
Abstract

Dear Editor:
Management of phantom limb pain (PLP) after amputation is challenging in diabetic patients on hemodialysis because available medication is limited. This report will focus on a case of PLP managed by adjunctive use of mianserin and discuss the potential utility of mianserin as an auxiliary pharmacotherapy for the recalcitrant pain in diabetic patients on hemodialysis.
A woman in her early 70s had been receiving hemodialysis due to diabetic nephropathy for 5 years. She had been agonized by an intractable pain of her right leg caused by arteriosclerosis obliterans and peripheral neuropathy secondary to diabetes (Fig. 1A). Neither nonsteroidal anti-inflammatory drugs, tramadol, nor peripheral nerve blocks were efficient.
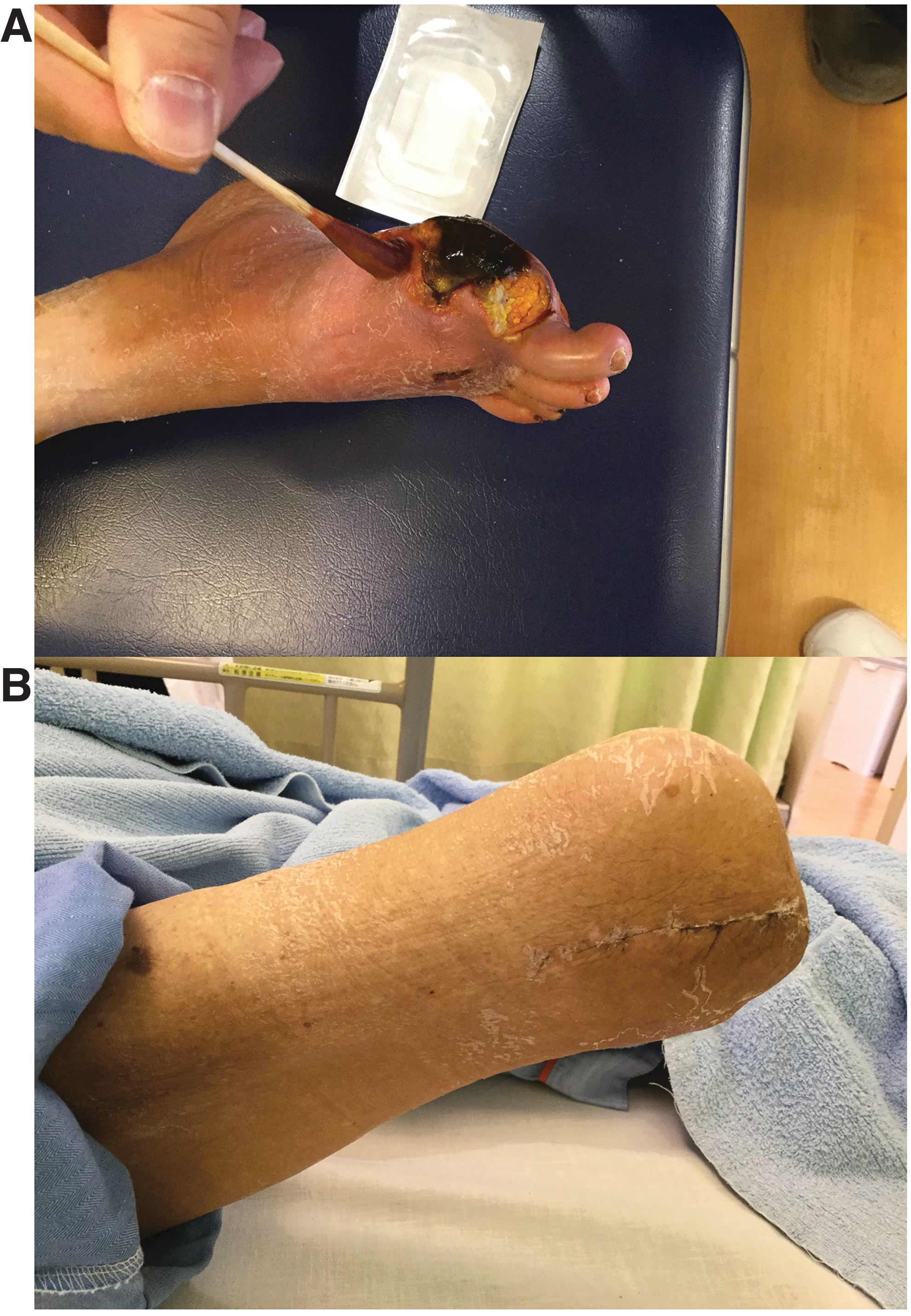
Her right leg ended up undergoing amputation, which developed PLP thereafter. The pain remained implacable and indicated 8–10/10 in the 0-to-10 Numerical Rating Scale (NRS) even one month after the operation when the surgical wound healed completely (Fig. 1B). She had not developed depressive disorder, but her sleep had been disturbed by the pain.
Available medication was limited due to her comorbidity. She tried antiepileptics such as gabapentin or mirogabalin, which were ineffective and caused nausea and somnolence. Serotonin-noradrenaline reuptake inhibitors were contraindicated in patients on hemodialysis. Tricyclic antidepressants and sodium channel blockers such as mexiletine were also to be avoided due to severe cardiac dysfunction caused by ischemic heart disease that imposed coronary artery bypass grafting on her.
The pain was partially palliated to 6/10 in NRS by 30 mg of codeine phosphate daily, but its dosage could not be increased sufficiently due to the risk of respiratory depression. Opioids such as morphine, hydromorphone, oxycodone, fentanyl, and tapentadol were needed to be avoided because they were strictly controlled for noncancer patients in Japan and they had safety concerns in patients on hemodialysis.
After starting 5 mg of mianserin nocte, the pain was assuaged to 0–2/10 in NRS and her insomnia was improved. She finally succeeded in discontinuing the regular use of codeine phosphate and coping with the pain by 5 mg of codeine phosphate on an as-needed basis once every few days.
Usefulness of mianserin for diabetic neuropathic pain is suggested in animal models. 1 However, its clinical efficacy has not been established fully, and there had been no report on effectiveness of mianserin for PLP. Mirtazapine, an analogue of mianserin, is reported to improve diabetic neuropathic pain 2 and PLP. 3 Similar to mirtazapine, mianserin might act antagonistically on α2 presynaptic receptors and increases monoamines, which could potentiate the descending pain inhibitory system. Mianserin is reported to act on sodium channels and opioid receptors, 4 which could improve the pain. Mianserin also could improve mood and sleep that affect the pain.
Mianserin might be weaker than mirtazapine regarding antidepressive effects. 5 However, mianserin has a shorter half life, which is more likely to prevent hangover and delirium, whereas mirtazapine could cause them. Mianserin does not need to be reduced in patients with renal dysfunction, whereas mirtazapine should be decreased depending on the creatinine clearance. Thus, adjunctive use of mianserin could be helpful to improve PLP in diabetic patients on hemodialysis.