
Abstract
Background:
People with life-limiting illnesses experience a range of distressing symptoms. Appetite-related symptoms are common, but studies have found varied prevalence and the distress caused has had limited quantification.
Objectives:
To examine the clinicodemographic factors and trajectory of appetite-related distress in the last 60 days of life.
Design/Setting/Subjects:
Consecutive cohort of 109,385 patients (359,038 data points) using specialist palliative care services in the Australian Palliative Care Outcomes Collaboration (PCOC).
Measurements:
Patient-reported appetite-related distress using the PCOC Symptom Assessment Scale.
Results:
Diagnoses included cancer (75%), end-stage organ failure (11%), neurodegenerative disease (4%), dementia (3%), and other noncancer (7%). Fifty-eight percent reported some degree of appetite-related distress at least once in the last 60 days of life. Daily mean distress scores did not vary greatly by diagnosis and the distributions of symptom severity were not linked with performance status. There was a sharp decline in mean distress for all diagnostic groups around 7–10 days before death. Moderate to severe distress was associated with nausea-, bowel-, pain-, and breathing-related distress, controlling for key baseline factors.
Conclusion:
Appetite-related distress is prevalent and burdensome in the 60 days before death and is strongly associated with distress from other cardinal symptoms.
Introduction
People with life-limiting illnesses often experience multiple distressing symptoms that reduce quality of life1–3 and directly impact on patients' clinical outcomes. 4 Loss of appetite (anorexia), early satiety, food aversions, changed tastes, and reduced food intake impact many people with palliative needs and their caregivers.5–7 Food intake carries significant emotional, social, and cultural meaning for most patients and families.8,9 In particular, weight loss, which is often a combination of reduced oral intake and cachexia, has been linked to patient and family anxiety, 10 serving as a constant reminder of illness. 11
Although most research focus on people with cancer, those with end-stage organ failure, neurodegenerative disease, or HIV/AIDS often experience anorexia. 12 Prevalence estimates vary by diagnosis: HIV (24% 12 to 46% 13 ), chronic heart failure (38%), 14 and advanced cancer (up to 80%). 15 Although prevalent, distress caused by anorexia is poorly quantified. 9
Anorexia may be caused by the life-limiting illness or coexisting symptoms including depression, pain, fatigue, nausea, vomiting, constipation, or breathlessness.15–17 Controlling other symptoms may improve appetite for some. 18 Anorexia is associated with mortality, thus potentially informing prognosis. 19
Little is known about the patterns of self-reported distress caused by appetite in different disease groups, with most data from hospitalized patients. 20 To address this, the primary aim of this study was to describe clinicodemographic factors, frequency, intensity, and temporal patterns of appetite-related distress in the last 60 days of life in a palliative population. The secondary aim was to determine whether primary diagnosis or setting of care predicted those at risk of appetite-related distress.
Materials and Methods
Study design and population
This longitudinal consecutive cohort study of prospectively collected point-of-care patient data from the Australian national Palliative Care Outcomes Collaboration (PCOC) used data from palliative care services that voluntarily provided data on all patients at agreed time points using standardized validated clinical assessment tools. 21 Deidentified data from 203 services on all patients aged ≥18 years who died between January 1, 2013, and December 31, 2018, with ≥1 measurement of appetite-related distress in the 60 days before death were included.
Data collection
Patient-level data included demographic characteristics and primary diagnosis collected on referral. Patient-level data were collected at each change in inpatient or community care setting (episode) and with changes in clinical phase (stable, unstable, deteriorating, or terminal) with each episode. 22
Symptom-related distress was measured by the validated PCOC Symptom Assessment Scale (SAS)23,24 This instrument was designed to be used as a patient-rated (or proxy-rated) assessment tool on the degree of each person's perceived distress regarding pain, appetite problems, nausea, bowel problems, breathing problems, insomnia, and fatigue using a numerical rating scale from 0 (no distress) to 10 (worst possible distress). Appetite-related distress was reported using the PCOC SAS23,24 and scores were grouped into absent (0), mild (1 − 3), moderate (4 − 7), and severe (8 − 10). 23 The definition of symptom distress used for PCOC SAS is “the degree of discomfort from the specific symptom as reported by the patient.”25,26 Function was clinician assessed using the ordinal Australia-modified Karnofsky Performance Scale (AKPS) 27 where lower scores reflect poorer function (100–0 in 10-point decrements).
Statistical analysis
Patients are presented in five diagnostic groups. The primary outcome was patient-reported appetite-related distress. The incidence of moderate or severe appetite-related distress by care setting, patient characteristics, diagnostic group, and other symptoms are presented.
The number of available assessments by days until death, locally weighted smoothing (LOESS)-smoothed curves of daily mean appetite-related distress over days until death, and the distribution of appetite-related distress by AKPS were calculated.
Odds ratios from logistic regressions for hospital and community were calculated for associations between appetite-related distress (severe-moderate vs. mild-absent) and distress related to nausea, bowels, pain, and breathlessness. These were adjusted for gender, age group at death, days until death, and AKPS. Confidence intervals were estimated using a patient-clustered variance sandwich estimator, adjusting for multiple assessments per patient. Analyses were undertaken using SAS® v9.4M5 and R v3.6.2.
Ethical considerations
PCOC has approval from the human research ethics committee of the University of Wollongong (approval ID: HE2006/045). These were deidentified aggregated clinical data negating need for individual consent.
Results
A total of 116,340 patients died in the study period of whom 109,385 provided ≥1 measure of appetite-related distress (359,038 data points). Most patients received care only in hospital (62.6%), whereas 11.2% of patients had both hospital and community episodes. Sixty-two percent of the 3195 patients with dementia were in community care. The number of clinical assessments increased as death approached (Fig. 1), reflecting referral patterns and changing clinical status.
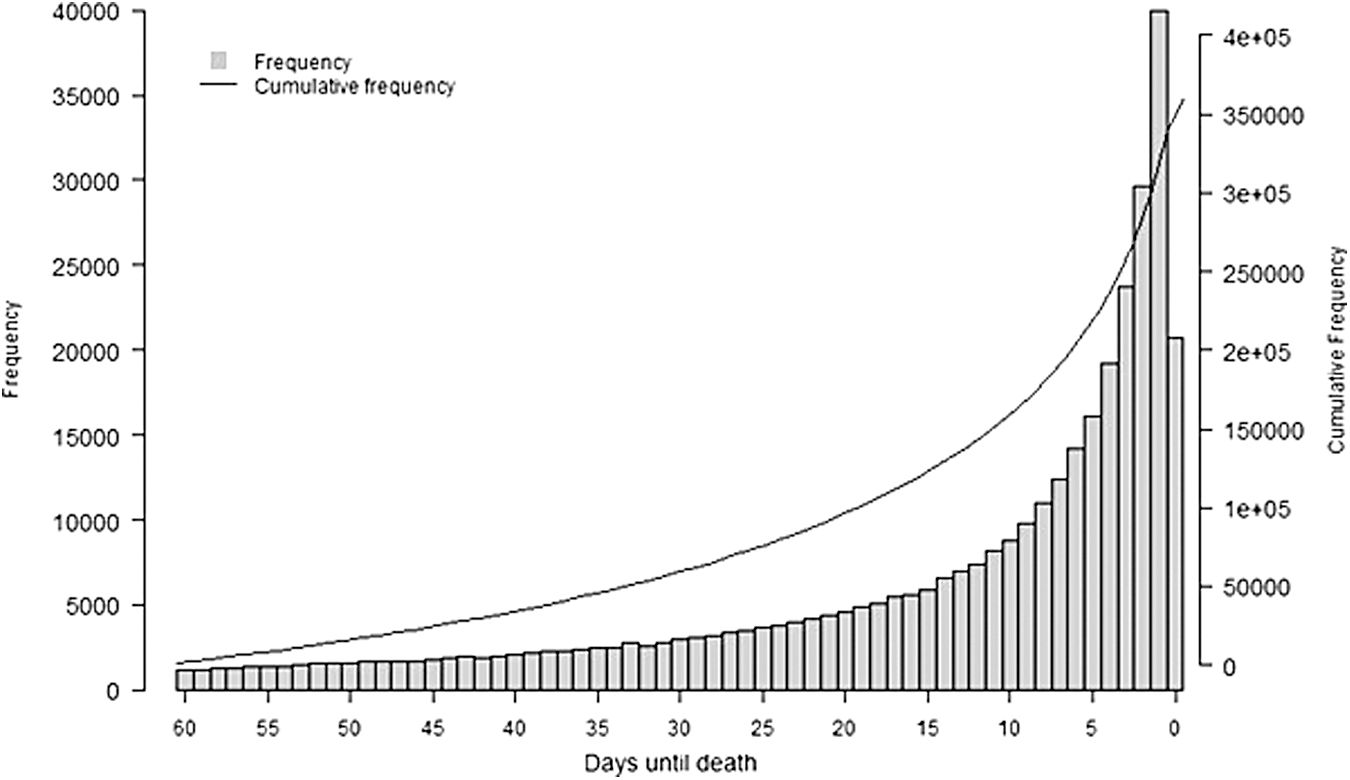
Daily and cumulative frequency of assessments in the last 60 days of life of distress related to appetite in a national cohort of people receiving palliative care (n = 109,385 patients, 359,038 data points).
More patients were male (53.8%), Australian born (64.2%), and English speaking (69.6%). In five diagnostic cohorts [cancer (75%), end-stage organ failure (11%), neurodegenerative diseases (4%), dementia (3%), and other noncancer diagnoses (7%)], age at death differed [the youngest—cancer (μ = 72.0 ± 13.1); the oldest—dementia (μ = 85.4 ± 8.6)] (Table 1). Overall, 57.9% of patients reported ≥1 appetite-related distress, more often in people with cancer (average of 1.5 reports per patient), and less often in neurodegenerative diseases or dementia.
Patient Characteristics of the Five Diagnostic Cohorts of People in the Last 60 Days of Life from a Consecutive National Cohort of People Referred to Participating Palliative Care Services
n = 109,385 patients, 359,038 data points.
LOESS-smoothed curves for daily mean appetite-related distress reflected little difference between diagnostic groups with a sharp decline in scores 7–10 days before death (Fig. 2). People with neurodegenerative disease or dementia reported lower levels of appetite distress from 15 to 30 days before death. When explored by function, severity of distress was stable until an AKPS of 20–10 (Fig. 3). Higher percentage of patients reported moderate or severe distress in the community (22.7%) than in the hospital setting (17.8%). Nausea- and bowel-related distress were more likely in people with appetite-related distress (Table 2).

Mean level of PCOC SAS appetite-related distress as death approaches, by diagnostic cohort in a national consecutive cohort of people referred to participating palliative care services. (n = 109,385 patients, 359,038 data-points). PCOC, Palliative Care Outcomes Collaboration; SAS, Symptom Assessment Scale.
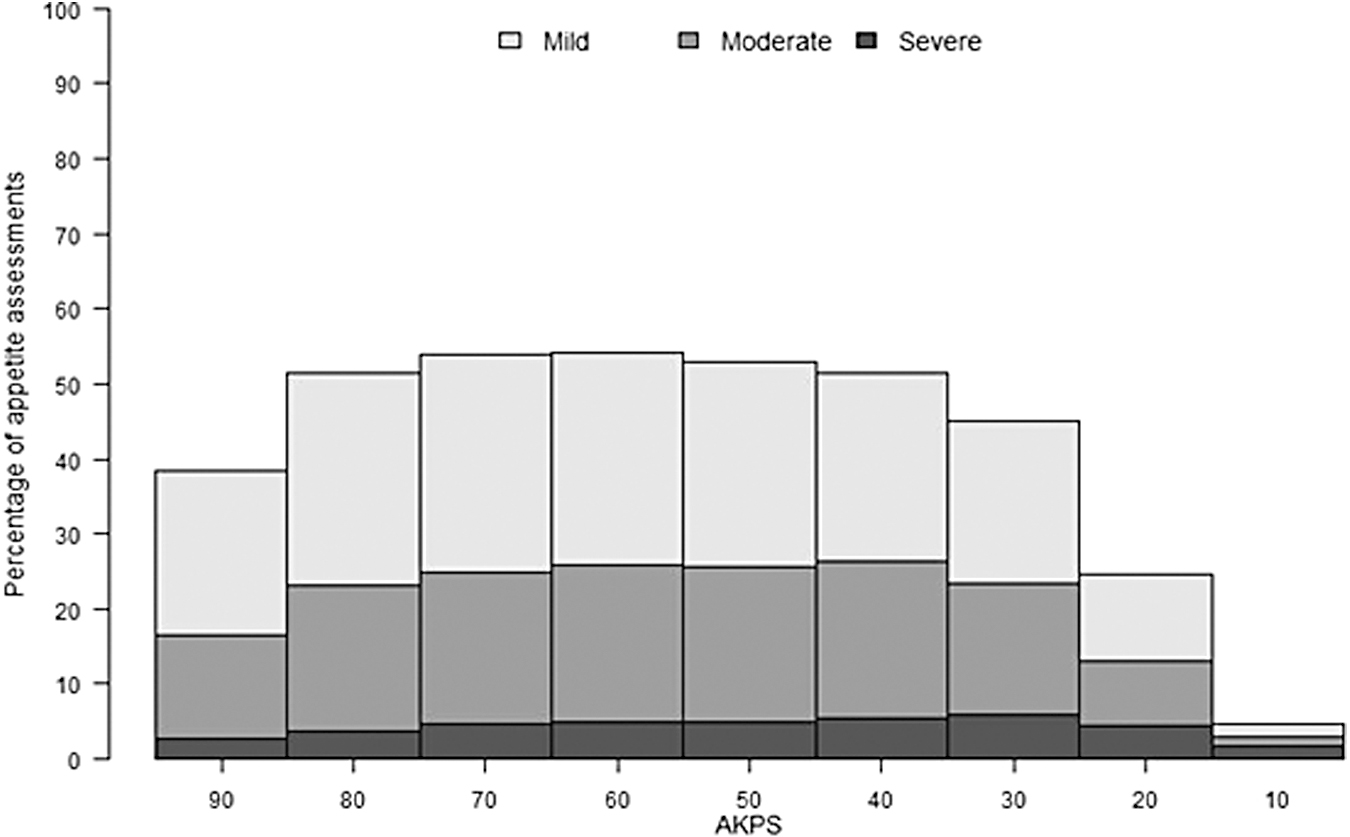
PCOC SAS appetite-related distress categories by AKPS in a national consecutive cohort of people referred to participating palliative care services. (n = 109,385 patients, 359,038 data points). AKPS, Australia-modified Karnofsky Performance Status.
Clinicodemographic Data for the Palliative Care Assessments by Care Setting (Hospital or Community) in a National Consecutive Cohort of People Referred to Participating Palliative Care Services
n = 109,385 patients, 359,038 data points.
AKPS, Australia-modified Karnofsky Performance Status; SAS, Symptom Assessment Scale.
Using logistic regression, conditional odds ratios of appetite-related distress for other symptoms were generated (Table 3). In hospital and community settings, moderate to severe appetite-related distress was associated with the presence of nausea-, bowel-, pain-, and breathing-related distress.
Adjusted Odds Ratios and 95% Confidence Intervals for Moderate/Severe Appetite-Related Distress for Levels of Other Symptom-Related Distress, by Setting of Care, Palliative Care Outcomes Collaboration Data, Deceased 2013–2018
All models include age at death, gender, days until death, and AKPS as covariates. Confidence intervals based on a patient-clustered variance sandwich estimator. Hospital and community models estimated separately.
Discussion
This very large consecutive cohort that includes people with nonmalignant diagnoses demonstrates mild to moderate appetite-related distress for most palliative care patients across five diagnostic groups, with distress diminishing in the last weeks of life. This study also shows a strong relationship between appetite-related distress and nausea- and bowel-related distress, reflecting also that patients with life-limiting illnesses are likely to more than one symptom at any one time, at times clustered together. 28
Findings are consistent with people who have advanced cancer attending a palliative care clinic 20 or admitted to hospital. 29 Kutner et al. in a cross-sectional study in people with life-limiting illnesses reported that although some degree of lack of appetite was among the most common symptom reported, patients seemed less affected by these symptoms, with distress scores varying from mostly mild to moderate. 30 People with neurodegenerative diseases or dementia had lower levels of distress overall and a decline in mean scores earlier than seven days before death, reflecting literature on people with dementia in the seven days before death, 31 although the ability to report distress may also be impaired late in life. 32
Appetite-related distress was reported more often in community settings but this may be an artifact of more hospital assessments occurring closer to death when appetite-related distress diminished. The regression model suggests that the difference between hospital and community in odds ratios is minimal once it is adjusted for other variables, therefore, not significant. Difference in symptom frequency and severity between community and hospital care may be due to inherent variations among patients, care settings, and manifestations of disease. 30
Strengths
Data from this study represent a very large and heterogeneous sample of palliative care patients with varying diagnoses across a broad geography, and in differing care settings using prospectively collected data using validated tools.23,24,27
Limitations
The study only reports on people referred to palliative care services, and in a high-income country. How these results can be interpreted in the proportion of people not referred nor in low- and middle-income countries is not immediately clear. The proportion of proxy reporting was also not available from the data set, although proxy rating may be acceptable. 24 As an observational study, no causal relationship can be inferred from the results. No data were available on the clinical response to appetite-related distress.
What this study adds
This study highlights that there needs to be frequent review of appetite-related distress in the last 2 months of life, however, distress may diminish in the last 7–10 days. Better understanding of appetite-related distress from the time of diagnosis may contribute to improved care planning for all palliative care patients, including those with diagnoses other than cancer.
Conclusions
In our cohort, mild to severe appetite-related distress was reported in over half of the assessments in patients with life-limiting illnesses in the 60 days before death. This finding is particularly important for people with noncancer diagnoses. Earlier interventions targeting other related symptoms (particularly, nausea and bowel-related distress) for more functional patients should also be explored to investigate whether appetite-related distress can be reduced more systematically.
Author's Contributions
M.S.S., W.D., M.B., V.R.-N., M.A., B.D., and D.C.C. made a substantial contribution to the concept or design of the study; or acquisition, analysis, or interpretation of data. M.S.S., W.D., M.B., V.R.-N., M.A., B.D., and D.C.C. drafted the article or revised it critically for important intellectual content. M.S.S., W.D., M.B., V.R.-N., M.A., B.D., and D.C.C. approved the version to be published. M.S.S., W.D., M.B., V.R.-N., M.A., B.D., and D.C.C. have participated sufficiently in the study to take public responsibility for appropriate portions of the content.
Footnotes
Acknowledgments
The authors thank the patients who provided symptom data throughout their contact with services and the participating services.
Conference Abstract presented as poster at the (Virtual) 5th Cancer Cachexia Society Meeting, September 10–11, 2020 (online); Montreal, Canada.
Data Management and Sharing
All data are available to bona fide researchers through the Australian national PCOC through their standard operating procedure for data access.
Funding Information
The Australian national PCOC is funded by the Palliative Care Section of the Commonwealth Department of Health and Ageing.
Author Disclosure Statement
The authors declare that they have no conflict of interest.