
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic compelled rapid transition to work from home for the University of Texas MD Anderson Cancer Center Palliative, Rehabilitation, and Integrative Medicine (PRIM) department to ensure social distancing and prevention of transmission.
Objectives:
To survey the attitudes and beliefs of personnel toward remote work during the COVID-19 pandemic.
Methods:
One hundred forty-eight clinical, research, and administrative PRIM department employees were invited to participate in an anonymous voluntary survey in May 2020, two months after the beginning of the COVID-19 pandemic and transition to work from home in the geographic location of Houston, Texas. The survey comprised 25 questions, including employee demographics and attitudes and beliefs toward working from home and the COVID-19 pandemic.
Results:
Ninety-four percent (139) of employees responded, with high response rates among all three employee arms. The majority of respondents were female (74%), between the ages of 30 and 59 years (87%), had broadband Internet (93%), and shared office space before working from home (59%). There were overall positive reports of experience (87%) and emotional response (79%) toward working from home, especially for those more concerned about COVID-19 illness and spread, shared office space, and those reporting adequate resources and equipment for remote work. Clinical role, however, was associated with a less positive response (80%), less productivity (29%), and higher levels of stress (62%). Most of the department also reported increased emotional exhaustion (68%). When surveyed about permanently working from home, most of the department responded favorably (69%).
Conclusions:
The PRIM rapid transition to remote work was associated with positive perceptions by most members of the clinical, research, and administrative teams. Insight from this survey can serve as a model for future rapid transitions in remote work and merits follow-up studies to prepare us for a postpandemic work environment. Clinical Trial Registration number NCI-2021-01265.
Introduction
The outbreak of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that leads to coronavirus disease 2019 (COVID-19) reached every continent in the world except the Antarctica and likely reached the United States in January 2020.1–3 During this unprecedented time, health care systems had to rapidly adjust and redesign service and care delivery. The infectious ability of SARS-CoV-2 requires physical distancing to reduce transmission and protect vulnerable at-risk populations,1,3 leading to recommendations for “Stay Home, Work Safe” orders to flatten the curve of new COVID-19 cases and protect health care resources.4–10 Our Palliative, Rehabilitation and Integrative Medicine (PRIM) Department at the University of Texas MD Anderson Cancer Center, located in Houston, TX, rapidly implemented a remote work model beginning March 13, 2020, to keep employees, patients, and their families safe.
Home-based telework is defined as working at or from home during part of an employee's contracted working hours.11,12 However, recent research has shown mixed results for home-based telework. Some studies indicate better employee performance, flexibility over work demands, autonomy, decreased work-role stress, work exhaustion, job satisfaction, and job-related well-being,13,14 while others suggest social and professional isolation, decreased knowledge sharing, work avoidance, and intensification of labor.11,14–16
These negative findings have also been observed in some studies evaluating the impact of home-based telework on organizational behavior and work performance as well as social support.11,15,16 The PRIM department had to face these challenges in a matter of days during the spring of 2020 as the COVID-19 pandemic continued to intensify.
PRIM administration and research employees transitioned to working from home full-time. Simultaneously, telemedicine was rapidly adopted by PRIM clinicians for outpatient and inpatient encounters, permitting palliative care teams to continue providing treatment even as critical decision making and symptom burden grew more urgent and access restricted.17–19 Clinicians were divided into shifts of work from home versus on campus. Work-from-home clinicians provided telemedicine to the ambulatory supportive care center and virtual inpatient visits, while in-person clinicians continued to provide inpatient care and occasional in-person ambulatory visits. Like research and administrative employees, PRIM clinicians transitioned to work mainly from home, delivering up to 50 virtual clinic visits a day.
To best manage these new long-term work arrangements, we designed an anonymous survey administered May 2020, two months since the start of the pandemic and after transitioning to remote work, toward the end of the first surge to determine the perceptions of PRIM employees regarding working from home and working on campus during the COVID-19 pandemic. By conducting the survey, the PRIM department sought to gain information about the challenges employees faced while transitioning to a telework/telemedicine environment, and the contribution of stressors that have been shown to be associated with providing health care during times of pandemic and the influence it can have on the telework environment.20,21
In this retrospective study, our primary objective was to determine the overall perceptions of PRIM personnel toward working from home during the COVID-19 pandemic. Secondarily, we explored associations between employee demographics, employee roles, and overall perceptions of working from home, COVID-19, workload, productivity, telework feasibility, and psychosocial burdens.
Methods
Survey
This retrospective study was approved by the Institutional Review Board at The University of Texas MD Anderson Cancer Center. The survey was designed ad hoc by interdisciplinary PRIM department leaders (chair, director, and management) in conjunction with scientist writers as a utilitarian effort to survey all personnel's experiences since transitioning to remote work due to the pandemic. The primary objective of this survey was to determine the attitudes and beliefs of the department's workforce toward work from home. This anonymous survey included two parts, demographic questions and questions regarding perceptions of work from home and the COVID-19 pandemic that took approximately five minutes to complete. The survey consisted of 25 questions developed through an iterative process to ensure that the most pertinent were included.
This quality improvement endeavor was intended to quickly identify needs and shape the departmental strategy moving forward with the health and safety of employees' families in mind during this pandemic, which can be directly related to work, as in many settings, employees have been worried about carrying the virus home to their loved ones. Likewise, questions also meant to address concerns about finances directly related to work in the COVID era, with workers concerned about layoff and ability to perform work, or on the contrary, less financial concern if no longer needing to commute.
A 5-point Likert scale (“Strongly Agree” to “Agree,” “Neither Agree nor Disagree,” “Disagree,” and “Strongly Disagree”) as well as a 7-point Likert scale (“Extremely negative” to “Very Negative,” “Somewhat Negative,” “Neither Positive nor Negative,” “Somewhat Positive,” “Very Positive,” and “Extremely Positive”) was used for the survey responses to determine the range and degree of these perceptions.
Survey administration
The PRIM department comprised palliative medicine, rehabilitation medicine, and integrative medicine clinicians, research personnel, and administrative staff with a total of 47 research team members, 80 clinicians, and 21 administrative personnel. Clinicians include physicians, advanced practice providers, registered nurses, medical assistants, psychologists, and counselors. The research team comprised managers, coordinators, data analysts, research nurses, research assistants, and research dieticians. The administrative team comprised administrative directors, operations manager, assistants, billing specialists, and clinical coordinators.
On May 18, 2020, all members of the clinical, research, and administrative teams in the PRIM department were sent an invitation e-mail to participate in the survey. Employees' e-mail addresses were used to automatically send the electronic survey through Qualtrics, and to send reminders to those who did not respond. Each employee was assigned a unique code, and e-mail addresses were not associated with the survey responses to maintain anonymity. Employees had five days to complete the survey, from May 18, 2020, to May 22, 2020. Participation in the survey was entirely voluntary, and no action was taken for refusal to participate in the study. The identities of those who did or did not respond were not revealed to leaders or managers.
Statistical analysis
Frequency and proportion were obtained for all the survey questions by each participant's role (research team members, clinicians, or administrative personnel) as well as for the total sample. Fisher's exact test was applied, and p-value was obtained to determine whether participants with different roles differ in the frequency with which they responded to the survey questions. The Fisher's exact test was applied both for the overall sample and for each pair of participant roles (clinical vs. research, clinical vs. administrative, and research vs. administrative).
Furthermore, to treat those survey questions with 5-point or 7-point Likert scale responses as continuous measures, ANOVA was first used to examine the overall difference in responses between roles and if significant difference was found for any survey questions (Table 2). Two-sample t test p-value was used to determine which pair of roles is significantly different from each other using a significance level at 0.0167 (Bonferroni correction 0.05/3 = 0.0167). Similar frequency and proportion were also reported for all the survey questions by gender. Fisher's exact test p-value was used to determine the significance of the gender difference on outcomes.
Finally, a subset of the survey questions, overall perception of working from home, perceptions about COVID-19, level of stress, increased time for caregiving for adult or minor dependants, financial burden, and emotional exhaustion, were identified and assessed with each of their associations with a list of predictors: gender, age, whether respondents had all the resources and equipment needed to work from home, whether respondents had high-speed Internet, level of concern in becoming ill due to the spread of COVID-19, concerns regarding the health and safety of their family, and whether respondents had increased time for caregiving for adult or minor dependants. Bivariate ordinary least squares (OLS) regressions were used to assess the association. Regression coefficients and the p-values are reported in Table 3.
Results
The survey had a high (94%) response rate from the research, clinical, and administrative teams, 87%, 97%, and 95%, respectively. Respondent numbers and demographic characteristics are presented in Table 1. Notably, the majority, across all teams, were female and between the ages of 30 and 59 years. Most employees also reported having broadband Internet and shared office space before working from home.
Respondent Characteristics
PRIM, Palliative, Rehabilitation, Integrative Medicine.
Overall experience toward work from home
Employees from all three teams reported a global positive experience toward the primary objective, “my overall experience with working from home has been,” with 87% (p = 0.093) ranging from “somewhat” to “very,” and “extremely positive” (Appendix Table A1). Figure 1 shows the distribution of overall global experience. Fewer clinical members reported a positive overall experience (76; 80%) than both research (41; 93%) and administrative members (20; 100%); the difference was significant (Table 2). Bivariate regression results of the overall perception of working from home showed that employees with shared office space had more positive overall perception of working from home, as well as employees who agreed more on having all the resources and equipment needed to work from home, or with a higher level of concern in becoming ill due to the spread of COVID-19 (Table 3).

Stacked bar graph of overall perceptions of working from home by employee role and total department.
Survey Questions with Significant Differences Associated with Employee Role and Analysis of Pairs of Roles
ANOVA of Likert scale responses was first treated as continuous measures to examine for the presence of any overall differences between employee roles and survey responses, followed by two-sample t-test analysis for significant differences between pairs of roles using significance level of 0.0167 (Bonferroni correction 0.05/3).
Bivariate OLS Regression Analysis of Responses When Treated as an Associated Factor Between Survey Questions
Subsets of survey questions regarding stressors during COVID-19 were identified and assessed with bivariate OLS regression with each other as possible predictive factors associated with employees' responses.
When asked “for me, being asked to work partially or completely from home permanently is,” the majority of the department, 69%, also found this to be positive, although to a lesser degree for the clinical team with a significant difference compared with the research and administrative teams (58% vs. 78% vs. 90%, respectively, Table 2).
Workload and productivity
Most respondents reported, “since COVID-19, my workload has,” no increase to a decrease in workload, (77 [56%]; p = 0.085), with no significant variation between employee roles (Table 2).
However, when surveyed about productivity with “compared to working on campus, I feel that when working at home I can be,” there were significant differences in employee role (Fig. 2 and Table 2). The majority of research (63%) and administration (75%) found working from home either more productive or neither more nor less productive. However, a significantly higher proportion (29%) of clinical members reported finding it less productive (Table 2).

Stacked bar graph of perceptions of productivity when working from home by employee role and total department.
Distress during the COVID-19 pandemic and working from home
Most of the department (68%) reported “since COVID-19, my emotional exhaustion has,” increased since the pandemic, with similar findings for clinicians (72%), researchers (66%), and administration (60%) (Table 2). Increased emotional exhaustion since COVID-19 was associated with employees who previously had their own office, higher level of concern in becoming ill, more concerns regarding the health and safety of family, and increased time demands for caregiving for dependants (Table 3).
Possible stressors were similar among employee roles (Table 2); Table 3 shows the association between concerns and different stressors.
Seventy nine percent of respondents found “for me, working from home is emotionally” positive, with significant differences depending on employee role (Table 2) and greatest positive report from administrative (90%) and research (86%) versus clinical (73%) roles.
Stress level
Forty-four percent of respondents reported increased stress two months after the start of the COVID-19 crisis in Houston compared with before it began. When surveyed, “compared to before the COVID-19 crisis, in the last 2 months my level of stress has been,” 32% responded with “somewhat worse,” and 12% “very” to “extremely” worse. This was significantly different between employee roles (Table 2), with highest reports among clinicians, 62% (n = 48) (Fig. 3). There were associations between those who agreed more on having all resources and equipment to work from home and those who previously shared office space with lower level of stress, but no associations with gender, age, or additional time demands for caregiving (Table 3).
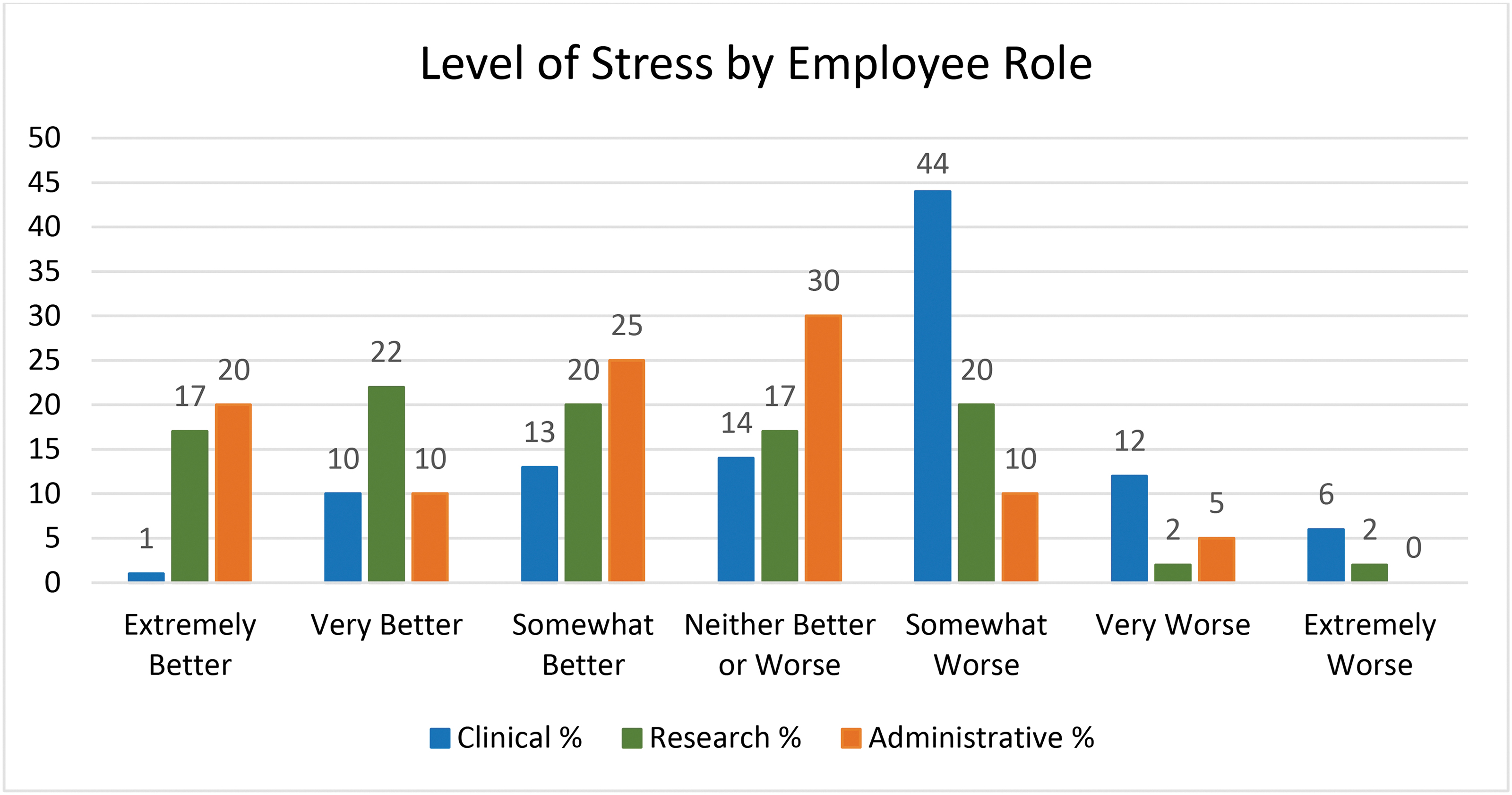
Bar graph of level of stress reported by employee role.
Discussion
In this anonymous survey, we found that employees of the PRIM department overwhelmingly supported working from home within the context of the COVID-19 pandemic. This positive reaction may have stemmed from concerns by most department members about becoming ill and social distancing, as reflected by those with shared office space. Many factors are needed to increase telework, from the availability of sufficient resources and equipment, including broadband Internet, to organizational scheduling and management trust and control. 12 Successful management of an environment with multiple telework schedules and in-person presence requires increased managerial planning as well. 11
Important in making PRIM's transition successful was ensuring that employees had all the resources and equipment needed to work from home. This may have been a challenge encountered by clinicians, who notably had the least positive experience. In fact, studies have found that, although not quite as effective as a face-to-face visit, inpatient and outpatient video visits can be a feasible method of delivering palliative care when necessary.18,19,22–28 PRIM department clinicians in the outpatient setting predominantly provided telemedicine visits, while the inpatient setting was divided into on campus and off campus teams.
However, providing empathic, high-quality, person-hood-driven palliative care by telemedicine meant navigating the availability of technological devices, Internet connection, difficulty with logging in to software, and communication adjustments, including being mindful of body language and interpretation of meaningful versus unintended silence. 26 Furthermore, inpatient telemedicine encounters faced challenges with the ability to connect with patients who were also receiving multiple in-person and virtual visits from other medical teams, undergoing diagnostics, sometimes did not answer phones, and other times were too ill or altered to conduct virtual visits. Although some clinicians were available in-person to provide care, this restricted remote work capabilities for the consulting service. It is possible that the less positive perceptions of clinicians reflect the burden of these challenges.
Workload experienced by the department was not reported to be significantly increased. However, the survey was conducted at the onset of the pandemic, when there was closure of clinical facilities, transition to telehealth, and some research projects on hold. The administrative group reported the highest increase in workload, possibly reflecting more interruptions to workflow and additional tasks due to new coordination of work virtually for the department.
A recent study by Reddy et al. 27 documented the transition of PRIM's supportive care clinic to virtual care and suggested that higher numbers of patients were seen post-transition and with fewer no-shows, as well as increased nonbillable encounters. More research is needed to better understand the changes in workload as the COVID pandemic continues to evolve and characterize the changes to monitor for work intensity and impact on productivity.
The challenges to work productivity and day-to-day stress due to the COVID-19 pandemic, felt by all employees (concern in becoming ill, safety of our families, increased family needs, worry about employment, ability to work, financial impacts), may have been somewhat mitigated by the department's ability to transition to work from home. Despite this, the study still revealed increased emotional exhaustion and stress levels, again worse among clinicians. This may be related to the challenges in a desire to balance keeping families safe with social distancing, caregiving needs at home, concerns over the ability to perform work as a result, while also attempting to deliver quality medical care with telemedicine.
Future studies detailing the changes in the pandemic as it relates to caregiving and financial impact on employees in relation to the unique aspects of each employee role's remote work experience may reveal how stress and emotional exhaustion have evolved over the course of the pandemic.
Burnout has been associated with decreased collaboration between leadership and an imbalanced workload. A study of the relationship between psychosocial variables and working conditions and distress during the 2003 SARS outbreak in Canada concluded that organizational supports congruent with health care workers' needs can reduce feelings of uncertainty and fear, in turn reducing symptoms related to burnout and improving health care delivery. 29
A recent study comparing burnout frequency among oncology physicians and nurses working on the frontline versus usual wards during the COVID-19 epidemic of Wuhan, China, showed that the frequency of burnout was actually significantly lower in the frontline group than the usual wards group; it was hypothesized that the usual wards group may have perceived less control over new policies and procedures enacted to keep staff and patients safe. 30 Safety of the work environment and supportive leadership are associated with higher job satisfaction among health care workers.31–33 The clinician response in this survey suggests that further research is needed examining factors related to increased stress reported during this pandemic 34 and its relationship with telework.
Conclusion
Major epidemics such as COVID and SARS are likely to become more frequent as global travel increases. The well-being and safety of employees are important in maintaining a healthy workplace in the face of global crisis and in the new normal thereafter. Significant changes in the year since the pandemic was declared include multiple peaks of infection and vaccination efforts. It will also be important to evaluate the impact of working from home under more usual conditions. We see from this survey that overall, working from home was received positively by the PRIM department.
However, some subgroups of individuals found working from home particularly distressing, and these may need additional support and solutions; clinicians may face different or more intensified stressors, and employees with significant home circumstances may need more flexibility in their work. Considerations may be needed for a hybrid model to optimize the best work environment or employ emerging technologies and work models to facilitate workplace well-being. Follow-up surveys are needed to track the progress of our work-from-home model, develop a more conclusive perception of the work-from-home transition, and find new solutions to maximize employee effectiveness.
The knowledge gained this time will help our team and others prepare for work-from-home situations. It is also likely that hybrid models of work will become more common, and our findings support the continuity of some work-from-home component as a permanent feature of palliative care programs.
Footnotes
Authors' Contributions
The authors confirm contribution to the study as follows.
Study conception, and design: E.B., N.S., A.E.A., J.B., M.Y.L., K.K.S., M.C., J.W., V.D.L.C., C.N., P.S., and Z.S.
Data collection: E.B., Y.R., M.H., P.S., Z.S., N.S., A.E.A., and J.B.
Analysis and interpretation of results: M.C., K.K.S., A.E.A., J.B., and E.B.
Draft article preparation: K.K.S., A.E.A., J.B., M.C., and E.B.
All coauthors have reviewed and approved of the article before submission.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
Appendix Table A1. Complete Survey Results of Employees' Perceptions of Work-from-Home Transition during COVID-19
| Total, n (%) | Employee role, n (%) | |||
|---|---|---|---|---|
| Clinical | Research | Administrative | ||
| My overall experience with working from home has been | ||||
| Extremely or very positive | 73 (53) | 30 (39) | 27 (66) | 16 (80) |
| Somewhat positive | 46 (34) | 31 (41) | 11 (27) | 4 (20) |
| Neither positive nor negative | 10 (7) | 7 (9) | 3 (7) | 0 |
| Somewhat negative | 5 (4) | 5 (7) | 0 | 0 |
| Extremely or very negative | 3 (2) | 3 (4) | 0 | 0 |
| Since COVID-19, my workload has | ||||
| Greatly increased | 21 (15) | 10 (13) | 7 (17) | 4 (20) |
| Increased somewhat | 41 (29) | 20 (26) | 14 (34) | 7 (35) |
| Neither increased nor decreased | 52 (37) | 28 (36) | 17 (41) | 2 (10) |
| Decreased somewhat | 22 (16) | 18 (23) | 2 (5) | 4 (15) |
| Greatly decreased | 3 (2) | 2 (3) | 1 (2) | 4 (20) |
| Compared with working on campus, I feel that when working at home I can be | ||||
| Extremely or very more productive | 45 (33) | 15 (20) | 17 (42) | 13 (65) |
| Somewhat more productive | 23 (17) | 12 (16) | 9 (22) | 2 (10) |
| Neither more nor less productive | 41 (30) | 26 (34) | 10 (24) | 5 (25) |
| Somewhat less productive | 23 (17) | 18 (24) | 5 (12) | 0 |
| Extremely or very less productive | 4 (3) | 4 (5) | 0 | 0 |
| I currently have all the resources and equipment I need to work from home | ||||
| Strongly agree or agree | 97 (71) | 50 (66) | 33 (81) | 14 (70) |
| Neither agree nor disagree | 14 (10) | 7 (9) | 4 (10) | 3 (15) |
| Strongly disagree or disagree | 25 (18) | 18 (24) | 4 (10) | 3 (15) |
| For me, working from home is emotionally | ||||
| Extremely or very positive | 74 (54) | 34 (45) | 26 (64) | 14 (70) |
| Somewhat positive | 34 (25) | 21 (28) | 9 (22) | 4 (20) |
| Neither positive nor negative | 19 (14) | 13 (17) | 4 (10) | 2 (10) |
| Somewhat negative | 7 (5) | 6 (8) | 1 (2) | 0 |
| Extremely or very negative | 2 (2) | 1 (1) | 1 (2) | 0 |
| Compared with before the COVID-19 crisis, in the last two months my level of stress has been | ||||
| Extremely or very better | 31 (22) | 9 (11) | 16 (39) | 6 (30) |
| Somewhat better | 23 (17) | 10 (13) | 8 (20) | 5 (25) |
| Neither better nor worse | 24 (17) | 11 (14) | 7 (17) | 6 (30) |
| Somewhat worse | 44 (32) | 34 (44) | 8 (20) | 2 (10) |
| Extremely or very worse | 17 (12) | 14 (18) | 2 (4) | 1 (5) |
| For me, working from home is financially | ||||
| Extremely or very positive | 79 (58) | 30 (39) | 34 (83) | 15 (75) |
| Somewhat positive | 24 (18) | 17 (22) | 3 (7) | 4 (20) |
| Neither positive nor negative | 31 (23) | 27 (36) | 3 (7) | 1 (5) |
| Somewhat negative | 2 (1) | 1 (1) | 1 (2) | 0 |
| Extremely or very negative | 0 | 0 | 0 | 0 |
| For me, being asked to work partially or completely from home permanently is | ||||
| Extremely or very positive | 64 (46) | 27 (34) | 23 (56) | 14 (70) |
| Somewhat positive | 32 (23) | 19 (24) | 9 (22) | 4 (20) |
| Neither positive nor negative | 22 (16) | 15 (19) | 5 (12) | 2 (10) |
| Somewhat negative | 13 (9) | 11 (14) | 2 (5) | 0 |
| Extremely or very negative | 8 (5) | 6 (8) | 2 (5) | 0 |
| From my perspective, keeping social distance is | ||||
| Extremely or very important | 129 (93) | 74 (95) | 38 (93) | 17 (85) |
| Somewhat important | 7 (5) | 3 (4) | 2 (5) | 2 (10 |
| Neither important nor unimportant | 2 (1) | 1 (1) | 1 (2) | 0 |
| Somewhat unimportant | 0 | 0 | 0 | 0 |
| Extremely or very unimportant | 0 | 0 | 0 | 0 |
| In general, were I to come to work at the MD Anderson campus today, I would feel | ||||
| Extremely or very safe | 35 (25) | 24 (31) | 8 (19) | 3 (15) |
| Somewhat safe | 55 (40) | 35 (45) | 15 (37) | 5 (25) |
| Neither safe nor unsafe | 9 (6) | 6 (8) | 2 (5) | 1 (5) |
| Somewhat unsafe | 21 (15) | 8 (10) | 6 (15) | 7 (35) |
| Extremely or very unsafe | 19 (14) | 5 (6) | 10 (24) | 4 (20) |
| With the current understanding of spatial needs for proper social distancing, if I were to come to work today in the department's office at MD Anderson, I would find my current working space | ||||
| Extremely or very safe | 57 (41) | 35 (45) | 15 (36) | 7 (35) |
| Somewhat safe | 31 (22) | 18 (23) | 8 (20) | 5 (25) |
| Neither safe nor unsafe | 4 (3) | 3 (4) | 0 | 1 (5) |
| Somewhat unsafe | 26 (19) | 12 (15) | 9 (22) | 5 (25) |
| Extremely or very unsafe | 20 (15) | 9 (12) | 9 (22) | 2 (10) |
| Overall, my level of concern in becoming ill due to the spread of COVID-19 in the community is | ||||
| Extremely or very concerned | 73 (53) | 37 (48) | 22 (54) | 14 (70) |
| Somewhat concerned | 52 (37) | 34 (44) | 13 (32) | 5 (25) |
| Neither concerned nor unconcerned | 6 (4) | 4 (5) | 2 (5) | 0 |
| Somewhat unconcerned | 2 (1) | 1 (1) | 1 (2) | 0 |
| Extremely or very unconcerned | 5 (4) | 1 (1) | 3 (7) | 1 (5) |
| Due to COVID-19, I have more concerns regarding my employment | ||||
| Strongly agree or agree | 95 (68) | 49 (63) | 31 (76) | 15 (75) |
| Neither agree nor disagree | 25 (18) | 17 (22) | 7 (17) | 1 (5) |
| Strongly disagree or disagree | 19 (14) | 12 (15) | 3 (7) | 4 (20) |
| Due to COVID-19, I have more concerns regarding my ability to perform work | ||||
| Strongly agree or agree | 30 (21) | 21 (27) | 8 (19.5) | 1 (5) |
| Neither agree nor disagree | 30 (22) | 17 (22) | 8 (19.5) | 5 (25) |
| Strongly disagree or disagree | 79 (57) | 40 (51) | 25 (61) | 14 (70) |
| Due to COVID-19, I have more concerns regarding the health and safety of my family | ||||
| Strongly agree or agree | 125 (90) | 71 (91) | 36 (88) | 18 (90) |
| Neither agree nor disagree | 7 (5) | 4 (5) | 2 (5) | 1 (5) |
| Strongly disagree or disagree | 7(5) | 3 (4) | 3 (7) | 1 (5) |
| Due to COVID-19, I have more concerns regarding my finances | ||||
| Strongly agree or agree | 87 (62) | 50 (64) | 23 (56) | 14 (70) |
| Neither agree nor disagree | 39 (28) | 21 (27) | 14 (34) | 4 (20) |
| Strongly disagree or disagree | 13 (9) | 7 (9) | 4 (10) | 2 (10) |
| Since COVID-19, I have additional demands on my time due to closure of schools or care facilities for my children or adult dependants | ||||
| Strongly agree or agree | 79 (57) | 47 (60) | 21 (52) | 11 (55) |
| Neither agree nor disagree | 29 (21) | 17 (22) | 10 (24) | 2 (10) |
| Strongly disagree or disagree | 31 (22) | 14 (18) | 10(24) | 7 (35) |
| Since COVID-19, my emotional exhaustion has | ||||
| Greatly increased | 25 (18) | 18 (23) | 4 (10) | 3 (15) |
| Increased somewhat | 70 (50) | 38 (49) | 23 (56) | 9 (45) |
| Neither increased nor decreased | 30 (22) | 17 (22) | 6 (15) | 7 (35) |
| Decreased somewhat | 13 (9) | 5 (6) | 7 (17) | 1 (5) |
| Greatly decreased | 1 (1) | 0 | 1 (2) | 0 |