
Abstract
Background:
In spring 2020, the COVID-19 pandemic overwhelmed intensive care teams with severely ill patients. Even at the end of life, families were barred from hospitals, relying solely on remote communication. A Remote Communication Liaison Program (RCLP) was established to ensure daily communication for families, while supporting overstretched intensivists.
Objectives:
To evaluate the effectiveness and impact of the RCLP on participating liaisons and intensivists.
Design:
Two quality improvement surveys were developed and administered electronically.
Setting/Subjects:
Based in the United States, all liaisons and intensivists who participated in this program were invited to take the surveys.
Measurements:
Descriptive statistics were used to analyze the quantitative Likert-scale data, and qualitative analysis was used to assess themes.
Results:
Among respondents, all (100%) liaisons and more than 90% of intensivists agreed or strongly agreed that the RCLP provided a valuable service to families. More than 70% of intensivists agreed or strongly agreed that the program lessened their workload. More than 90% of liaisons agreed or strongly agreed that participation in the program improved their confidence and skills in end-of-life decision making, difficult conversations, and comprehension of critical care charts. Themes elicited from the liaisons revealed that participation fostered a renewed sense of purpose as physicians, meaningful connection, and opportunities for growth.
Conclusions:
RCLP successfully trained and deployed liaisons to rapidly develop skills in communication with beleaguered families during COVID-19 surge. Participation in the program had a profound effect on liaisons, who experienced a renewed sense of meaning and connection to the practice of medicine.
Introduction
In spring 2020, as COVID-19 surged in the northeastern United States, intensive care unit (ICU) teams were overwhelmed with critically ill patients, resulting in extended clinical duties and limited time for non-acute medical management. To protect families from illness, hospital visitation policies barred families from the bedside, even when patients were critically ill and dying.1,2,25 The elimination of in-person interactions with health care teams left families desperate for information on their loved ones' status. Infrequent discussions via telephone with overburdened ICU personnel often did little to compensate for the loss of in-person interactions.2,3
COVID-19 caused new hardships for patients and families and unprecedented burdens for health care workers. 29 Health care workers endured long duty hours, sleep disruptions, and concerns for personal and family safety.5–7 As early as March 2020, the World Health Organization warned about the pandemic's potential psychological stress and negative impact on health care workers. 4 The serious mental health effects for health care workers are as follows: heightened burnout, post-traumatic stress disorder, anxiety, and depression.5–10
During and after the initial COVID-19 surge, health care organizations attempted to address burnout via strategies, including peer support, 11 counseling, 12 and debriefing. 13 Providing meaningful family-centered care or contributing to “a good death” was found to mitigate clinician post-traumatic stress disorder and burnout,1,14,15 but there is little evidence supporting specific interventions to facilitate family-centered care.
To address the challenges faced by families of critically ill patients and ICU providers, our hospital established a Remote Communication Liaison Program (RCLP). Liaisons functioned like family navigators (FN) to provide consistent clinical updates, emotional support, and primary palliative care services to families who could not be present in-person and to offset work for the ICU staff and palliative care team who were working at three times pre-pandemic capacity. Typically, FNs have extensive ICU experience. Liaisons were from varied non-ICU backgrounds, eager to help, but with limited ICU experience. Due to lack of experience or need to mitigate personal risk, they were unable to volunteer in-person.
What is unique about this program is that despite limited ICU experience liaisons were able to fulfill similar roles. Liaisons were rapidly identified, expediently trained utilizing real-time resources and peer-to-peer expertise, and deployed <1 week after identifying a communication gap. A unique aspect of this program is a focus on continuous peer learning, including real-time crowd-sourced resource development of innovations such as a live wiki-page for individuals to share experiences in a centralized and easy to access document. Additionally, peer-to-peer coaching teams worked as evolving educational groups of two to three liaisons on ICU pods to help navigate challenges such as difficult family conversations, uncertainty of prognosis, and end-of-life issues. For additional information on design and setup, refer to the study by Lipworth et al. 16
We hypothesized that liaisons would serve as effective FNs to provide communication and emotional support to patients' families during the first COVID surge. The objectives of this article were to evaluate the impact of this adaptive strategy on participant clinicians and to determine if the program met its mission to decrease ICU workload.
Methods
We surveyed intensivist and liaisons who were deployed in a suburban academic medical center during the first New England COVID-19 surge. Two post-program quality improvement surveys, each for the liaisons and intensivists, were developed (Supplementary Tables S1 and S2), including Likert-scale questions for quantitative analysis and open-ended questions for qualitative analysis. The surveys assessed the (1) program's perceived impact on families, (2) effectiveness of the training program and coaching supports provided to liaisons, (3) effectiveness of program in supporting ICU providers, and (4) professional impact of participation on the liaisons and intensivists.
Questions regarding participant's likelihood of recommending the program were scored 0–10 and used to generate an overall measure of participant experience, analogous to the validated Net Promotor Score® (NPS®) measure of customer experience. 30 Electronic surveys were administered via Google Forms between June 23 and July 27, 2020. Participation was voluntary, anonymous, and without incentives. After the initial invitation, two additional reminder e-mails requesting participation were sent. Quantitative analyses were completed using commercially available statistical software with Fisher's exact test.
The free-text responses to open-ended questions were reported based on Standards for Reporting Qualitative Research reporting guidelines. 17 Qualitative analyses were completed with investigators from our research team (M.H., N.M., and A.D.L.). These individuals reviewed responses independently, developed coding schemes, grouped codes, and identified overarching themes for each survey using in vivo, open, and axial coding maintained in files behind the protected hospital firewall. The coders met to reconcile similar codes into a common codebook and to discuss emergent categories and themes.
Coding categories were linked to prevalence determined by content analysis to identify emerging patterns. Thematic analysis was used to group codes and patterns. Group consensus was used to merge into higher level themes and to resolve discrepancies. This process was repeated until coders reached consensus. Codes and themes were subsequently reviewed with all authors for final consensus. This quality improvement project was deemed exempt by the Lahey Hospital and Medical Center Institutional Review Board.
Results
Quantitative results
Fifty-six out of 62 (90.3%) eligible communication liaison providers and 18 out of 34 (52.9%) intensivists completed the survey. Three liaison-volunteers were not invited to take the survey: two participated (as coaches) during the four-day pilot phase only, 16 and the third helped to administer the program and developed these surveys. Liaisons were physicians, advanced practice providers, and psychologists representing 19 specialty divisions (Table 1). Intensivists were attending physicians from pulmonology, surgery, anesthesia, and neurocritical care.
Specialty Breakdown for Liaison Participants Eligible for the Survey
Medicine: Allergy, Cardiology, Endocrinology, Gastroenterology, Hematology-Oncology, Primary Care.
Other: Neurology, Pathology, Radiation Oncology.
Surgery: Bariatric, Breast, Colon and Rectal, General, Gynecology, Ophthalmology.
More than 94% of responding liaisons agreed or strongly agreed that the RCLP prepared and supported the liaisons during the program. More than 90% of liaisons indicated agreement or strong agreement with confidence in their post-program ability to (1) rapidly comprehend a critical care chart, (2) discuss end-of-life-care planning, and (3) engage in highly emotional conversations with patients' families. These results (Fig. 1) represented a significant increase compared with liaisons' self-reported baseline ability: ICU chart comprehension (strongly agree 58.9% vs. 14.3% p < 0.001), end-of-life-care planning (strongly agree 50% vs. 25% p = 0.01), and ability to engage in emotional conversations (strongly agree 57.1% vs. 32.1% p = 0.01). Liaisons overwhelmingly reported their interactions with families (98.2%), critical care colleagues (96.4%), and other liaisons (100%) to be rewarding (Fig. 2). Additionally, 98.2% of liaisons strongly agreed that the program provided a valuable service to families.
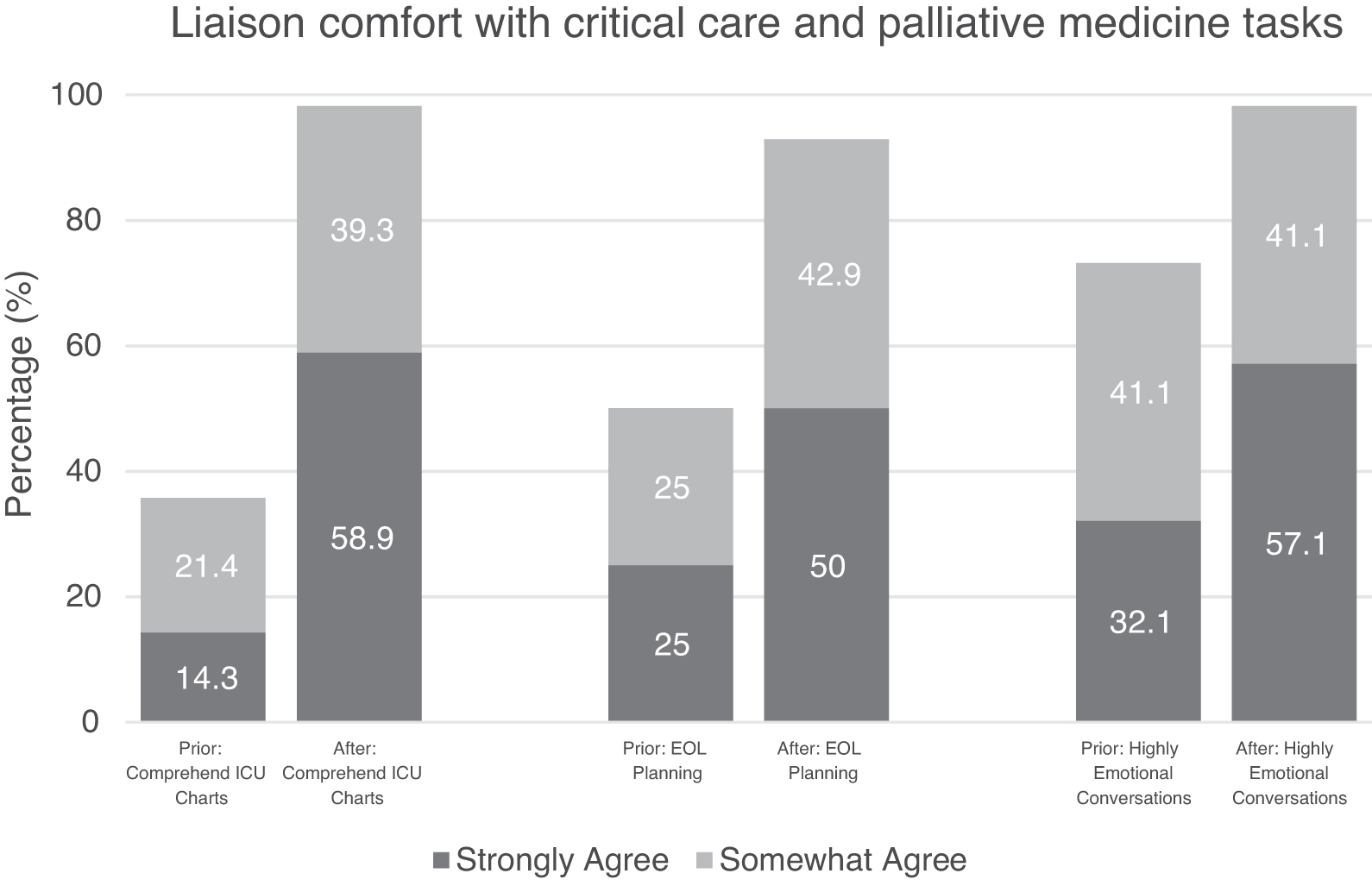
The proportion of liaison providers who agreed or strongly agreed with assertions of confidence in their ability before and after the program to (1) “rapidly review and comprehend a critical care chart,” (2) “discuss end of life care planning with patients and families,” and (3) “handle highly emotional conversations with patients and families” (p < 0.005). EOL, end of life; ICU, intensive care unit.
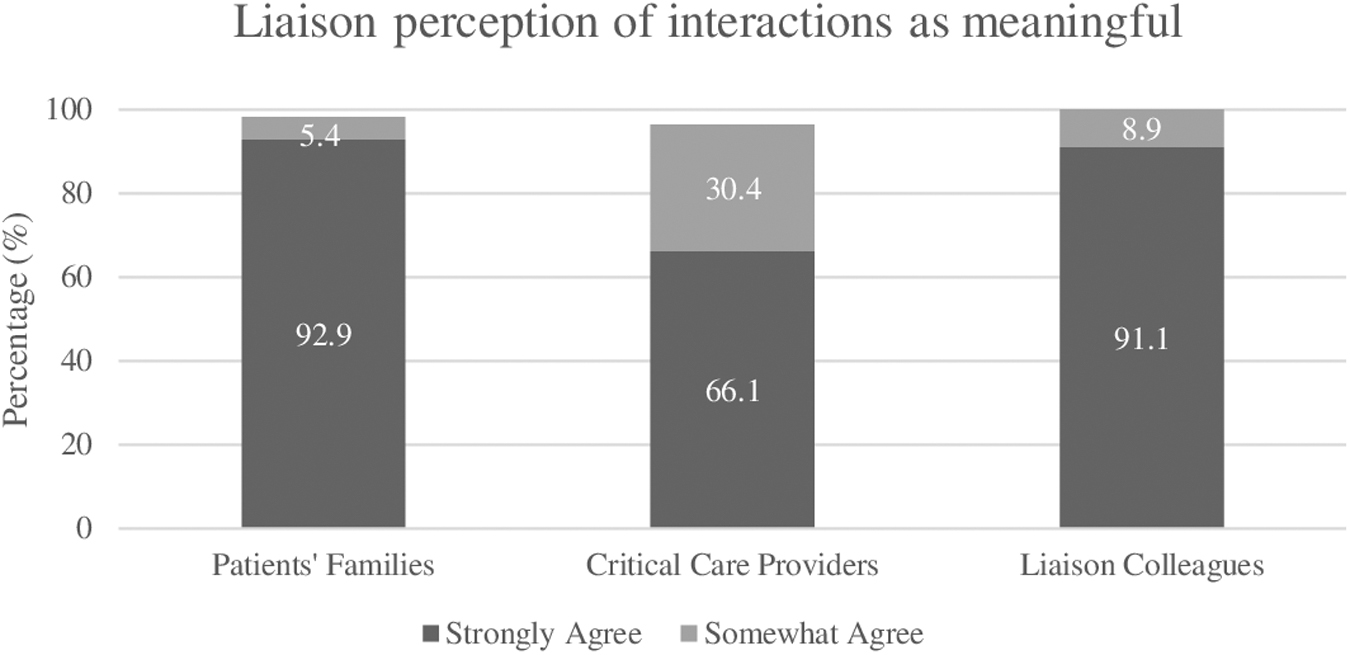
Proportion of liaisons who agreed or strongly agreed with statements asserting that they found their interactions with (1) patients' families, (2) critical care providers, and (3) liaison colleagues to be meaningful. More than 90% of liaisons perceived these interactions to be meaningful.
In the survey of intensivists, 94.4% of respondents concluded that the program provided a valuable service to families (Fig. 3). Additionally, 72.2% of ICU respondents agreed or strongly agreed that the program lessened the workload of the ICU team. Compared with self-reported baseline perceptions, at the end of the program, there was a statistically significant 38.9% increase (p = 0.04375) in intensivists strongly agreeing that they were comfortable with the liaisons communicating with families on behalf of the ICU team (Fig. 4).
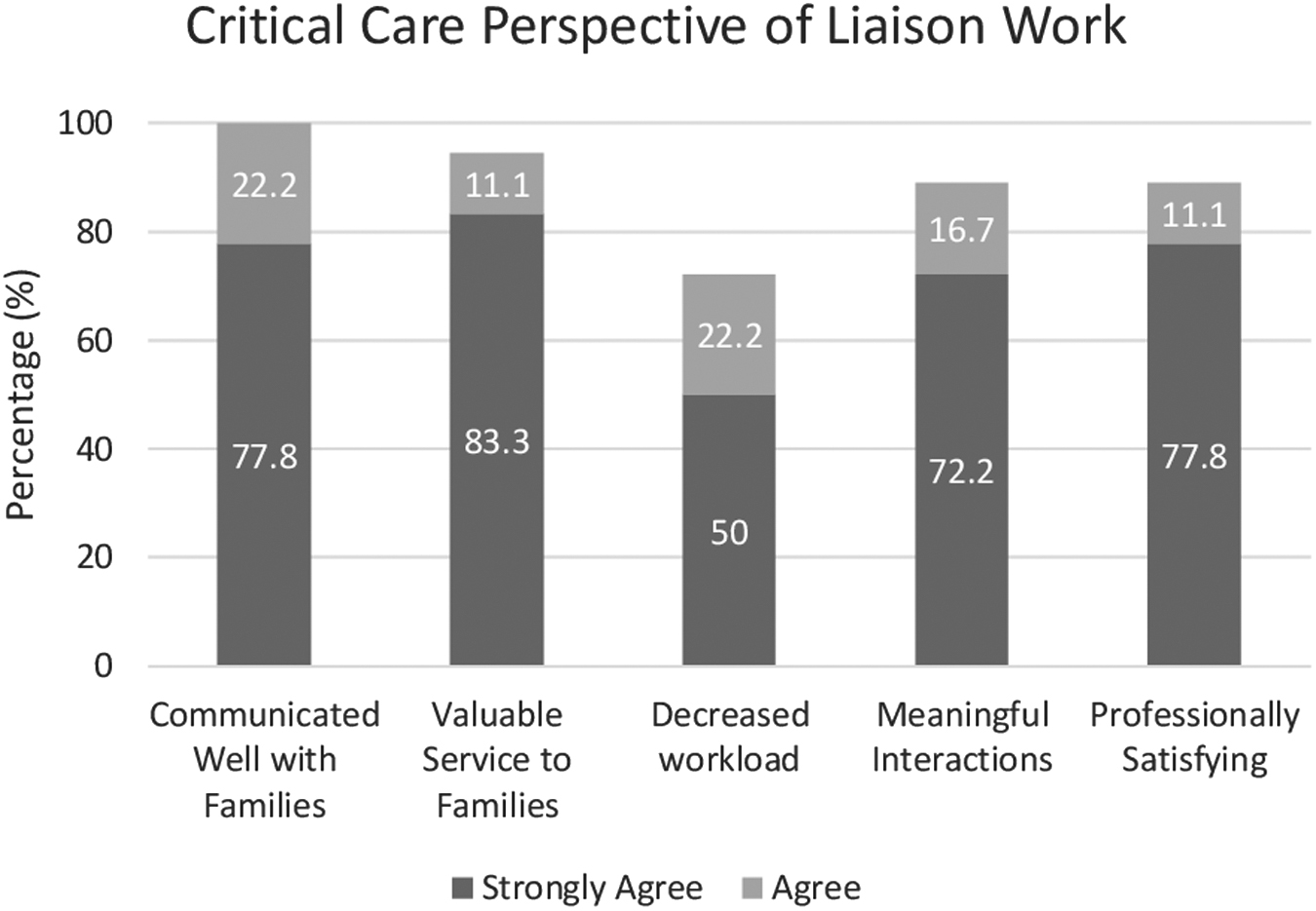
Degree to which intensive care physicians agreed with statements asserting that (1) “liaison providers communicated with families in a professional and effective manner,” (2) “the liaison program provided a valuable service to ICU patients' families,” (3) “the liaison service decreased the overall workload for the ICU team,” (4) “I found my interactions with liaison colleagues meaningful,” and (5) “I found my experience with the liaison service professionally satisfying.”
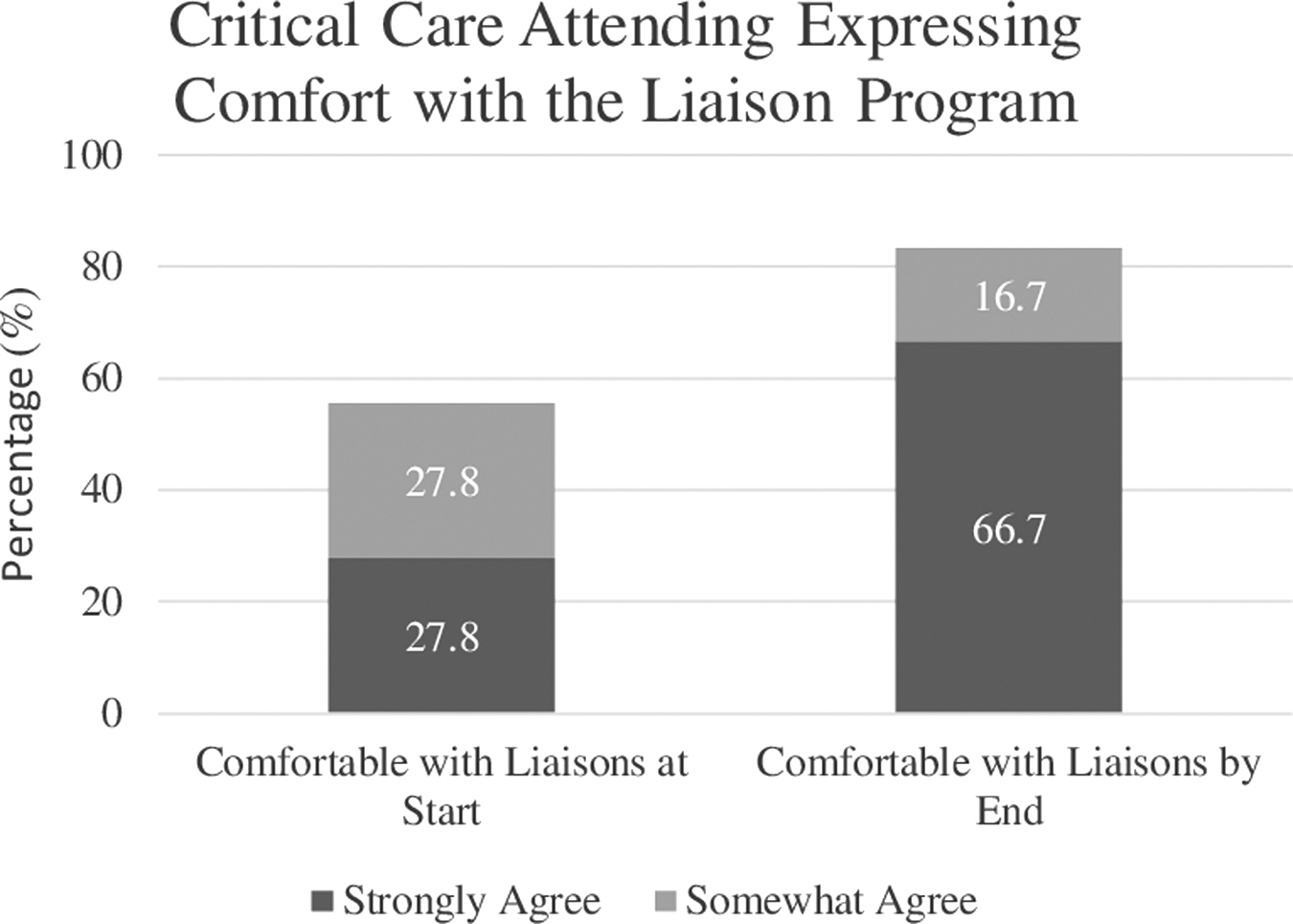
Proportion of ICU physicians who agreed with the statement that they were “comfortable with remote liaison providers communicating with patients' families on behalf of my ICU team” at the start of the program and at the end of the program. At the end of the program, there was a statistically significant increase to 2/3 of the participant respondents who strongly agreed that they were comfortable with this approach.
Participants were each asked how likely they were to recommend the RCLP to other hospitals facing a COVID-19 surge. Responses to this question were pooled into an overall participant experience value, utilizing methodology akin to the NPS,. 30 On a scale out of 100, intensivists' likelihood to recommend the program was 61.1 and liaisons' was 96.4. Liaisons were also highly likely to recommend participation as an RCLP liaison to a colleague (89.3). All liaison (100%) and 88.9% of intensivist respondents agreed or strongly agreed that participation was professionally satisfying. More than two-thirds (67.9%) of liaisons and nearly half (44.4%) of critical care provider respondents indicated that they would change their future medical practice based on their experience with the RCLP (Fig. 5).
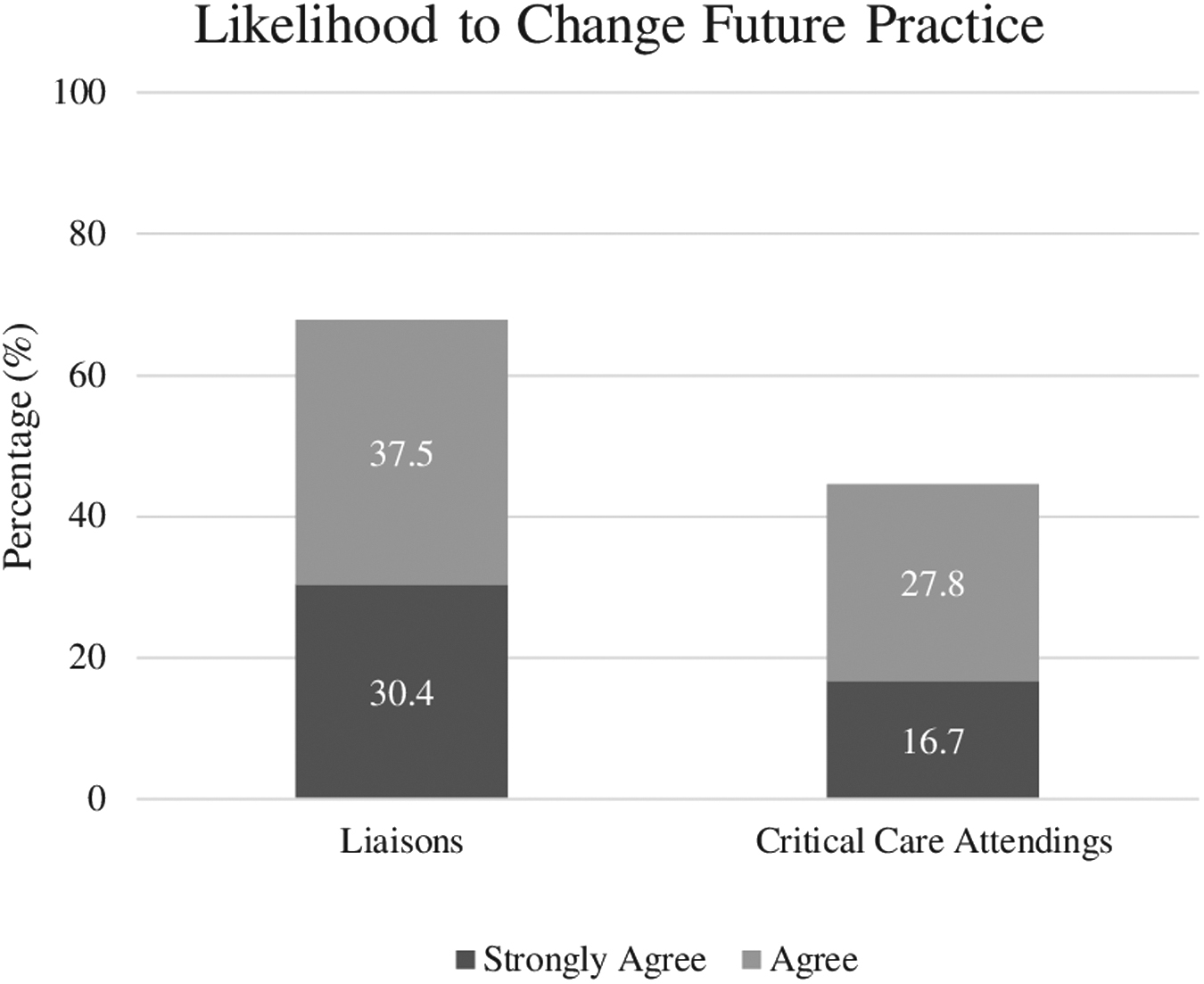
Degree to which liaisons and intensivists agreed with a statement asserting that “I expect to make changes to my future medical practice based on my experience” with the liaison program. 67.9% of liaisons and 44.4% of intensivists agreed or strongly agreed with the assertion of intent to change the way they will conduct their future practice.
Qualitative results
Respondents provided 219 free-text responses (liaisons n = 193, intensivists n = 26) from which 3 major themes were identified: (1) sense of purpose, (2) meaningful connection in a period of extreme isolation, and (3) opportunities for growth (Table 1). Descriptions of these themes with supporting quotations are illustrated below (Table 2).
Themes Derived from the Liaison and Intensivist Surveys With Associated Description and Illustrative Quotes
ICU, intensive care unit.
Theme 1: Sense of purpose
Many free-text responses invoked an enhanced sense of purpose. Liaison participants reported that they volunteered because their own clinics or procedures were temporarily reduced due to the COVID-19 surge or because their own medical history or family factors prohibited redeployment as frontline providers. This left them with an initial feeling of idleness during the global health crisis. The RCLP offered a meaningful way for providers to contribute to the pandemic effort despite barriers. Intensivists also indicated that participation enhanced their sense of purpose to relieve family suffering.
Theme 2: Meaningful connection during extreme isolation
Participants widely described how the program provided a means for fostering meaningful connections through interactions with patients, families, and colleagues during a period of extreme isolation. Liaisons described family affirmations of how valuable they found the reliable communication between the ICU team and loved ones. Multiple liaisons highlighted the impact of listening to families' stories about the patients' lives, noting the power of conversations to foster humanistic connection despite the physical separation necessitated by the pandemic. Additionally, the program provided an opportunity for colleagues across specialties to interact, forming lasting relationships.
Theme 3: Opportunity for growth
The final theme was that the program provided an opportunity for personal and professional growth for the participants. Liaisons acquired new skills from shadowing, coaching, and working with palliative care specialists. Both liaisons and intensivists noted improved compassionate communication skills and increased comfort with end-of-life conversations. Liaisons and critical care providers acknowledged learning from the deep and varied expertise of their RCLP colleagues.
Discussion
The RCLP was established to support patients' families and ICU teams through a severe COVID-19 surge, which presented unprecedented challenges to the care of critically ill patients. Despite the program's rapid implementation, liaisons felt well prepared to provide support for patients' families and ICU teams. Liaisons and intensivists perceived benefit to patients' family members. Furthermore, participants derived unexpected benefits reporting an enhanced sense of meaning, connection, and personal and professional growth. Approximately two-thirds of liaisons and nearly half of intensivists, including physicians with more than 10 years of experience, reported that the RCLP experience would change their future practice of medicine.
Our primary purpose for the RCLP was to provide connection and comfort for families who could not physically be with their critically ill loved ones. The literature supports the use of liaisons or FNs in the ICU setting.18–20 A randomized pilot study by Torke et al demonstrated that FNs can be integrated into the ICU to provide consistent clinical updates and emotional support. 18 Similarly, a quasi-experimental design study by Shelton et al showed that the implementation of family support coordinators can result in a statistically significant increase in the family's understanding of their loved one's treatment and condition. 19
Additionally, a randomized controlled trial by White et al demonstrated that working with nurse support navigators, as part of a multicomponent family-support intervention, can significantly elevate the quality of clinician–family communication during their loved ones' hospitalization. 20 This type of communication has been associated with higher ratings of patients' end-of-life care, as experienced by bereaved family members. 1 Liaisons can benefit families of ICU patients by providing consistent updates and improved communication.
Liaisons and intensivists alike overwhelmingly perceived that the RCLP achieved this intended benefit for families. By eliciting feedback on how the liaisons perceived proficiency with the requisite palliative care skills to benefit families, our study provides insight into real-time professional development for practicing clinicians. Despite rapid deployment of liaisons with limited ICU experience, this program was effective in advancing participants' knowledge and confidence through accelerated training, evolving online resources, and coaching. 16 While many studies look at longitudinal training for improved communication skills in the ICU,21,22 some studies like ours have demonstrated that brief focused trainings on end-of-life communication skills can impact self-reported efficacy for communication.23,24
Despite having little prior critical care knowledge, liaisons reported significantly increased confidence in their ability to comprehend critical care charts, discuss end-of-life care, and handle highly emotional conversations. As detailed in the study by Lipworth et al, 16 the RCLP employed crowd-sourced reference materials, electronic health record tools, peer-to-peer coaching, and a robust escalation system to quickly prepare liaisons for their unfamiliar functions. These survey results demonstrate that such methods can indeed result in improved confidence, knowledge, communication effectiveness, and palliative care during a crisis.
In addition to achieving substantial benefit for families, the surveys also indicate the RCLPs other core purpose was met: decreasing ICU workload between ICU teams and families. Ninety-eight percent of liaisons perceived and 72.2% of critical care providers confirmed that the program decreased workload for intensivists. Our survey did not identify objective reasons for the 26% discrepancy between the liaisons' and the intensivists' perception. Nevertheless, a 72.2% endorsement of the RCLPs impact on ICU workflows among intensivists indicates a high degree of endorsement, even if not to the level perceived by the liaisons. Intensivists credited the liaison daily communication as invaluable to families and to ICU teams, and they were highly likely to recommend the program to other hospitals.
Our study indicates that the RCLP had a third unanticipated benefit beyond supporting families and offloading ICUs: participants reported transformative growth. More than two-thirds of liaisons and nearly half of intensivist respondents, including physicians with more than 10 years of experience, reported an intention to change future practice based on their experience with the RCLP. The implication that participation may have a lasting impact on participants' careers was an unexpected finding. We did not directly collect information on which aspects of program experience were influential in participants' likelihood to change future practice. However, all three themes identified from the free-text survey are plausible drivers of the lasting professional impact.
Liaisons repeatedly described their sense of purpose and self-worth as a key personal benefit of RCLP participation. Studies have shown that working in high stress environments, such as ICUs during the spring 2020 COVID-19 surge, can have unfavorable mental health outcomes.10,25 However, several protective factors have been associated with reduced risk of burnout in such environments, including a strong sense of purpose and professional self-worth.26,27 Multiple liaisons not only emphasized the meaningful nature of their work but also contrasted the positive impact they derived from that work with the negative emotions they believed they would have experienced in its absence.
In addition to garnering a sense of purpose from providing meaningful service to patients and colleagues, participants noted the opportunity for growth. Liaisons noted markedly improved skills with end-of-life communication. The isolation from family to protect them from infection and work fatigue increased risk for moral distress, defined as a psychological burden experienced as a result of challenging situations. This may be associated with suboptimal decision making for patients. 10 Improving end-of-life communication among health care providers is an important step to improve decision making with families.25,28 Liaisons built upon pre-existing interpersonal skills and empathy to counteract challenges of physical separation of families from their critically ill loved ones. Despite the stressful nature of liaison–family interactions and the potential for distress, liaisons overwhelmingly reported in the quantitative and qualitative components of the survey that their experience was positive and meaningful, in part because of the growth they achieved through the program.
The liaisons and intensivists reported that this program fostered an environment to form new and meaningful colleague connections. Firew et al conducted a cross-sectional survey of health care providers during the COVID-19 pandemic, which noted that isolation, particularly aloneness exacerbated by the pandemic, had a negative impact on the mental health of frontline workers. 5 Many frontline workers chose to live apart from their pre-surge cohabitants to mitigate the infectious risk to their loved ones, furthering isolation. The RCLP provided consistent connection with colleagues and families, thereby lessening extreme isolation.
Once the first surge subsided, there was a shift back to pre-pandemic functioning, including fewer ICU patients and a return of families to the bedside. These conditions, along with improved understanding of optimal COVID management, decreased the need for liaisons. Furthermore, our liaison volunteers returned to their prior clinical duties limiting time to act as liaisons. However, this program can be reinstituted or replicated elsewhere in periods of analogous crisis. Additionally, the rapid establishment and ultimate efficacy of the RCLP in achieving its aims suggests that elements of the program can and should be leveraged even in periods of more routine operation, when additional communication support could be helpful for individually complex patients or challenging families.
Limitations
Our study has limitations. First, we report perceived benefit to patients' families rather than direct impressions from families themselves. In-depth family interviews have been completed to directly measure impact and will be reported in a subsequent article. Second, this program was conducted at a single institution. While we think this program can serve as a model for future programs, it is possible that the effects may not be universal across other institutions or in other locations. Third, the circumstances surrounding the implementation of this program, namely the intensity and uncertainty of the initial surge of the COVID-19 pandemic, may not be applicable in future pandemics if circumstances differ. Fourth, while the results are promising as a means to offset potential burnout associated with pandemic work, this study did not directly measure burnout, moral distress, or burden.
Conclusions
The COVID-19 RCLP was rapidly implemented amidst a global pandemic; it trained providers to provide daily communication with families while easing intensivist workload. The RCLP exceeded expectations, not only because it was need-driven, but because it was peer-driven via crowd-sourced wiki reference materials, coaching teams, and a strong overall sense of community. Program liaisons and intensivists perceived invaluable benefit to patients' families and for themselves. Participants described how they experienced a sense of purpose, created meaningful connections, and seized professional growth opportunities. This article demonstrates that even during a crisis it is possible to rapidly teach effective communication and end-of-life discussion skills, both of which will have long-lasting impacts on the individual participants and on their medical practices.
Footnotes
Acknowledgments
The authors are indebted to the liaison participants, intensivists, patients, and families without whom this program would not be possible.
Authors' Contributions
N.M.: Writing—original draft (lead), writing—review and editing (lead), formal analysis (equal), data curation (supporting), project administration (equal), validation (equal), visualization (equal). A.D.L.: Conceptualization (lead), formal analysis (equal), data curation (lead), investigating (lead), project administration (equal), validation (equal), writing—review and editing (supporting), visualization (equal). Y.L.: Formal analysis (lead), validation (supporting), writing—review and editing (supporting). L.B.: Validation (supporting), writing—review and editing (supporting), visualization (supporting). M.H.: Data curation (supporting), formal analysis (supporting), writing—review and editing (supporting). E.C.: Conceptualization (supporting), methodology (supporting), validation (supporting), supervision (supporting), writing—review and editing (supporting). A.C.M.: Conceptualization (supporting), methodology (supporting), validation (supporting), supervision (lead), writing—review and editing (supporting), visualization (supporting). S.K.: Conceptualization (supporting), methodology (supporting), validation (supporting), supervision (supporting), writing—review and editing (supporting), visualization (supporting).
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.