exhibit more trust in the health care system compared with their lay counterparts. 51
Our finding of higher patient centeredness being associated with lower HPSs was unexpected, and while statistically significant, the association was weak and driven by a small proportion of the sample with high patient centeredness. This association was attenuated after adjustments for demographic and other psychosocial factors. GSE, however, was associated with more favorable attitudes toward palliative care philosophy in univariable and multivariable models. The positive association between confidence performing certain tasks (self-efficacy) and attitudes toward palliative care indicates that CHWs/PNs are willing and able to perform tasks in the realm of EOL care. Despite the perception that this work may be beyond their scope, 52 previous research has demonstrated that there is a lower level of awareness for EOL care in minority patient populations 23 ; CHWs/PNs may mitigate these gaps.
Limitations
This study had several limitations. The sample size is small, increasing the likelihood of type I errors. The cross-sectional design limits the ability to draw causal inferences from this study. It is also limited to CHW/PNs in a single state, which may affect the generalizability of these findings. However, the sampling frame used in this study (two state-wide groups) is theoretically open to all CHWs/PNs in the state of Maryland. This decreases frame biases, in which the target population is not adequately covered in the sampling frame and improves the internal validity of this survey. This survey is subject to respondent selection bias through which certain groups of people are more likely or less likely to volunteer for the study. Furthermore, our survey failed to account for a CHW/PN's spirituality, an important feature in EOL care. 53 There may be other predictors of attitudes toward EOL care that were unmeasured in this study. All surveys are potentially subject to social desirability bias, but our use of self-administered, anonymous surveys reduces the risk of this threat to validity.
Conclusion
In this study, we assessed the EOL care views of CHWs/PNs and the potential for different personal attributes affected CHW/PN viewpoints on EOL care. Our findings reveal that CHWs/PNs have a positive outlook on palliative care. These results give preliminary evidence in support of integrating CHWs/PNs into EOL care. Given that CHW/PNs in general, and in our sample specifically, tend to be more representative of the minority populations in the United States, CHWs/PNs may be a valuable resource to address disparities in EOL care. 54 Future research should consider how CHW/PN attributes affect EOL care decisions, palliative care utilization among underrepresented patient populations, and patient and caregiver experiences at the EOL. We hope this finding supports further community-based interventions to expand access to and decrease disparities in palliative care.
Footnotes
Authors' Contributions
Conception and design: K.T.L., C.A.I., and F.M.J. Collection of data: K.T.L. Data analysis and interpretation: K.T.L, A.D.Z, and F.M.J. Article writing: all authors. Final approval of the article: all authors. Accountable for all aspects of the work: all authors
Disclaimer
This article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
Funding Information
This work was funded by the National Heart, Lung, and Blood Institute Institutional National Research Service Award T32 HL139426, National Heart, Lung, and Blood Institute 1K01HL153204-01, and AHRQ 1K08HS024736.
Author Disclosure Statement
The authors have no financial or personal relationships that could inappropriately influence the work reported in this study. K.T.L has received research funding to the institution from Pfizer and has been an unpaid consultant for Eli Lilly.