
Abstract
Background:
Pediatric nurses are particularly vulnerable to moral distress and turnover due to frequent experiences with patient death combined with limited pediatric palliative resources and related support.
Objective:
This study examined pediatric nurses' experiences of pediatric patient death, moral distress, and turnover intention and identified the correlations between them as well as the mediating role of moral distress.
Methods:
This cross-sectional study conducted an online survey with 161 pediatric nurses working in a tertiary hospital in Seoul, South Korea. The survey comprised questions to assess nurses' experience of pediatric patient death and turnover intention and a validated instrument to measure their moral distress. Logistic regression was used to examine the relationships between study variables, and structural equation modeling was performed to determine the mediating effect of moral distress.
Results:
Pediatric nurses (N = 161) reported high levels of moral distress with a mean score of 101.06 (standard deviation = 70.528) on the pediatric version of the Moral Distress Scale. Turnover intention increased 1.01 times for every 1 U increase in moral distress. Moral distress fully mediated the relationship between the experience of pediatric patient death and turnover intention.
Conclusion:
Pediatric patient death had an indirect effect on turnover intention through moral distress among pediatric nurses. Reducing pediatric nurses' moral distress caused from experiencing patient death may help minimize their turnover intention.
Introduction
Nurses vividly recall and are significantly impacted by memorable patient deaths. 1 In particular, witnessing pediatric patient deaths is emotionally and ethically challenging and may cause nurses to experience grief, feelings of inadequacy, helplessness, or distress.2–4 Such emotional reactions may transform into moral distress in situations of high patient mortality and constrained or conflicting clinical situations. 5 Campbell et al. 6 defined moral distress as “the one or more negative self-directed emotions or attitudes that arise in response to one's perceived involvement in a situation that one perceives to be morally undesirable” (p. 6).
Many studies have revealed that nurses' moral distress influences their turnover intention.7–9 Nurses' turnover has a negative impact on the quality of care and patient safety as well as the financial performance of the health care system. 10
In South Korea, the turnover rate of nurses within one year after graduation is ∼25%, which increases to 50% within the first five years.8,11 In particular, the turnover intention of pediatric nurses in the neonatal intensive care unit (NICU) is 72.4%, 12 which may be due to high mortality in tertiary hospitals and moral distress caused by a lack of experts and resources to care for dying pediatric patients. In Korea, pediatric nurses in tertiary hospitals often experience pediatric patients' death.
In 2018, 81% of deaths of children under 15 years of age occurred in hospital settings. 13 Furthermore, 21 (50%) out of 42 tertiary hospitals in Korea are located in the Seoul metropolitan area, 14 and ∼47% of deaths of children <19 years of age occur in this area. 15 As such, pediatric nurses working in the tertiary hospitals in this area care for a high volume of dying.
As pediatric nursing's fundamental philosophy is patient and family-centered care, 16 the nurses have a strong attachment toward the pediatric patients and form close relationships with their families. Although such attachments and relationships can facilitate quality nursing in pediatric palliative care, 17 it can also make pediatric nurses vulnerable to moral distress, and they may experience ethical conflicts due to the close relationships.18,19 For example, nurses often experience emotional distress when they disagree with the parents regarding the best treatment for the pediatric patients. 20 Nurses experience moral distress when aggressive treatments that they considered futile need to be provided to children because of the physician's order or parents' wishes, and when there is a lack of continuity in care or limited communication among health care professionals.19–21
With the advancement of medical technology, nurses often experience conflict related to aggressive life-sustaining treatments, which may not be in the best interest of the child. 21 Repeated exposure to distressed situations damages nurses' moral integrity and causes desensitization to moral issues. 22 In particular, pediatric nurses experience stress, emotional burnout, and turnover intention when they witness pediatric patients' pain and death 23 and provide aggressive end-of-life care. 19 As such, it is important to examine pediatric nurses' moral distress in detail and the correlations between pediatric nurses' experience of patient deaths, moral distress, and turnover intention.
Although the Act on Decisions on Life-sustaining Treatment for Patients in Hospice and Palliative Care or at the End of Life was enacted in 2016 and came into force in 2018, such care for children has received little attention in Korea to date. 24 Of the 107 institutions that provide hospice and palliative care services, only 9 provide pediatric services. 25 Therefore, this study examines the status of Korean pediatric nurses' experience of pediatric patient death, moral distress, and turnover intention and identifies the relationships among these factors to determine the mediating role of moral distress in the relationship between the experience of pediatric patient death and turnover intention. Finally, this study recommends potential interventions that could decrease pediatric nurses' turnover intention.
Materials and Methods
Study design and sample
This study employed a cross-sectional design using an online survey to examine nurses' experiences of pediatric patient deaths, moral distress, and turnover intention in a tertiary hospital in Seoul, Korea. The inclusion criteria of the sample were being a registered nurse who provides direct care to pediatric patients and works in a targeted tertiary hospital. The exclusion criterion was having less than six months of work experience as a registered nurse. A total of 192 nurses responded to the survey.
Of these, 31 were excluded due to incomplete responses, resulting in a sample pool of 161 responses. The response rate was not calculated, as it was impossible to determine the number of people who viewed the survey link or QR code but did not start the survey. The questionnaire carried a statement specifying that it was only for pediatric nurses of the targeted hospital. It was confirmed that there were no duplicate responses in the process of paying compensation worth 10 dollars later.
Data collection
The pediatric nurses were recruited using convenience and snowball sampling methods, and data were collected from October to December 2020. The survey was developed and conducted online to protect nurses' privacy and to facilitate data collection regardless of physical accessibility limitations such as nurses' shift schedules and COVID-19 restrictions. The study's first recruitment was conducted at a palliative care promotion session for pediatric nurses at a hospital. The study purpose, procedures, and methods were introduced at the end of the session.
A QR code and a hyperlink for the online survey were provided to the attendee nurses by displaying them on the screen. To facilitate the study recruitment, the palliative care team of the hospital sent an SMS with the link to the survey to the session participants. In addition, the attendee nurses were encouraged to share the survey link or QR code with their colleagues who met the eligibility criteria.
This study was approved by the institutional review board (IRB) of the university (No. MIRB-sin20200819-001). The first page of the online survey provided a description of the study, including purpose and study methods, voluntary participation, the right to withdraw from the study at any time, and the anonymity of data collection and management. As the research involved no more than minimal risk and no identifiable information, and thus, would not affect the participant's welfare, the participant's consent form was not obtained, as per the IRB's approval. However, if the participants clicked on the “next” button on the first page of the survey, it was deemed that they agreed to participate in the study.
Measures
Based on the theory of moral distress by Corley, 26 predictor, mediator, and outcome concepts were determined and measured using questions and a validated instrument.
General characteristics
Demographic characteristics such as age, gender, presence of child(ren), work experience (in years), working unit, and training experience in palliative care/pediatric palliative care were obtained.
Predictor: Experience of pediatric patient death
Participants were asked whether they had experienced pediatric patient death during their career, which was answered as “yes” or “no.” In addition, participants reported the number of pediatric patient deaths experienced during their careers.
Mediator: Moral distress
Moral distress was measured using the pediatric version of the Moral Distress Scale-Revised (MDS-R). The MDS-R consists of 21 questions regarding the frequency of the encountered situation and the intensity of moral distress. The frequency and intensity scales range from 0 (never) to 4 (very frequently) and from 0 (none) to 4 (great extent), respectively. The total score is obtained by adding the frequency scores and multiplying the obtained number by intensity (frequency × intensity). Scores range from 0 to 336. The Cronbach's alpha of the original tool was 0.88, 27 and that of the Korean version was 0.91. 12 In this study, the Cronbach's alpha was 0.93.
Outcome: Turnover intention
Turnover intention was assessed by asking participants whether they intended to leave their current job, with “yes” and “no” options available.
Data analysis
Data analyses were performed using STATA version 15.0 software (Stata Corp LP, College Station, TX), and the significance level was set at 0.05. Participants' general characteristics, experience of pediatric patient death, moral distress, and turnover intention were described using means, standard deviations (SDs), frequencies, and percentages. The t test, one-way analysis of variance, and chi-square test were used to explore differences within study variables based on participant characteristics.
Logistic regression was used to examine the relationship between the experience of pediatric patient death, moral distress, and turnover intention among pediatric nurses, controlling for general characteristics. Structural equation modeling was performed to determine the mediating effect of moral distress on the relationship between the experience of pediatric patient death and turnover intention. The number of bootstrapping samples was 5000, with a 95% confidence interval (CI).
Results
The characteristics of the participants are summarized in Table 1. The average age of the participants was 33.31 ± 7.45 years. Most of the participants were women (97.5%), and 62.1% had no children. The mean number of years of work experience as a registered nurse was 9.32 ± 7.64 years, with 44.1% of the participants having worked as registered nurses for >10 years. The most common working unit was the intensive care unit (30.4%), followed by the general ward (28.6%), outpatient unit (21.7%), emergency room (14.3%), and others such as intravenous therapy team or hospice centers.
General Characteristics of Participants (N = 161)
M, mean; PC, palliative care; PPC, pediatric palliative care; SD, standard deviation.
Most of the participants had experienced pediatric patient death (83.2%). Over half of the participants (56.7%) had experienced 6 or more pediatric patient deaths, and approximately one-third (38.8%) had experienced >11 pediatric patient deaths. Approximately 15.5% of the participants had received pediatric palliative care education, whereas the majority had not (84.5%). The mean score for moral distress was 101.06 (SD = 70.53). Approximately 61.5% of the participants reported that they planned to leave their current job.
The top five ranked moral distress items, as given in Table 2, were “Carrying out unnecessary physician's orders” (8.46 ± 5.98), “Work with unsafe providers” (7.89 ± 6.57), “Lack of provider continuity” (7.78 ± 6.26), “Unwillingly continuing life support due to family wishes” (7.04 ± 5.45), and “Continuing to provide hopeless care due to a lack of decision to withdraw support” (6.95 ± 5.90).
Scores and Ranks of Moral Distress Items Among Pediatric Nurses (N = 161)
The number of pediatric patient deaths experienced was significantly correlated with the level of moral distress (r = 0.262, p = 0.002). The results of logistic regression are presented in Table 3. For every 1 U increase in moral distress, there was 1.01 times higher turnover intention among pediatric nurses after controlling for other variables (odds ratio [OR] = 1.01, 95% CI = 1.001–1.012). There was no statistically significant correlation between the experience of pediatric patient death and turnover intention among pediatric nurses after controlling for other variables (OR = 0.48, 95% CI = 0.160–1.449).
Logistic Regression Model for Turnover Intention Among Pediatric Nurses (N = 161)
Values were adjusted for participants' general characteristics, including age, gender, and presence of children, work experience, training experience in PC, and training experience in PPC.
CI, confidence interval.
The mediating effects of moral distress on the relationship between the experience of pediatric patient death and turnover intention are shown in Figure 1. The experience of pediatric patient death had no effect on turnover intention (p = 0.186). The experience of pediatric patient death had a positive association with moral distress (p = 0.001), and moral distress had a positive effect on turnover intention (p = 0.003). The indirect effect of the experience of pediatric patient death was significant (β = 0.067, Boot CI = 0.012–0.122). Therefore, moral distress had a complete mediating effect on the relationship between the experience of pediatric patient death and turnover intention.
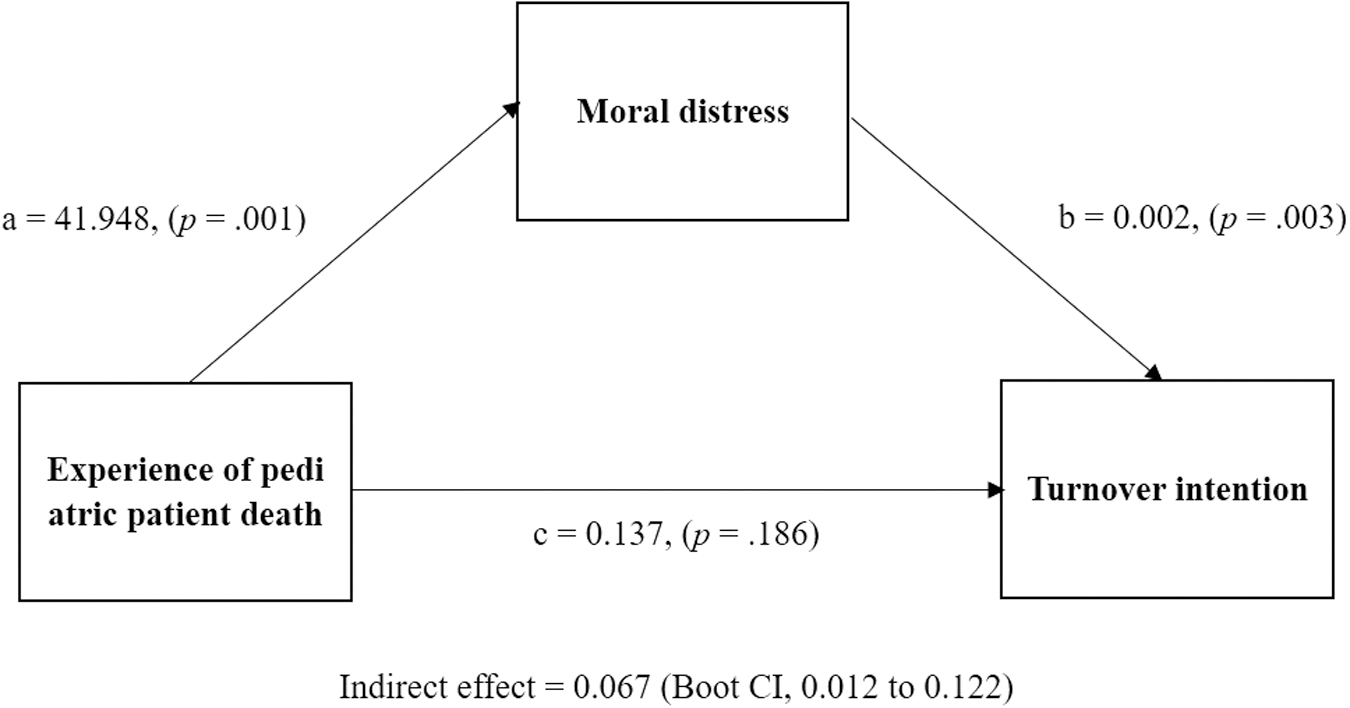
Mediating effects of moral distress on relationship between the experience of pediatric patient death and turnover intention.
Discussion
This study examined nurses' experiences of pediatric patient death, moral distress, and turnover intentions at a tertiary hospital in South Korea and explored the correlation between these factors. A previous study reported that new nurses felt unprepared to experience the death of a pediatric patient. 28 Although this study included participants with experience ranging from 6 months to >10 years, the rate of nurses' experience of pediatric patient death was high (83.2%), but only ∼15% had received palliative care education. This raises serious concerns about the lack of preparation of pediatric nurses in providing quality palliative care to children and their families and coping with patient deaths and resultant moral distress.
This study revealed that pediatric nurses in Korea experience high moral distress (101.06 ± 70.528). Previous studies using the same instrument found similar rates of moral distress among Iranian pediatric nurses (106.41 ± 61.64) 18 and significantly lower rates among intensive care unit (96.5 ± 55.8) 29 and pediatric nurses (47.3) in the United States. 21 Previous research 30 revealed slightly higher moral distress rates among NICU nurses in Korea (108.37), where each item's score distribution was similar to that of this study. For instance, three of the five top-ranked items were the same.
Therefore, previous research combined with the present results suggests that pediatric nurses tend to experience moral distress when they cannot provide what they consider optimal care due to external constraints. In addition, pediatric nurses' reported turnover intention was 61.5%, which was higher than the reported rates in other countries, including 44.3% in New Zealand, 26.8% in the United States, 19.9% in Canada, and 15.1% in Australia. 10 As Korean pediatric nurses experience high volumes of patient deaths, moral stress, and turnover intention without adequate preparation in providing palliative care, it was crucial to examine the inter-relationships among these factors to better understand their relationships and investigate factors that can decrease the pediatric nurses' moral distress and turnover intentions.
This study indicated that the experience of pediatric patient death influenced the moral distress of pediatric nurses. Nurses, as health care providers, are expected to provide intimacy and compassionate care for patients over time. Pediatric nurses experience great stress when faced with the death of the patient while emotionally intervening with the patient by forming a deep attachment through long-term care. 31 Although experiences of patient death can negatively affect nurses' attitudes during care, 1 controlling mortality at tertiary hospitals in metropolitan areas in Korea is challenging due to the centralization of human resources and medical technology as well as severity of patient concerns.
In some cases, the death of pediatric patients is uncontrollable and inevitable. Therefore, interventions and strategies to reduce moral distress among nurses who frequently experience pediatric patient deaths must be developed. In addition, an understanding of specific factors that cause moral distress among pediatric nurses, which differ from adult patient settings, must be established and considered when managing nurses' moral distress.
This study demonstrated that nurses' turnover intention was indirectly influenced by pediatric patient death experience and directly influenced by moral distress, and that moral distress was impacted by patient death experience. However, mediating factors with characteristics other than moral distress could not be identified. These results are in line with previous studies, which revealed a significant positive correlation between moral distress and turnover intention among nurses.9,32 This study indicated that managing the high moral distress of pediatric nurses could help reduce nurses' turnover intentions. Therefore, institutions should intervene to decrease nurses' moral distress to avoid the consequences of nurses' turnover.
Strategies helping pediatric nurses to cope with pediatric patient death are essential to decrease moral distress. Early detection of moral distress, 33 organizational commitment and engagement,34,35 ethics education, 36 mindfulness, 37 and the creation of pediatric palliative care teams within hospital units 38 were found to be effective in decreasing moral distress. In terms of palliative care ability, moral distress was affected by nurses' competences in palliative care.39,40 Therefore, strengthened competency in palliative care would help reduce the level of moral distress among pediatric nurses who experience patient deaths and their turnover intention.
Developing and providing systematic and pediatric-appropriate education may improve nurses' ability to cope with palliative care situations.41,42 Moreover, education and consulting services could help nurses develop positive attitudes. 43 For instance, peer storytelling using an online platform to illuminate nurses' implicit and explicit thoughts, feelings, and responses after a patient's death was found to be helpful in resolving nurses' grief. 44
Korea is in the initial stages of developing a pediatric palliative care system. Korea's health insurance system has not yet been developed to include pediatric palliative care service, and shortage of nurses is an ongoing problem in Korea. Consequently, pediatric nurses continue to be burdened with the emotional and physical responsibilities of caring for dying pediatric patients. Experiencing such unavoidable conditions frequently without adequate support and education is challenging for nurses. In addition, these situations may inadvertently compromise patient outcomes and influence nurses' turnover intention.
Therefore, it is crucial for nursing management and institutions to provide psychological support to pediatric nurses in cases of patient death and moral distress relief plans through pediatric palliative care education. In addition, the development of supporting systems such as pediatric palliative care experts and referral systems for hospice care teams could assist nurses in coping with pediatric patient death.
This study has some limitations. First, a causal relationship among the variables could not be confirmed due to the cross-sectional design of this study. Second, this study was conducted at a single tertiary hospital. Therefore, the generalizability of the study findings is limited. However, it was meaningful to survey most pediatric nurses in one institution. To increase generalizability, future studies should use random sampling with a larger pool of pediatric nurses from various hospitals. Finally, the used instruments might not fully reflect the concepts we intended to explore.
Although MDS-R contains many items of moral distress related to end-of-life care situations, it also includes items related to other situations. In addition, nurses' turnover intention was investigated through a question that asked respondents' subjective turnover intentions. Examining objective data such as institutional turnover rate may provide various perspectives, which could be compared with subjective answers to obtain more information.
Conclusion
This study provided insight into the moral distress of pediatric nurses, which has not been studied extensively in the past, and confirmed the correlation between moral distress and experience of pediatric patient death and turnover intention. Pediatric nurses often care for dying children, and such experiences cause moral distress, which can lead to turnover intention. The death of a pediatric patient is sometimes inevitable. However, interventions that prepare pediatric nurses for the difficult experiences or that reduce their moral distress may help mitigate the threat of turnover. Health care institutions should provide appropriate education and support, such as education on pediatric-focused palliative care, ethics, or critical thinking, and stress management programs for pediatric nurses.
Footnotes
Authors' Contributions
Conception and design of the study were done by all authors; data analysis was taken care by A.M. and S.K.; interpretation of results was by all authors; drafting of article was done by all authors; revising article critically for important intellectual content was taken care by S.G.J. and S.K.; final article approval for publication was by all authors; and accountability for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved was by all authors.
Acknowledgments
The authors wish to acknowledge all the nurses for participating in the survey.
Funding Information
This research was supported by the Catholic Medical Center Research Foundation made in the program year of 2020.
Author Disclosure Statement
The authors declare that there are no conflicts of interest. The research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.