
Abstract
Cutaneous T cell lymphomas are associated with distressing symptoms, including pain and pruritus that negatively impact quality of life. Early involvement of palliative care can provide relief of symptoms and address multifaceted distress. This case highlights the complex management of cutaneous T cell lymphoma pain and associated symptoms, including existential and psychosocial distress. Our patient required frequent titration and rotation of high-dose opioids and adjuvant analgesics, ultimately requiring transfer to the intensive care unit for analgosedation. Total skin loss and disease complications led to his death after a compassionate withdrawal of life support. Cutaneous T cell lymphoma pain can be successfully managed with an interdisciplinary approach, early palliative care, and aggressive pain management. Complications from advanced disease, superinfection, and multidimensional distress complicate the efficacy of a multimodal analgesic approach. Further research is needed to deepen our understanding of how to optimally alleviate suffering within this vulnerable population.
Introduction
Cutaneous T cell lymphomas (CTCLs) are a type of non-Hodgkin's lymphoma in which monoclonal T lymphocytes infiltrate the skin. 1 CTCL is characterized by skin erythema, patches, plaques, or tumors. 2 Mycosis fungoides (MF) is the most prevalent subtype, followed by Sezary syndrome, which has a shorter prognosis. 2 CTCL is associated with a high symptom burden due to the disease itself and from disease-targeted treatments. Pain is a very common symptom, arising from skin lesions and is associated with debilitating pruritus that interrupts sleep and significantly impacts quality of life. 3 Palliative care consultation services are asked to provide pain and symptom management associated with CTCL, while balancing treatment goals and patient values. We describe the following case to illustrate the multitude of challenges in managing CTCL pain, including a review of the pathophysiology of CTCL pain and pharmacological drug selection for refractory pain.
Case Description
A 67-year-old male with a history of Crohn's colitis, psoriasis, and CTCL/MF presented for an initial consultation to the Supportive Care Service at Memorial Sloan Kettering Cancer Center for a symptom management evaluation a few months after his MF diagnosis. He had received multiple lines of cancer treatment, including brentuximab, total skin electron beam radiation, mogamulizumab, and cyclophosphamide and etoposide, before this appointment, and there was a possibility of undergoing a bone marrow transplant with the goal of a potential cure.
Outpatient pain management
Due to the coronavirus 2019 (COVID-19) pandemic, the patient's initial Supportive Care visit was conducted using telehealth. He endorsed excruciating “burning” pain to his extremities and torso, with somatic and neuropathic characteristics (including allodynia), 10/10 intensity, aggravated with palpation and dressing changes. He was taking oxycodone and gabapentin, prescribed by his oncologist, with suboptimal relief. The MF wounds required slow and painful dressing changes, up to three hours daily, conducted by his wife. His goal was to achieve pain relief using minimal opioids, if possible, as he greatly valued his independence.
His outpatient Supportive Care provider prescribed morphine extended release, along with increased doses of oxycodone and gabapentin (Table 1). He experienced dose-limiting side effects (e.g., confusion, hallucinations) with morphine. He subsequently developed worsening erythroderma, plaques and dryness on his face, trunk and extremities, along with new weeping areas in the antecubital fossa, lymphedema, and desquamation of his skin surface; these skin changes caused significant worsening of his pain. His symptom management in the outpatient setting was challenged by the limitations of using telehealth, which made it difficult to visualize his skin and wounds directly. Dose-limiting opioid side effects, especially sedation and confusion, continued to complicate his pain management (Table 1).
Summary of Analgesics Used during Outpatient Management
q, every; h, hour.
ER, extended release; PRN, as needed.
Inpatient pain management
Although the patient hoped to avoid hospitalization, he was eventually admitted for pain crisis. He required hydromorphone intravenous (IV) patient-controlled analgesia (PCA) and IV ketamine infusion, which was limited by psychomimetic side effects (i.e., hallucinations), hypertension, and tachycardia. His skin condition progressed with more severe ulcerations and desquamation resulting in excruciating pain, which he described as “sitting on broken glass.”
The widespread nature of his skin lesions precluded many pain management options. For example, there was no single identifiable location for placement of a transdermal fentanyl patch. Topical analgesics were not feasible given his diffuse total body skin loss. He was not a candidate for a home PCA infusion due to the increased risk of infection with insertion of a central access catheter (which would be required to receive the home PCA infusion), nor was he a candidate for procedural-based interventions (e.g., local nerve block), due to the diffuse distribution of his pain. These challenges were exacerbated by the patient's nonadherence and frequent self-titration of analgesic medications without notifying his Supportive Care team. He was ultimately transitioned to methadone successfully (Table 1), yet continued to experience debilitating pain.
He was rehospitalized approximately one month after his initial admission. During this second admission, Dermatology determined his condition was most consistent with a grade 4 lichenoid drug eruption due to mogamulizumab, with bacterial superinfection. He was treated with systemic steroids and broad-spectrum antimicrobials. The inpatient Supportive Care team guided his analgesic regimen (Table 2). Throughout this admission, the patient and his wife requested that he be “knocked out” for dressing changes, which consistently caused him to cry out and tremble for an hour afterward. He was ultimately transferred to the intensive care unit (ICU) to safely utilize pharmacologic interventions for palliative sedation to optimize his pain management during his dressing changes and requisite nursing care.
Summary of Analgesics Used during the Terminal Inpatient Admission
q, every; h, hour.
CPOT, Critical Care Pain Observation Tool; HD, hospital day; IV, intravenous; PCA, patient-controlled analgesia; PO, by mouth; PRN, as needed.
ICU pain management
His ICU course was complicated by acute kidney injury and dose-limiting sedation, causing him to lose the capacity to use the demand dose of his PCA appropriately. He was subsequently transitioned to a methadone IV PCA, with an hourly basal rate and clinician boluses only (Table 2). Despite these interventions, his pain was only tolerable when he was lying still, fully immobile, and not being touched. The intense distress associated with bearing witness to this pain was felt by the full interdisciplinary team, especially the bedside nurses who performed his wound care. Following multiple family meetings with the interdisciplinary Lymphoma, Nursing, Supportive Care, Dermatology, Infectious Disease, ICU, and Ethics teams, he was ultimately intubated for airway protection and maximal analgosedation (Table 2). The Ethics team played a key role in facilitating the process of shared decision making, highlighting the providers' responsibility to prevent and alleviate suffering while empowering the patient and family to decide what level of sedation was acceptable based on their core values.
Pain management at the end of life
The patient's clinical course in the ICU was complicated by progressive electrolyte derangements, pancytopenia, metabolic acidosis, sepsis, and hypothermia in the setting of extensive skin loss. Although his nonverbal pain scores improved (Table 2), the interdisciplinary team members worried that his prolonged (and uncertain) wound healing timeline would likely preclude receipt of further lymphoma-directed treatment. After his condition remained unchanged despite a time-limited trial of life-sustaining treatments, his wife elected to allow a natural death, as she recognized that his quality of life was no longer acceptable to him. In the last week of his life, his comfort was maintained using IV fentanyl, methadone, lorazepam, propofol, and ketamine (Table 2). He died peacefully after a compassionate withdrawal from the ventilator, surrounded by loved ones.
Discussion
Palliative care is frequently consulted to assist with symptom management at all stages of illness. For patients with CTCL, pain is a common reason for palliative care consultation, as it is present in 41% of people with the diagnosis, and is more likely to be reported in advanced disease or during dressing changes.4–6 While other case reports have been published on the management of CTCL 7 and mogamulizumab-induced mucocutaneous lichenoid reaction, 8 none has primarily focused on the complicated management of CTCL pain. This case report exemplifies the devastating effects of pain related to CTCL and the myriad challenges in managing such pain.
Pathophysiology of CTCL pain
Although pain has been shown to contribute to poor quality of life for patients with CTCL,3,5 the pathophysiology of CTCL pain is not well understood (Table 3). The primary etiology of CTCL pain is from the lesions associated with the disease, including skin breakdown in the form of fissures, lacerations, sores, or complications such as skin infections. 3 CTCL pain is commonly associated with diffuse pruritus and can present similarly to neuropathic pain.3,9 Other case reports have described this relationship between pain and pruritus. 10 Patient descriptions of pain support the notion that CTCL pain is mostly neuropathic, with some nociceptive qualities. As in our case report, CTCL pain is commonly described as “burning,” “needles sticking your body,” “sharp,” or “stabbing.” 3 While further research is needed to establish the relationship between CTCL pain and pruritus, a recent study shows the role of transient receptor potential ankyrin 1 (TRPA1), a member of transient receptor potential (TRP) channels, in helping mediate pain and pruritus related to chronic inflammatory skin conditions and cancers, such as CTCL. 11
Pathophysiology of Our Patient's Cutaneous T Cell Lymphoma Pain
CTCL, cutaneous T cell lymphoma.
Pharmacologic management of CTCL pain
The approach to management of CTLC pain in this case followed standard cancer pain management guidelines. 12 Use of opioid analgesics and adjuvants were optimized as these are commonly used to manage cancer-related pain and are required for analgesia in 43% of cancer patients. 13 As pain progressed in the setting of severe cutaneous disease and treatment-related effects, more aggressive approaches were required. Opioids were rotated due to dose-limiting adverse effects; methadone was selected based on its beneficial role in managing neuropathic pain, as an N-methyl-D-aspartate receptor antagonist. 14 Anticonvulsants (e.g., gabapentin, pregabalin) were added for their beneficial analgesic and antipruritic effects, in addition to their effective use in malignant wound care. 15
Ketamine, which has been used successfully to manage refractory cancer-related pain, 16 and as an analgesic and sedative option for burn wound care, 17 was also used. Additional multimodal adjuvants (e.g., duloxetine, acetaminophen, ketorolac, steroids) were incorporated to address ongoing neuropathic and inflammatory pain components. However, this patient suffered multiple disease complications (e.g., infection, severe electrolyte derangements) that substantially impeded his analgesic response.
Additional considerations in refractory CTCL pain
Given the dearth of literature on CTCL pain, alternative approaches were required to achieve analgesia, especially during dressing changes. After the optimization of standard analgesics, dexmedetomidine was used for intractable pain and potential opioid-induced hyperalgesia. 18 Subsequently, additional sedation was required for wound care, for which propofol was used in combination with lorazepam. While subhypnotic doses of propofol have been used for pruritus associated with liver disease, 19 opioid-induced pruritus, 20 or for refractory pain during palliative procedures, 21 its use in this case was primarily for palliative sedation. In our setting, use of these sedating agents (e.g., dexmedetomidine, propofol) required the patient to be transferred to the ICU and are typically considered to be an option of “last resort.” Other drugs, such as midazolam, phenobarbital, or promethazine (in addition to or without propofol), could have been used for palliative sedation but were not needed in this case. 22 Another option, not utilized in this case, is IV lidocaine, which has been used for intractable cancer-related pain and wound care, 23 and refractory CTCL pruritus 10 in the hospice and palliative care setting.
Total CTCL pain
We share this case to help consolidate knowledge and awareness of varied clinical approaches to managing pain in patients with advanced CTCL. It is important to note that our patient's pain was exacerbated by existential distress, concerns about his mortality, and progressive loss of independence. Total pain, a term coined by Dame Cicely Saunders, describes this type of multidimensional suffering associated with pain, including physical, psychological, social, and spiritual contributing factors. 24 The patient's request to be “knocked out” serves as an indicator of the extreme extent of total pain he was experiencing (Fig. 1). CTCL pain is often associated with insomnia, anxiety, and depression. 2
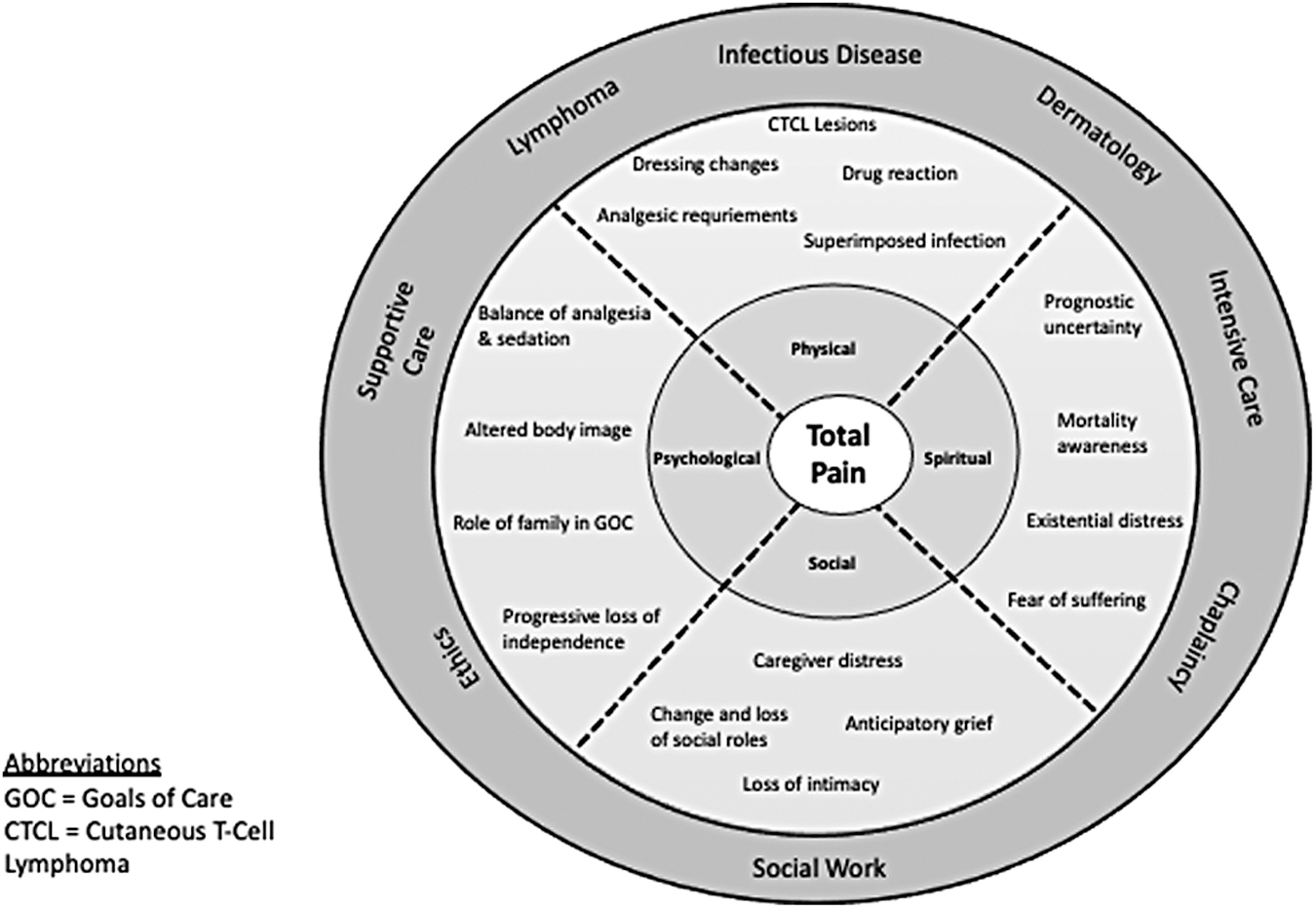
Total pain experienced with cutaneous T cell lymphoma.
In addition, the visual experience of CTCL causes a profound psychological impact, interfering with socialization and intimacy. 6 This case underscores the importance of eliciting and honoring the patient's wishes with respect to balancing analgesia with sedation, and thereby restoring some agency and empowering the patient in a situation in which so much is beyond the patient's control. It was critical to work closely with the interdisciplinary team to provide optimal analgesia and effectively address the multiple contributors to this patient's intense pain and distress.
Conclusion
This case occurred within a highly specialized tertiary cancer center, with access to a robust interdisciplinary Supportive Care service providing symptom management expertise and extensive psychosocial and existential support for the patient and family, 24 hours per day and 7 days per week. The experience of the patient, his family, and the health care team may have been quite different in another care setting, with more limited access to team resources and available personnel. Nonetheless, the immensity of this patient's suffering and the multidimensional aspects of his pain syndrome necessitating a complex, multimodal analgesic approach are relevant for the management of not only CTCL patients, but also patients with other debilitating chronic skin diseases. Further research is needed to deepen our understanding of CTCL pain and how to optimally care for and alleviate suffering within these vulnerable patient populations.
Footnotes
Funding Information
This research is funded in part through the NIH/NCI Cancer Center Support Grant P30 CA008748. A.V.D. is supported by a Career Development Award from the National Palliative Care Research Center (Kornfeld Scholars Program) and was the Frances Young Tang Research Fellow in Palliative Medicine at the Memorial Sloan Kettering Cancer Center from 2016 to 2017.
Author Disclosure Statement
No competing financial interests exist.