
Abstract
Background:
Surgeons must evaluate and communicate the risk associated with operative procedures for patients at high risk of poor postoperative outcomes. Multidisciplinary approaches to complex decision making are needed.
Objective:
To improve physician decision making for high-risk surgical patients.
Design:
This is a retrospective review of patients presented to a multidisciplinary committee for three years.
Setting/Subjects:
Evaluation of patients was done in a single-center U.S. veterans affairs (VA) hospital. All patients who were considered for surgery had a VA Surgical Quality Improvement Program (VASQIP) risk calculator 30-day mortality >5%.
Measurements:
Thirty-day and one-year mortality were measured.
Results:
Seventy-six patients were reviewed with an average expected 30-day mortality of 14.2%. Forty-two patients (57%) had a recommended change in the care plan before surgery. Fifty-four patients (71%) proceeded with surgery and experienced a 30-day mortality of 7.4%.
Conclusions and Relevance:
Multidisciplinary discussion of high-risk surgical patients may help surgeons make perioperative recommendations for patients. Implementation of a multidisciplinary high-risk committee should be considered at facilities that manage high-risk surgical patients.
Introduction
In 2010, 38
In contrast, the vast majority (75%) of seriously ill patients say they would not choose life-sustaining treatment if they knew the outcome would be long-term cognitive or functional impairment. 5 These critical decision-making discussions place a significant burden on clinicians to make accurate risk determination and recommendations to patients. Decisions to proceed with major operations are especially pertinent for those who are critically ill or at high risk for morbidity and mortality, Withholding or withdrawing treatments is among the most challenging ethical dilemmas for nurses and doctors that were associated with highest rates of staff burnout. 6
Medical decision making should not only be driven by physician's expectations but also incorporate patient values to determine whether the risks are in line with patient's goals of care. 7 A true understanding of complications and long-term consequences in complex patients may be better assessed by an interdisciplinary team that manages the patient. The aging veteran population has additional vulnerabilities that make decision making more complex, including a higher prevalence of cancer, diabetes, and mental health conditions, as well as increased frailty compared with nonveterans.8,9 To help with this decision-making process, we created a multidisciplinary committee to improve preoperative decision making and outcomes for our high-risk patients.
Methods
The Rocky Mountain Regional Veterans Affairs (VA) Medical Center is a Level 1a complexity surgical facility responsible for complex surgical cases in Veteran Integrated Service Network 19. These patients include candidates for cardiac, thoracic, vascular, neurosurgical, general, and urologic procedures. The implementation of this initiative was a quality improvement project by the department of surgery to address the high mortality seen in our institution from 2013 to 2014. Implementation of the multidisciplinary committee at this VA Medical Center had three objectives: first, to determine whether the medical teams agree that proceeding with surgery would benefit the patient. Second, to evaluate whether the realistic outcome of the surgery was in line with the patient's goals of care. Third, to identify modifiable risk factors that could be addressed or improved upon before surgery. Beginning in 2016, the department mandated that all patients scheduled for surgery have a 30-day mortality risk calculated by the Veterans Affairs Surgical Quality Improvement Program (VASQIP) database risk calculator. 10 It was recommended by the department that all patients with a >5% risk of death within 30 days be presented at this committee. Patients are presented by the primary surgical team to the multidisciplinary committee with all care team members present. No subspecialties are excluded. The committee providers include all phases of perioperative care, including surgery, anesthesiology, critical care, palliative care, geriatrics, ethics, and hospital medicine. Additional attendees include risk management, quality improvement nurses, social work, physical therapy, and occupational therapy. The committee is available on a routine weekly basis or ad hoc for consideration of cases who needed to be performed urgently. Once there was a consensus decision on the next step, the primary team would proceed with care as outlined by the decision-making committee. The recommendations made by the committee were not mandatory but were documented in the patient's chart.
For patients who had surgery, 30-day and 1-year mortality were collected retrospectively. For patients who did not have surgery, decision-making outcomes as well as 30-day to 1-year mortality from the time of discussion were collected. The University of Colorado Institution Review Board granted exemption for this quality improvement initiative review.
Results
Seventy-six patients with a predicted VASQIP score >5% were reviewed by the committee between January 2016 and December 2019. The preoperative average 30-day mortality risk for the group was 14.2% with a range of 5.0% to 73.3%. Patient demographics are given in Table 1. The specialties reviewed are given in Table 2.
Patient Demographics
DNR, do-not-resuscitate order; VASQIP, Veterans Affairs Surgical Quality Improvement Program.
Surgery Specialty Cases Reviewed
After multidisciplinary review, 42 patients (57%) had a change in the care plan. Examples of changes in the operative plan included amputation instead of revascularization, transmetatarsal instead of partial ray amputation, and girdle stone procedure instead of a total join replacement. Changes in anesthesia included utilization of local versus a general anesthetic. Specialty consultations recommended included palliative care, cardiology, renal, and pulmonary. For five patients, surgery was not recommended.
Fifty-four (71%) patients went on to surgery and 4 patients (7.4%, 4/54 patients) died within 30 days of surgery in contrast to the mean expected 30-day mortality of this group of 54 patients (13.0%). Overall, one-year mortality for this group was 38% (21/55).
Twenty-two patients (27.6%) did not proceed with surgery after presentation to the committee. The decision making and outcomes are shown in Figure 1. Eight patients were discharged to hospice care. Within 30 days of discussion, one patient died, (1/22, 4.5%), Overall, one-year mortality for this group was 55% (12/22).
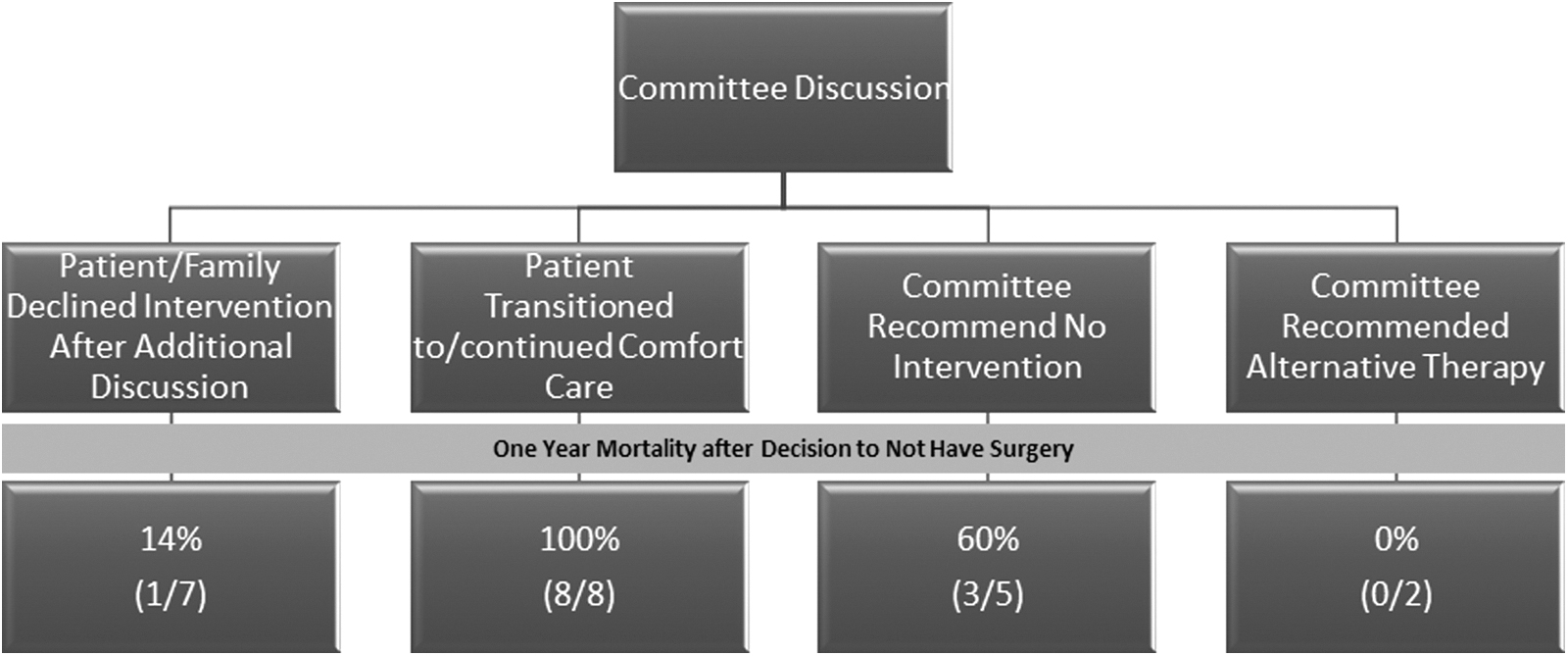
Decision making and one-year outcomes for nonsurgical patients.
Discussion
There are no uniform recommendations for surgery in patients with a high potential risk of morbidity and mortality. Sacks et al. found a 39% variation in surgical recommendations when practicing surgeons were presented urgent clinical vignettes and asked to consider the risks of operative versus nonoperative management. 11 Surgeons consistently chose the treatment plan that maximized the benefits and minimized harm, but significant variation came with the surgeons' judgment of the possible outcomes in complicated patients. A multidisciplinary committee to make these recommendations represents a new paradigm in decision making, eliciting the opinion of all perioperative services to present a united recommendation to patients.
This is one of the first articles to describe a multidisciplinary surgical decision-making committee for high-risk patients. We observed a lower 30-day mortality of 7.3% in the patients who had surgery compared with the predicted (13.0% 30 day mortality for the 54 patients who had surgery); however, the difficulty in the management of high-risk patients is apparent in our cohort where a significant number of patients died within one year of discussion, whether or not they had surgery (55% for nonoperative patients vs. 38% for patients who had surgery). For these patients, standardized risk calculators are not an adequate mechanism to describe the risk of a procedure. 12 Establishment of a multidisciplinary committee may be a more meaningful alternative for assessing risks for both the providers and patients.
Instead of 30-day mortality, outcomes such as disability-free survival, days spent at home, or freedom from pain after surgery have been suggested as more meaningful measures for patients after surgery. 13 Rather than a surgical risk calculator, these outcomes are better addressed through consultation with all of the providers and teams caring for these complex patients. One example of our focus on patient-centered outcomes is the inclusion of palliative care in the 1/3 of our recommendations (26/76) patients. Nationally, palliative care has been identified as an underutilized means to improve preoperative physician–patient communication. 14 By clarifying goals from the patient's perspective, patients are able to identify what they are willing and not willing to endure to achieve their desired outcomes, indicated by the 10.5% (8/76) of our patients who chose hospice care as an alternative to an invasive procedure.
In addition to patient benefits, improving communication between all medical teams can help alleviate the decision-making process for the operating surgeon. We found that it was surgeons who requested more meetings with the committee than other services to discuss potential plans and, more importantly, present a consensus to the patients, an observation also previously made by Sroka et al. in a similar anesthesia-led initiative. 15 This type of complex decision making not only affects the patients and their family but is also a significant factor in physician and staff effectiveness and longevity. Although not specifically evaluated in our study, multidisciplinary discussion and decision making likely reduce this burden and may improve staff and physician satisfaction and longevity.
There are three major limitations in our pilot study. This is a retrospective review of patients who were selected by their medical providers to be reviewed. There were likely patients who could have been presented but were not brought to the committee. A second major limitation is the lack of a standardized approach for recommendations after presentation. These recommendations were made by consensus opinion, and follow-up of the steps for optimization was left to the primary surgical team. Although all teams and patients followed the recommendations, objective evidence of this is difficult to assess. Finally, to truly create a patient-centered discussion, it is imperative to include the patients or their representative at these discussions, a modification we will be trialing in the near future.
Conclusion
Surgical decision making will only become more complex as the population ages and treatment options become more complex. We have demonstrated that, with resources already at hand, a multidisciplinary review of high-risk surgical patients may aid in decision-making physicians. Widespread implementation has the potential to not only improve morbidity and mortality but also improve patient and family satisfaction as well as reduce physician and staff burnout.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.