
Abstract
Background:
The events surrounding the COVID-19 pandemic have created heightened challenges to coping with loss and grief for family and friends of deceased individuals, as well as clinicians who experience loss of their patients. There is an urgent need for remotely delivered interventions to support those experiencing grief, particularly due to growing numbers of bereaved individuals during the COVID-19 pandemic.
Objective:
To determine the feasibility and acceptability of the brief, remotely delivered StoryListening storytelling intervention for individuals experiencing grief during the COVID pandemic.
Setting/Subjects:
A single-arm pilot study was conducted in the United States. Participants included adult English-speaking family members, friends, or clinicians of individuals who died during the COVID-19 pandemic. All participants engaged in a televideo StoryListening session with a trained StoryListening doula.
Measurements:
Participants completed a brief follow-up telephone interview two weeks after the StoryListening session. We describe enrollment and retention data to assess feasibility and conducted a deductive thematic analysis of the follow-up interview data to assess acceptability.
Results:
Sixteen clinicians and 48 friends/family members enrolled in the study (n = 64; 75% enrollment), 62 completed a StoryListening session; 60 completed the follow-up interview. Participants reported that the intervention was useful and offered a valuable opportunity to process their grief experience.
Conclusions:
The StoryListening intervention is feasible and acceptable for friends/family members and clinicians who have experienced grief during COVID. Our intervention may offer an accessible first-line option to address the increasing wave of bereavement-related distress and clinician burnout in the United States.
Introduction
The COVID-19
In a majority of cases, bereaved individuals are gradually able to cope effectively to reduce the grief associated with their loss. 6 However, as with any form of coping, a lack of social or emotional resources and competing stressors can impede the process of coping, including in bereavement.7,8
While there are evidence-based interventions to reduce grief in bereaved adults, including web-based interventions,9,10 many involve an extended number of sessions, often with a trained therapist, and are focused on resolving complicated or prolonged grief—persistent and pervasive grief that characterizes a clinical disorder. However, there has been a shortage of specialist grief services and a lack of resources to meet the increased need and burdens on those offering grief services during the pandemic. Further, complicated grief exists in only approximately 10% of bereaved people, 11 and less intensive interventions may be beneficial for those coping with grief, but who do not meet diagnostic criteria.
Evidence suggests that emotional regulation strategies, in which individuals influence which emotions they have, when they have them, and how they experience them, 12 are key to coping with grief. 13 Storytelling is one way that individuals may exert control over complex emotions and can be a powerful tool to process distressing experiences. 14 Storytelling has been used in several contexts, including bereavement, to manage emotions and reduce distress.15–17 While storytelling can be helpful, social norms may prevent individuals from sharing their bereavement stories. 18
Doulas are nonmedical care providers specifically trained to make and hold safe space and be a compassionate presence during intense times, including around death and grief.19,20 Telling one's story of grief to a nonjudgmental, nondirective Doula may offer the benefit of storytelling, while avoiding the perception of overburdening friends or family members, or the potential financial costs and/or stigma associated with accessing advanced-practice mental health professionals. 21 There is an urgent need for remotely delivered interventions to support those experiencing grief, particularly due to growing numbers of bereaved individuals during the COVID-19 pandemic.22,23 Thus, we use a novel approach of offering a remotely delivered Doula-led storytelling intervention.
The purpose of this work is to determine the feasibility and acceptability of a brief, remotely delivered doula storytelling intervention to support healthy grieving among individuals experiencing the death of a person during the time of COVID. As defined by the National Institutes of Health (NIH), 24 feasibility involves assessment of enrollment, intervention retention, and completion of assessments. Acceptability explores the willingness of participants to engage in the intervention; our goal was to identify reports of the difficulty and value of participating in the intervention.
Methods
We conducted a single-arm pilot feasibility trial of the StoryListening Doula program from June 17, 2020 to April 27, 2022.
StoryListening intervention
A StoryListening Doula focuses specifically on inviting and listening to experiences of the bereaved, as perceived and narrated by those participants. Doulas offer an engaged, neutral, and accepting presence, validate through attentive listening, and normalize suffering and loss. Doulas do not advise, provide medical explanations, psychotherapy, arguments, agreements, or false reassurances. StoryListening Doulas have completed professional certification and extensive additional project-specific training to ensure that they are nondirective and let the storyteller/participant guide the depth and direction of each session. Training also includes recognizing levels of participant distress that might require urgent clinical attention, accessing an on-call study physician and helping participants to access emergency mental health services in their local area and involving an on-call study physician.
Sessions were conducted by four Doulas via televideo. At the opening of the StoryListening session, the Doula opens space for storytelling by prompting either, “In your own words and in as much detail as you'd like, can you share with me your experience caring for patients during this time of COVID?” (for clinicians and staff), or “In your own words and in as much detail as you'd like, can you share with me the story of your recent loss?” (for loved ones, friends, or family members). Many stories unfolded without additional prodding. Doulas relied often on silence, but occasionally invited participants to expand (“Would you like to tell me/say more about…”).
Upon closing, Doulas identified key themes (if/when participant had not already done so), reflected the major sentiments/insights voiced by the storyteller, and expressed gratitude to the participant for sharing their story. Doulas also encouraged participants to journal should they continue to experience emotions around their loss.
Participants
While there are often differences in the grief experience of family/friends and clinicians,2,25 both groups experienced atypical death and dying situations and isolation from typical grieving support during the COVID-19 pandemic,22,23 and thus both groups were included in our study population. Adult, English-speaking family members, friends, or clinicians of any person who died of any cause during the COVID-19 pandemic were eligible for this study. Participants could reside anywhere in the United States. For clinician participants, eligibility required only that they were professionally involved in the person's care sometime during the hours, days, or weeks preceding their death. Participation required access to a device (e.g., phone, tablet, computer) with internet connectivity sufficient to support video conferencing. Participants were recruited via word-of-mouth, and fliers and advertisements distributed in the community, online, and through health professional networks.
Procedures
Potential participants contacted study staff via email or telephone and those who were eligible and interested were consented by phone by trained study staff. After completing a brief demographic interview, participants were scheduled for a StoryListening session, usually within two weeks of enrollment. During the StoryListening session, a palliative care physician (the lead investigator) was on call for any participants experiencing extreme distress. Data regarding enrollment and retention were recorded.
After two weeks, participants were recontacted to complete a brief follow-up interview, which included two open-ended questions to address acceptability: “In your own words, what was it like to share your experience during the StoryListening visit,” and “Did you find the StoryListening visit had any impact on your quality of life? If so, in what ways?” The study interviewer recorded participant responses in writing, as close to verbatim as possible. Study procedures, including regarding privacy and security of data, were approved by the University of Vermont Institutional Review Board (Protocol ID: 00000925) and all study staff had ethical and research training.
Analyses
We used descriptive statistics to describe feasibility, including rates of enrollment, intervention retention, and completion of assessments.
To assess acceptability, four study team members with expertise in the study protocol and qualitative analysis conducted a deductive thematic content analysis 26 on transcribed open-ended question responses. After familiarization with the data, team members identified themes and created a codebook based on the NIH definitions of acceptability. A priori acceptability themes included the (1) difficulty and (2) value of participating in the intervention. Themes were applied to transcript data. Emergent themes, including the reasons for participation, impressions of the doula approach, and acknowledgment of the need for additional effort, were also identified in the coding process and refined using the constant-comparison method. Similarities and discrepancies in the application of all a priori and emergent codes were discussed by the coding team until consensus was reached.
Results
Description of sample
A total of 64 individuals participated in the study, including 16 clinicians and 48 friends/family members. Participant characteristics are presented in Table 1. The stories that participants shared varied in duration as well as theme. Stories lasted a median of 45 minutes (range: 17–132 minutes). Both family/friend and clinician participants recounted expected deaths (i.e., known life-threatening illnesses) and unexpected deaths (e.g., COVID-19, accidents, suicide), which occurred in a number of settings, including homes, hospitals, hospices, assisted living facilities, and even outdoors.
Participant Demographics
GED, general educational development.
Feasibility
Intervention feasibility was assessed based on enrollment (including time to recruit), retention to the intervention, and completion of assessments. We enrolled 64 participants in 19 months, using largely passive methods (i.e., flyers) requiring participants to opt in. As seen in Figure 1, of the 85 potential participants who contacted the study team, 64 enrolled in the study (75%) and 62 completed a StoryListening session. Sixty (97%) also completed the follow-up interview and provided data on acceptability. No participants were identified as needing distress referral.
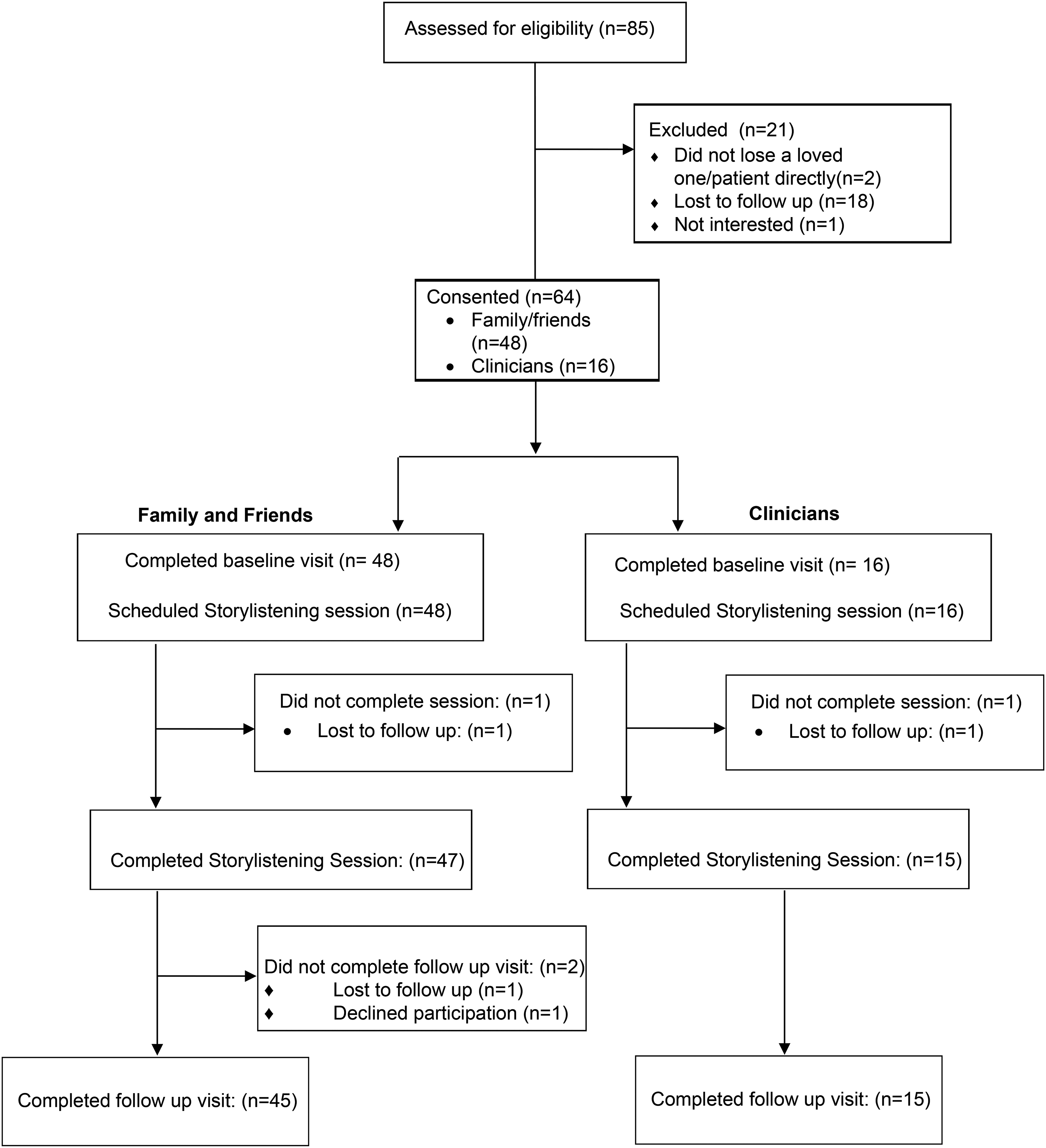
CONSORT flow diagram.
Our qualitative data suggest that a common motivation for participants was to help others by sharing their experience. For example:
I was hoping that it would do good somehow, not for me but for whoever was listening to it. To help people going into any related field to understand what people go through. (Participant 008, Friend/Family)
However, several participants were motivated to participate to create a memorial for the person who they had lost:
I knew that it was going to be recorded and that I could share with family. (Participant 006, Friend/Family)
Acceptability
Acceptability data were drawn from open-ended interview questions. Based on the NIH definitions of acceptability, a priori acceptability themes included the difficulty and value of participating in the intervention. Most participants reported that although participating in the intervention brought up some difficult emotions, the process was useful and even important. For example:
It was very difficult at first but then it became easier and I felt better after I did it. (Participant 020, Friend/Family) At times it was difficult, it brought up strong emotions. It was cathartic also to express those feelings. I welcomed the opportunity. (Participant 024, Friend/Family) It was easy to do. Cathartic. Helpful. Emotional. Insightful to where I am in my healing journey. It reaffirmed my values and my moral compass. I felt comfortable. I felt heard: [the doula] was a good listener. (Participant 053, Friend/Family)
Although a few participants reported no impact from participation, the vast majority reported that the experience was valuable, including those who reported feeling difficult emotions. In particular, participants described the intervention as providing an opportunity for processing, healing, or catharsis.
I hadn't realized I felt so traumatized so it brought up that. It was freeing, letting stuff go felt really nice. A little sad but it was healing to talk about. (Participant 007, Clinician)
It was good and necessary. There was so much grief and loss I couldn't lay on anybody. I needed this experience to get it all out and it really showed me it's much bigger, it's huge. Talking about the losses and suffering of employees, residents, and families was overwhelming. This is where an angel needs to come in and take over. This is too much for a human to bear. (Participant 010, Clinician)
Helped me decompress: take a heavy experience and externalize it. It was therapeutic in its own way. (Participant 031, Clinician)
Emergent codes, including impressions of the doula approach, and acknowledgment of the need for additional effort were identified in the transcripts. These themes provide context to the overall acceptability of the intervention. Participants attributed part of the benefit to the unique approach taken by the doula:
Very helpful to have someone to listen to the whole story start to finish. (Participant 017, Friend/Family) It was actually really great. As a palliative care doctor I'm taught to do a lot of the same things as a doula and I have never been able to tell my story to a totally nonanalytical person, not my therapist or a family member. It felt really good and really powerful. I felt better about being more reflective about my experiences. (Participant 049, Clinician)
Although both clinician and family/friend participants found the intervention valuable, an important difference was in the amount of additional effort participants reported needing after participation. Often friend/family participants appeared to be processing grief they had previously acknowledged, even if that grief had already been explored. For example:
I think maybe it was a let go of some things and the things that I hold guilt about, maybe it highlighted that more for me. (Participant 013, Friend/Family) It felt so good. It had been a long time since I had revisited the whole story. It helped me really appreciate how hard and lovely it was, both aspects. And it brought me to a new level of grief which I appreciated. (Participant 030, Friend/Family)
Conversely, many clinicians reported surprise about the grief they were experiencing, and acknowledged that their participation was an important beginning and recognition of the need for additional grief work:
[Participating was] eye opening. I realized there was a lot to unpack even though I didn't realize I had anything to unpack. (Participant 027, Clinician) It felt freeing to put a voice to things I didn't identify or wasn't willing to identify as trauma. It put in my face as “hey I need to work on these things” and reminded me to reach out to peeps and say “hey this is how I'm doing” and ask for help. It started the trajectory for how to work on it. (Participant 007, Clinician)
Discussion
Our remotely delivered StoryListening Doula intervention was feasible and acceptable for family members, friends, and clinicians experiencing grief over a death during the time of COVID. With millions impacted by death during the COVID-19 pandemic, and increasing barriers to accessing support, there is a need for more tools to address the expansive experience of grief in accessible ways.22,23
Although we relied on opt-in methods for recruitment, we were able to recruit a sample of 64 in 19 months during the COVID-19 pandemic, and 97% of participants were retained through the two-week follow-up. Participants reported, unprompted, several motivations for participation, including the desire to share their story as well as the desire to memorialize their loved one. This suggests the appeal of storytelling to those who have experienced grief. Even as many participants mentioned that study activities were emotionally difficult, there was overwhelming agreement that telling their stories was useful and important, which outweighed the difficulty.
There is long-standing research that suggests that the cognitive and emotional processing involved in constructing stories around stressful experiences can be useful tool in the process of making meaning out of different types of grief27,28 and can improve mental and physical well-being, particularly when there is a social aspect to the story-telling experience.17,29,30 In this way, having a nonjudgmental listener in the form of a doula can help tap into social benefits, without also activating potential feelings of conflict or burden that may be associated with sharing difficult emotions with friends or family members. 31
In addition, offering the intervention remotely can increase access. While the current article is focused on the feasibility and acceptability of the StoryListening intervention, future research can explore outcomes associated with engaging in storytelling with a doula, as well as the mechanisms that explain who may benefit and in which contexts. Moreover, similar narratives to those constructed in our intervention may be useful in clinical education to help bolster empathy. 32
Although not a replacement for a mental health professional, the StoryListening doula may offer a “first-line” option for bereaved individuals, particularly for those not coping with prolonged grief. Our data suggest that the StoryListening session may have been sufficient for some participants, particularly friends and family who had spent time before our study processing their grief. However, the intervention may have helped others recognize the need for additional support, such as counseling. This is particularly true for clinicians, several of whom reported being surprised by the emotions they felt. Clinician burnout was a pervasive issue before the COVID-19 pandemic 33 and has only increased. 34 Helping clinicians identify the need for help may be an important tool in preserving the clinical workforce.
Limitations
This study has important limitations. While our Doulas received extensive training, the Doula role surrounding end-of-life is not well-defined and this lack of standardization may limit generalizability. 19 Because we recruited using passive methods, we are unable to identify the broader population from which participants were enrolled. The intervention was offered only in English and for people who had access to Internet; our sample was also more educated and less diverse than the general population. Additional work, including a larger trial focused on efficacy, may help to tease out specific differences between friends/family and clinician experiences with the StoryListening intervention, as well as measure specific outcomes of intervention participation.
Conclusions
The StoryListening Doula intervention is feasible, and offers an acceptable and accessible way for bereaved individuals to share stories about their experiences with grief. Offering remotely delivered interventions for individuals experiencing grief may help address the increasing wave of bereavement-related distress and physician burnout in the United States.2,23,34
Footnotes
Authors' Contributions
R.G., F.A., and D.M.R. conceptualized the study. M.R., A.W., F.A., and S.P. conducted analyses. M.R. wrote the first draft of the article. All authors contributed to and approved the final article.
Acknowledgments
The authors thank Greg Brown and Matilda Garrido, as well as those who shared their stories as part of our research project.
Ethical Approval
This study was approved by the University of Vermont Institutional Review Board (Protocol ID: 00000925). The authors certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding Information
The Holly & Bob Miller Endowed Chair in Palliative Medicine and the Kate Laud Story Fund at the Vermont Conversation Lab at the University of Vermont.
Author Disclosure Statement
No competing financial interests exist.