
Abstract
Background:
The Serious Illness Care Program has been shown to improve quality and feasibility of value-based end-of-life conversations in primary care.
Objectives:
To elicit patients' perspectives on serious illness conversations conducted by primary care clinicians.
Subjects and Methods:
Telephone interviews were conducted with patients at an academic center in the United States, who had a recent serious illness conversation with their primary care clinician. Interviews were audio-recorded and qualitatively analyzed using thematic analysis.
Results:
A total of eleven patients were enrolled. We identified three major themes: (1) positive emotional experiences are facilitated by established patient-clinician relationships and/or clinicians' skills in navigating emotional challenges, (2) patients appreciate a personalized conversation, and (3) clinicians should orchestrate the experience of the conversation, from preparation through follow-up.
Conclusion:
Patients appreciate having serious illness conversations in the primary care setting. Future efforts can be focused on improving clinicians' skills in navigating emotional challenges during conversations and implementing system changes to optimize orchestration.
Introduction
Preferences for medical care at the end of life are not fixed, but emerge through a process of discussion and reflection centered on patients' important relationships, values, and goals.1,2 The Serious Illness Care Program, which includes a structured serious illness conversation guide, communication training, and electronic medical record (EMR) modification, has been shown to improve the quality and feasibility of such conversations,3,4 yet there are limited data about patients' experiences. In the oncology setting, when approached by clinicians trained in the program, patients are open to discuss emotionally challenging topics and articulate their preferences 5 ; patients also report significant reductions in anxiety and depression, as well as enhanced future care planning post-conversation.6,7
To our knowledge, current literature has not explored patients' experiences of serious illness conversations in primary care. Different from oncology patients, patients in primary care may live with multiple advanced chronic diseases that evolve over time, often with a less predictable disease trajectory and more ambiguity around prognosis. To further the understanding of patients' experiences with serious illness conversations, our study uses a qualitative approach to elicit the perspectives of primary care patients.
Materials and Methods
The study was approved by Partners Human Research Committee. Patients were eligible if they were >18 years of age, English-speaking, and able to recall having had a serious illness conversation at two selected primary care practices. The two practices were located in downtown Boston and served a predominantly English-speaking, White population. Clinicians in these practices received training in 2017–2018 to use the serious illness conversation guide. The training sessions were 2.5 hours and included both didactics and small group practice, with actors led by communication facilitators. Training details and the serious illness conversation guide used for this study have been published elsewhere. 8
The incorporation of a serious illness conversation into workflow varied by clinicians, who were given flexibility to either include it in a routine visit or schedule a separate visit. Clinicians were trained to tailor the conversation to the patient's information preferences and ability to cope, and to document the conversations using a dedicated template in the EMR.
To enroll patients in the study, research staff used a weekly EMR-generated report of patients who had a conversation. The patient's primary care clinician was contacted to identify and exclude patients who could not participate in the phone interview due to cognitive impairment, language barriers, or psychosocial concerns. Eligible patients were then contacted for enrollment by a letter, followed by a phone call. Patients were excluded if the conversation occurred more than five weeks before a phone interview could be conducted. (The authors estimated that five weeks would allow sufficient time for enrollment, while the serious illness conversation remained relatively fresh in patients' memory.) All patients at the participating sites were eligible for screening; however, to maximize variation, up to two patients from each clinician's panel were enrolled.
An interview guide containing 12 open-ended questions was independently developed by the research team with guidance from a patient advocate (C.M.) and the Patient and Family Advisory Council (Supplement Data S1). The phone interview was designed to be semistructured to flexibly assess patients' perspectives of serious illness conversation. Two researchers (J. J. and L.X.) conducted interviews after obtaining consent from participants. Interviews were recorded and transcribed.
A convenience sample of 20 interviews was targeted at the inception of the study. Eleven interviews were conducted between July 2019 and February 2020, and the study was halted due to the COVID-19 pandemic. At that point, the authors identified that the final two interviews did not yield new information, suggesting that data saturation was reached. 9 The authors also felt that further interviews would have been heavily influenced by patients' experiences of the pandemic and not necessarily comparable to the prepandemic interviews.
Thematic analysis was performed, given the approach's several advantages, including the ability to highlight similarities and differences of participants' perspectives as well as generate unanticipated insights.10,11 Two researchers (J.J. and L.X.) separately sorted segments of interview transcripts into unifying themes and subthemes using an inductive iterative approach, 12 until all variations were accounted for. The two researchers then compared findings and iteratively revised themes and subthemes. Disagreements were discussed between the two researchers first and then shared with the research team to reach consensus.
Results
Fifty-seven patients were screened for eligibility and 32 patients were approached (Fig. 1). A total of 11 participants from the panels of 9 different clinicians were enrolled, between 61 and 92 years of age (median = 81 and standard deviation = 8.6). Six were female and ten were White. Frequencies of each serious illness conversation component documented in chart were extracted from the medical records. Clinicians discussed patients' illness understanding (10 out of 11), hopes (9 out of 11), worries (8 out of 11), most important goals, values, and priorities (10 out of 11) and made recommendations (10 out of 11). Notably, only 3 out of the 11 conversations covered prognostic information. We identified three major themes through qualitative analysis of the interviews.
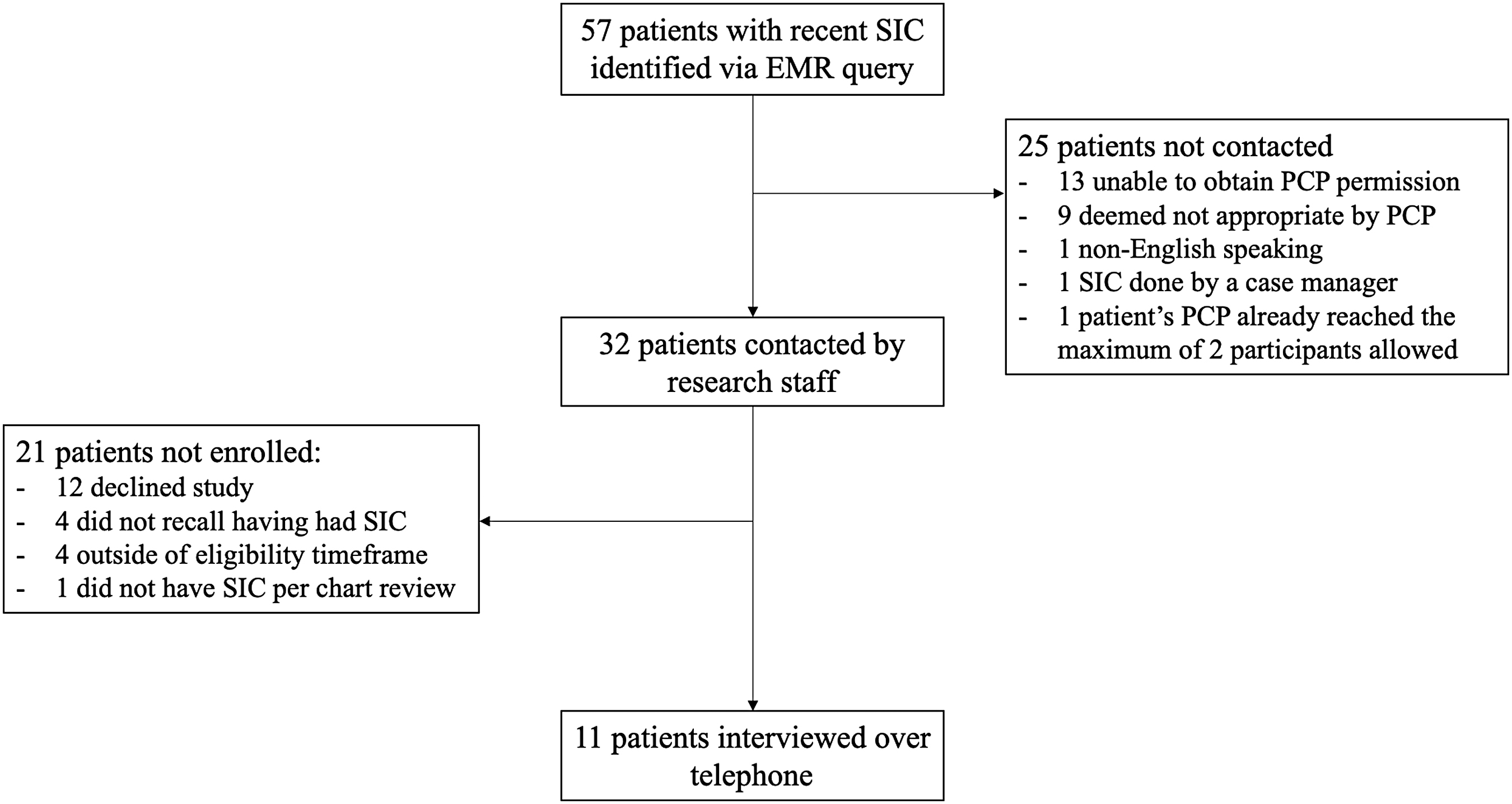
Flow chart of patient enrollment for semistructured telephone interview. EMR, electronic medical record; PCP, primary care physician; SIC, serious illness conversation.
Positive emotional experiences are facilitated by established patient-clinician relationships and/or clinicians' skills in navigating emotional challenges
Nearly half of the patients reported that an established relationship with their clinicians helped them to share more openly: “I can say things to [Dr. S] that I might be hesitant to say to someone I don't know that well.” Several patients reflected that the presence of an entrusted provider created a safe environment where they could speak freely, and described their emotions as “reassured,” “calm,” “not frightened,” and “less anxiety, more relaxed.” Moreover, the conversations also strengthened the patient-clinician alliance, as a patient reflected, “[The conversation] was another step in the bonding process that [Dr. L] and I had been going through.”
When asked for advice to improve the conversations, several patients acknowledged that a conversation could be an emotionally sensitive experience for both patients and clinicians: “It's hard for providers to get patients to talk about it, and then the other way around, it's hard for patients to get doctors to talk about it.” Another patient commented, “Some doctors may be very uncomfortable with [the conversation] and do a poor job of it.” Patients pointed out that clinicians should develop specific skills to navigate the emotional turmoil during the conversation not only for the patients but also for the clinicians themselves: “It takes a really good doctor to have this type of conversation without being morbid… Train your doctors to be themselves, relaxed and not excited about what they're talking about, and to get his or her patient to be in a calm, thoughtful, mindful way of listening and discussing.”
Patients appreciate a personalized conversation
Many patients emphasized that it was essential for the clinicians to listen and understand each patient as a unique individual, instead of treating patients as “cookie-cutter people,” “a production line,” or “a checklist.” The importance of shared decision making was a recurrent subtheme: “I have never liked being forced to agree to something…[Dr L] will listen to all of my views on things and when I have strayed off the path, she will tell me so.” Patients greatly appreciated conversations that explored their values and reasoning behind decisions: “Dr. H really wanted to know beyond just recording what my wishes were… and truly understand the background of why.” When asked if the use of a conversation guide affected the personalized experience, one patient commented on the free-flowing nature of the conversation: “It sounds like it was conversational. You could tell he was following a format but it felt very personalized.”
Clinicians should orchestrate the experience of the conversation, from preparation through follow-up
Collectively, patients provided feedback on how coordinating and planning each part of the conversation enhanced effective communication.
For preparation, some patients expressed preference for advance notice of the purpose of the conversation, so that they could prepare themselves or make plans to bring loved ones: “My daughter came with me to have that conversation… it was a very calm and gentle meeting. I am not excited about [the meeting]. I'm not depressed or worried or anything like that about it.” Having a few questions to prompt thinking before the visit was also helpful for some.
During the conversation, patients commonly emphasized the importance of having dedicated time to facilitate deeper introspection of values and beliefs, so that they could “concentrate their thinking,” “not feel pressured by time,” and “focus on doing this without interruption.” Some patients acknowledged that it often took more than one visit to fully explore their goals and priorities, and stressed the importance of follow-up visits when additional questions arise or when the patient feels ready for further discussion: “I haven't asked for a timeline. I think it's too soon… maybe when everything's in place, I'll ask them.”
For follow-up after the conversation, patients commonly expressed desire to communicate their thoughts to loved ones: “I have to put that in writing…I would like to make it as easy for [my family] as possible.” Another patient found the structure of the serious illness conversation helpful in discussing with family members afterward: “The conversation has helped me explain it to [my daughter] and other people who care about me…I was able to remember the scene from the play and structure it.”
Discussion
Our study shows that primary care can be a desirable setting for serious illness conversations. A close relationship with the clinician increases the depth and openness of conversations, while the conversations in turn further strengthen the patient-clinician relationship. These findings are consistent with previous literature showing patients' emotional readiness for serious illness conversations enhances their satisfaction with it, and that the patient-clinician relationship plays a key role.13–16 Patients also appreciated a dedicated time and safe space to focus on themselves and deliberate their priorities. The conversations brought a sense of empowerment and increased control over medical decisions, which was similarly reported in oncology patients' experiences. 7
Previous studies suggested that primary care clinicians face numerous barriers to effectively conduct serious illness conversations, including discomfort with discussing prognosis, lack of clarity about appropriate timing to initiate conversations, and challenges with care coordination and integrating conversations into workflow. 17 Even using the Serious Illness Care Program, previous work shows oncology providers continue to have difficulty in responding to emotional or ambiguous patient statements or discussing prognosis, 5 a finding that echoed observations in our study. Patients in our study keenly observed that conversations could be emotionally uncomfortable for both themselves and their clinicians, posing another barrier to effective communication.5,18
Despite some emotional discomfort, patients found the serious illness conversations to be personalized and valuable. When clinicians use the guide effectively, the scripting “disappears” and instead the conversation emerges as a structured exploration of patients' unique experiences and individual preferences. Previous study has also shown the guide to be acceptable to clinicians, decreasing anxiety about conversations and increasing role satisfaction. 7 Advanced serious illness conversation training might place more emphasis on responding to patients' emotions as well as help clinicians to reflect and react on their own discomfort during the conversations.
Our findings also emphasized the importance of optimizing a conversation's impact through orchestration. This includes a well-coordinated team effort to help patients mentally prepare, to set aside time in the clinician's schedule, and to ensure adequate follow-up through phone calls or in-person visits. 14 Fear of burdening loved ones or difficulty in initiating follow-up conversations with family are common barriers reported by patients in previous studies.15,19 Our findings suggest that facilitating family presence during the conversations and providing guidance for patients to communicate preferences to loved ones are important areas to focus on when orchestrating conversations.
Our study has several limitations. First, it was a small sample of predominantly Caucasian, English-speaking patients, which reflected the population served at the participating practices, so the results may not represent the perceptions of patients from diverse backgrounds. Second, there is likely selection bias toward patients who had positive experiences as the study excluded those who did not recall having the conversation, declined enrollment in the study, or were deemed not appropriate for participation by their primary care clinician; the reasons behind the patient's or clinician's decision not to participate were not recorded. Third, we did not collect clinical information about patients' illness trajectory, so we do not know how the experience of the conversation might have been impacted by patients' health experience. For example, a patient with new and significant functional decline might experience a conversation differently from a stable patient who, although living with serious illness, is functioning at baseline.
Finally, the study was conducted at a time when the Serious Illness Care Program was within the first two years of implementation with varied practices by different clinicians at the participating sites. Thus, the patients' experiences presented in this study likely do not reflect the full impact of iterative, orchestrated conversations conducted over time. Future work should explore the experience of having multiple conversations.
Conclusion
Patients reported positive experiences with serious illness conversations in primary care. They appreciated well-planned, personalized conversations, facilitated by established relationships with primary care clinicians who are skilled communicators. Future efforts can be focused on improving clinicians' skills of navigating emotional challenges during these conversations and implementing system changes to optimize orchestration of conversations, ideally with dedicated visit time set aside and with improved access for diverse populations.
Footnotes
Authors' Contributions
L.X., R.K.S., L.N., C.M., L.T., and J.J. contributed substantially to the study design and drafting/revision of the article. L.X. and J.J. completed data acquisition, analysis, and interpretation. All authors approved the final version of the article.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.