
Abstract
Palliative care (PC) is beneficial, however, in many settings it is under-resourced and unable to consistently meet the needs of patients and their families. A lack of national health policy support for PC contributes to underutilization and the low value care experienced by many patients with serious illness at the end of life. Through a series of transformative health care structure and process improvements including developing robust initiatives and promoting institutional culture change, the Department of Veterans Affairs (VA) has significantly improved the quality of PC among veterans. VA's strategic simultaneous top-down and bottom-up approach to develop programs, policies, and initiatives provides important perspectives and deserves attention toward advancing PC in the broader U.S. health care system. Although opportunities for improvement exist, the comprehensive framework within VA should help inform the future of program development and serve as a model for integrated and accountable care organizations to emulate.
Introduction
Palliative care (PC) is associated with improved quality of life and decreased symptom burden for patients. 1 However, PC is under-resourced and does not consistently meet the needs of patients suffering from serious illness and their families. 2 Considerable variation exists in the availability, utilization, and quality of PC, which limits the potential benefits to patients and their families.3–6 Underuse of PC also contributes to high-intensity low-quality medical care received by many patients at the end of life7–10 that may not be consistent with their wishes or values. 11 Furthermore, the fee-for-service health care payment model is common in the US and may contribute to burdensome high-intensity care at the end of life by incentivizing quantity and not quality of care,12,13 as regional differences in physicians' practices are partially attributable to the availability of high-intensity health care. 14
In addition, important barriers to PC uptake include the lack of clinician knowledge of available resources and inadequate training in PC.14,15 Indeed, clinicians' practice patterns reflect their local environment or “culture,” as evidenced by multiple studies demonstrating that clinicians who work in areas of higher density health care services are more reliant on these resources with decreased emphasis on PC.3,7,16–19 In response to these shared challenges to the provision of high-quality PC across the US, the Department of Veterans Affair's (VA) implemented structure and process changes that provide key insights and a possible path forward for the broader U.S. health care system.
Structure and Process Changes
Recognizing the increased needs of an aging multimorbid veteran population and the underutilization of PC, 20 VA committed significant resources to develop, expand, and improve its PC capabilities over the past two decades (Fig. 1). The main goals of these efforts were to improve access to and the resultant quality of end-of-life care among veterans by developing and expanding program structure, defining processes of care, and initiating system-wide quality outcome measurements.
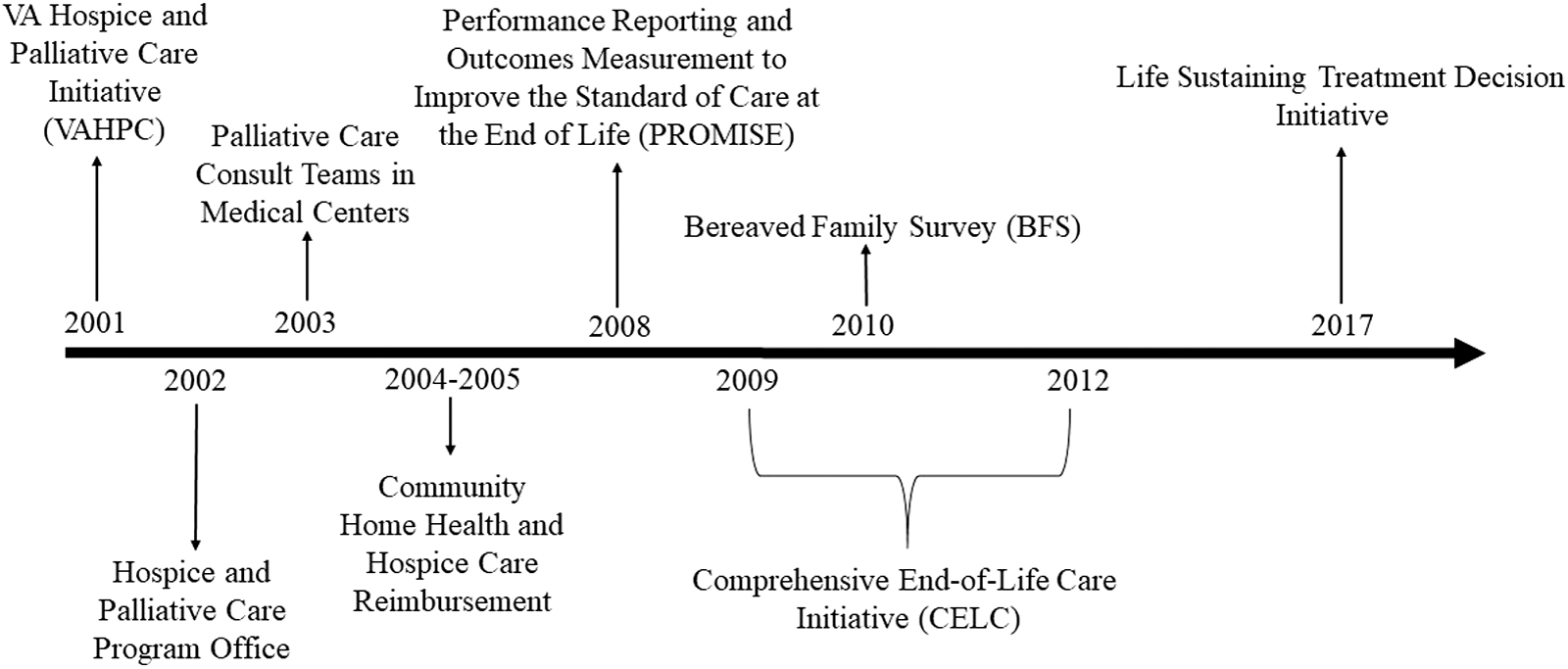
VA timeline for the development of palliative and hospice care program structure. Over the past 20 years, VA has devoted significant resources to the development and expansion of veterans' access to palliative care and hospice services. Beginning in 2001 with the development of the VAHPC and most recently with the Life Sustaining Treatment Decision Initiative in 2017 to enhance educating clinicians on conducting goals-of-care discussions and ensuring patients' goals, values, and preferences are elicited and documented in the electronic medical record. VAHPC, VA Hospice and Palliative Care Initiative.
To lead these efforts, VA established the hospice and palliative care initiative (VAHPC), which included the National Hospice–Veteran Partnership Program, and their Hospice and Palliative Care Program Office (Table 1). As part of this initiative, VA mandated that every medical center (hubs in their spoke-hub model) has an inpatient PC team providing clinical services to veterans and their families. 20 With generous funding from congress and partnerships with experts in the field including the Center to Advance Palliative Care (CAPC), VitalTalk®, and the Education in Palliative and End-of-life Care (EPEC) program, VA implemented its Comprehensive End-of-Life Care (CELC) initiative. This initiative also included start-up funding for multidisciplinary PC team members and the creation of the Veteran Experience Center (VEC). 21 The VEC tracks and collects data about care outcomes and satisfaction among bereaved family members and caregivers using validated surveys that have evolved over time. Initially, the Family Assessment of Treatment at End-of-life (FATE) survey 22 was developed and piloted for this purpose. Later, the FATE was replaced by the Bereaved Family Survey (BFS) that is endorsed as an end-of-life quality measure by the National Quality Forum. 23
Veterans Affairs Palliative Care and Hospice Program Advances in Chronological Order of Implementation
VA, Veterans Affairs.
Importantly, under the VA hospice program, veterans are able to receive concurrent medical and hospice care without the cessation of disease-modifying therapies—a unique feature that is not currently available in the Medicare Hospice Benefit. 24 The ability to receive medical care concurrent with hospice may contribute to higher quality,25,26 although results are mixed. 27 Concurrent care may eliminate the “terrible choice” between patients' common desires for both quantity and quality of life, 28 potentially removing a barrier to early hospice enrollment that is associated with improved symptom burden and quality of life. 29 Based on this concurrent care model within VA, the Center for Medicare & Medicaid Services is testing a demonstration project, Medicare Care Choices Model, evaluating whether hospice care provided in conjunction with other medical services can improve quality of life, increase patient satisfaction, and decrease expenditures. 30
Finally, VA initiated a policy called the Life Sustaining Treatment Decision Initiative, focused on educating clinicians on conducting goals-of-care discussions ensuring patients' goals, values, and preferences are elicited and documented in the electronic medical record using standardized tools across the continuum of care. 31 Clinicians (physicians, advance practice providers, nurses, social workers, chaplains, etc.) are offered comprehensive training communication sessions based on Vitaltalk, an evidence-based communication skills program. 32 In the first seven months of implementation across 137 VA facilities, ∼225,000 Life Sustaining Treatment Decision Initiative note templates were completed and entered into VA electronic health record for ∼110,000 unique veterans. 33 The initiative continues to expand and has now been implemented in 141 VA medical centers with ∼308,000 documented initial goals-of-care conversations per program data reports.
Results of VA System-Wide Improvements: Outcomes
Increased availability and access
As recently as 20 years ago, veterans had limited access to both palliative and hospice care. For example, in 2000, 38% of VA medical centers had inpatient PC programs, and only 5% of Veteran decedents received hospice care 20 compared to ∼22% among Medicare decedents. 9 With the establishment of the VAHPC and its associated structural and process changes, access to palliative and hospice care across VA has significantly improved. For example, a recent study found that hospice use among veteran decedents aged ≥65 years old increased by 7.6% between 2007–2008 and 2010–2014, compared with an increase of only 5.6% among Medicare decedents during that same time period. 34 Similarly, the number of inpatient veteran decedents who received PC consultation increased from 29% in 2003 to 46% in 2006. 20 Over this same period, the percentage of inpatient deaths occurring in hospice beds in VA almost tripled from 8% to 22%. 20 Among veterans with advanced lung cancer who were recommended to receive timely PC according to the American Society of Clinical Oncology guidelines, 35 one study found a 42% relative increase in PC receipt from 2007 to 2013 within VA. 36 However, in non-VA settings, underutilization of PC remains a persistent challenge. 37
Site of death
Congruence between preferred and actual place of death is an important aspect of quality end-of-life care. Although the majority of patients and families overwhelmingly prefer to die at home rather than in a hospital, 38 ∼30% of Americans use the intensive care unit (ICU) in the last month of life. 9 PC is one tool that can help align patients' treatment preferences with the care they actually receive. For example, among patients with advanced stage lung cancer, one study found that PC receipt was associated with a 43% reduced risk of death in an acute care hospital setting at the end of life compared with nonreceipt of PC. 36 Specifically within VA, improved access to PC through the initiatives described above likely improved congruence between patients' preferred and actual place of death. For example, one study found that veteran decedents who died in VA facilities were more likely to die in a dedicated PC or hospice unit rather than being admitted to an acute care unit compared with those who died in non-VA facilities (47% vs. 16%, respectively). 40 In that same study, families of veteran decedents who died in VA compared with non-VA facilities had significantly higher mean satisfaction scores on the FATE survey, indicating better quality of care at the end of life. 40 This higher satisfaction likely reflects increased access to PC services and dedicated hospice units within VA.
High-intensity treatment at the end of life
There is a growing body of evidence that the intensity of treatment received at the end of life is lower among veterans than among matched Medicare beneficiaries. For example, a recent study compared intensity of treatment received among veterans diagnosed with advanced colorectal or lung cancer between 2001 and 2002 with propensity-matched patients in fee-for-service Medicare. Authors found that Medicare beneficiaries were more likely to receive chemotherapy within 14 days of death (7.5% vs. 4.6%) or be admitted to an ICU within 30 days of death (19.7% vs. 12.5%) compared with veterans. 41 Similarly, another study of veterans with solid tumors who died between 2010 and 2014 compared intensity of treatment received among those who exclusively used VA services and those who were Medicare -reliant for their care in the last 30 days of life. 42 Authors found that Medicare beneficiaries were more likely to have received chemotherapy (adjusted odds ratio [aOR] = 1.73; confidence interval [95% CI]: 1.68–1.88), be admitted to an ICU (aOR = 1.43; 95% CI: 1.36–1.49), be hospitalized (aOR = 1.12; 95% CI: 1.09–1.16), or have experienced an in-hospital death (aOR = 1.19, 95% CI: 1.13–1.24) compared with veterans who were not reliant on Medicare. 42 Furthermore, among veterans with advanced stage lung cancer, PC was associated with reduced health care utilization including emergency department visits (adjusted incidence rate ratio [aIRR] = 0.86, 95% CI: 0.77–0.96), hospitalizations (aIRR = 0.64, 95% CI: 0.59–0.70, and ICU admission [aOR] = 0.63, 95% CI: 0.53–0.75). 39 Taken together these studies suggest that VA's palliative and end-of-life care initiatives may have helped reduce high-intensity care at the end of life that is consistently lower than comparable Medicare beneficiaries.
Bereaved families' perceptions of care
As part of the CELC initiative, surveys are administered to veterans' families or caregivers when veterans pass away in VA facilities. These surveys consistently demonstrate that families who receive PC and hospice services at VA report significantly higher quality of care. 22 For example, families of veterans who died in a PC unit had significantly higher mean FATE scores than families of veterans who died in other inpatient settings. 43 Families of veterans with end-stage renal disease44,45 or heart failure 46 who concurrently received PC and/or hospices services were also more likely to rate overall quality of end-of-life care better, through the BFS, compared with those families of patients who did not receive these services. Finally, earlier receipt of PC in the disease trajectory is associated with improved quality of end-of-life care as perceived by patients and their families. For example, one study found that families of decedent veterans were more likely to rate overall care as “excellent” on the BFS when the PC consult occurred 91–180 days before death, compared with those whose PC consult occurred 0–7 days before death (aOR = 1.37, 95% CI: 1.08–1.73). 47
Lessons for the Future
The strategic implementation and expansion of PC and hospice services that VA undertook have increased accessibility to services with improvements in patients' and families' experiences and reduced emphasis on burdensome low-quality care at the end of life, although, from the available evidence, these benefits are mostly demonstrated among veterans with cancer. Despite significant patient and family benefits, there are several potential reasons why widespread adoption of VA's PC structure and process changes has not occurred in non-VA settings.
First, similar to many health care policy changes, these initiatives occurred outside of a research framework, therefore, attributing specific changes to improved outcomes is challenging. Therefore, if similar programs are initiated in non-VA settings, there is significant potential for pragmatic or adaptive study designs to better discern outcomes and effect sizes. Second, program and leadership structure within VA have likely influenced local culture including clinicians' beliefs and practice patterns within the system, 48 which are known to be key drivers of the delivery and quality of end-of-life care,14,49,50 but may be difficult to replicate in other settings. A top-down approach to PC implementation including developing a program office to support initiatives and local leadership likely affected local institutional culture and disentangling the effects of structure or process changes versus institutional culture change is problematic. Finally, as an integrated health care system, VA can more easily influence care through the hiring of clinicians and other professionals, implementation of PC education or training for nurses, dissemination of institutional guidelines, and application of guidelines through local leadership. A national strategy to improve PC delivery has been suggested 51 and many of VA's programs and initiatives are scalable and deserve consideration for broader implementation in non-VA settings.
Several components of VA's programs may be more readily implementable. First, VA's experience in PC program development included emphasis on robust program infrastructure that supports program capacity, implementation, and sustainability. This infrastructure needs to include local program leadership who are able to promote, coordinate, and champion activities and initiatives including PC education for non-PC clinicians. Second, VA serves as a model for an interprofessional approach that is well suited to the practice of PC, as teams address multiple domains in caring for patients with serious illness including physical, psychological, social, and spiritual.52,53 Third, the creation of the VEC to monitor patient outcomes, with regular feedback to front-line PC staff, is an essential component of process improvement and is increasingly being implemented by health care organizations outside of PC disciplines. 54 Finally, the benefits of an integrated health care system where outpatient, acute care, rehabilitation, and inpatient hospice services share a common payer, electronic medical record, and infrastructure are likely central to improved outcomes among veterans as care coordination is a core domain of quality PC. 52
Despite the potential benefits afforded by the VA system in the provision of quality care among those with serious illness, major shifts in the financing of care are occurring, including recommendations that VA shift from a capitation-based system to an increasingly Medicare-like role in purchasing care in non-VA settings. 55 If this occurs, the question that arises is whether care delivery and quality will be better than the current VA system, studies suggest this will not be the case.42,56 Fee for service is the most common payment model that serves most Americans with serious illness and this model may incentivize clinicians and hospitals to render more intensive services than are beneficial at the end of life.57,58 Addressing the financial incentives of fee-for-service care is critical to health care reform efforts,59,60 and shifting payment from a service-based to a value-based model could emphasize patient preferences and improve the quality of end-of-life care. Finally, moving away from an integrated health care system to become a purchaser of care, VA would likely experience the same negative effects of fragmented care that plague patients, clinicians, and hospitals in nonintegrated health care systems,61–63 which may be particularly harmful for the delivery of quality PC. Although opportunities for improvement and research gaps exist within VA's framework, their PC program structure, processes, and policies deserve broader attention toward improving the quality of care among persons with serious illness.
Footnotes
Authors' Contributions
All authors made substantial contributions to this article based on the International Committee of Medical Journal Editors criteria.
Acknowledgments
We thank Dr. Kelly Vranas for her editing of earlier versions of this article. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Department of Veterans Affairs did not have a role in the conduct of the study, in the collection, management, analysis, interpretation of data, or in the preparation of the article.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States Government.
Funding Information
D.R.S. was funded through the Sojourns Scholar Leadership Program Award of the Cambia Health Foundation.
Author Disclosure Statement
No competing financial interests exist.