
Abstract
Background:
Despite Advance Care Planning recommendations for patients with cancer, many lack Advance Directives (ADs). AD disparities persist among Black, Indigenous, or People of Color (BIPOC) patients. Based on a hypothesized correlation, we examined the association between patient-perceived cancer incurability and AD completion.
Methods:
This cross-sectional study obtained self-reported AD completion and incurability perception from routine care surveys. AD completion by incurability perception was estimated using modified Poisson regression. Subgroup analyses examined patients who were BIPOC, White, and had solid organ malignancies.
Results:
Our sample (N = 1209) was predominantly female (70%), White (73%) with early-stage disease (60%), and solid organ malignancies (82%). AD completion was 42%, and 40% of patients reported their cancer incurable. Patient-perceived incurability was not associated with increased AD completion (likelihood ratio 0.94, 95% confidence interval 0.78–1.13) in overall or subgroup analyses.
Conclusion:
Patient-perceived cancer incurability was not associated with AD completion, even accounting for race/ethnicity and cancer type.
Introduction
Advance Care Planning (ACP) is a process of conversation and/or documentation, which allows patients to convey their values and goals as they relate to their medical care, should they be unable to participate in medical decision making. 1 Benefits of ACP include improved quality of life, increased goal-concordant care, decreased postmortem family member distress, and reduced health care expenditures in the last week of life without change in survival.2–4 The American Society of Clinical Oncology 5 and National Comprehensive Cancer Network 6 have recommended ACP since 1998 and 2001, respectively.
Within ACP, the Patient Self Determination Act of 1990 shifted the focus to completion of an Advance Directive (AD), a common form of written ACP, which can be used by a patient's clinical team and surrogate decision maker. 7 Similar to ACP, AD benefits include improved goal-concordant care, decreased decisional burden for others, decreased in-hospital death, and lower utilization of feeding tubes and mechanical ventilation in the last month of life.8–11 Barriers to AD include factors related to logistics (time, new patient without established relationship), physicians (uncertain prognosis), and patients (difficulty accepting prognosis).12,13
Heterogeneity of AD completion in relation to end-of-life outcomes is a common criticism of AD studies. Patient preferences and AD completion may evolve over the course of disease, especially given challenges in prognostic awareness, namely comprehension of incurable disease and its implications. Across multiple studies, 32% to 82% of patients with stage IV solid organ cancers describe their disease as curable.14–16 A study assessing patients with metastatic non-small cell lung cancer found 68% of patients reported their disease as incurable, while 69% indicated the goal of therapy was to eliminate all of their cancer. 17 Moreover, little is known about the relationship between patient perception of incurability and AD completion. 18 Furthermore, awareness of incurability may disproportionately influence groups known to have low AD completion, such as patients who are Black, Indigenous, or People of Color (BIPOC), or have hematologic malignancies, where cancer may be incurable but with long survival. 19
We hypothesized that patients who perceived their disease as incurable would have a higher rate of AD completion compared with those who saw their cancer as curable. We anticipated that this difference would persist among BIPOC and White patients, and that it would be more pronounced in patients with solid organ rather than hematologic malignancies.
Methods
Study design and participants
This single-institution cross-sectional study included patients with cancer receiving care at the University of Alabama at Birmingham (UAB) from December 2016 through August 2021. Included patients had available patient-reported outcome (PRO) data; surveys were administered as part of routine care. Other inclusion criteria included age over 18 years and sufficient English proficiency for survey completion, although surveys could be completed by proxies with the patient. Implementation occurred across clinics at different times, with breast cancer and gynecologic oncology earlier than other groups. This study was approved by the UAB Institutional Review Board (IRB-300001910).
Outcome
The PRO survey asked, “Do you have an advance directive (a written document that describes the medical care you want in the future, or who you want to make decisions for you if you can't make them for yourself)?” Available responses were “yes” and “no.”
Exposure
Patients were asked to reply to the statement, “My cancer is curable” with available responses “yes” and “no.”
Patient characteristics
Demographics and clinical characteristics, including age (at time of data compilation), sex (male, female), marital status (married, not married), cancer type (breast, gastrointestinal, genitourinary, gynecologic, hematologic, other), stage (0, I, II, III, IV/progression/recurrence, hematologic), and phase of care were abstracted from the electronic medical record (EMR). Patients were grouped by stage into early (0/I/II/III) and late (IV/progression/recurrence). Phase of care was defined as initial (diagnosis to 12 months afterward), survivorship (12 months after diagnosis to 6 months before death), and end of life (the 6 months before death).20–22 Self-identified race and ethnicity, as well as Eastern Cooperative Oncology Group (ECOG) performance status were captured on PRO surveys.
Statistical analysis
Descriptive statistics were calculated using frequencies and percentages for categorical variables and medians and interquartile ranges for continuous variables. Differences in characteristics, regardless of sample size, between patient groups with and without an AD were compared using standardized mean differences from Cohen's d (small effect: 0.2, medium effect: 0.5, large effect: 0.8) or Cramer's V. V of 0.1 is considered a small effect, 0.3 a medium effect, and 0.5 a large effect when comparing across two categories; 0.1 small effect, 0.25 a medium effect, and 0.4 a large effect when comparing across more than two categories. 23 The association between perceived curability and completion of AD was evaluated using likelihood ratios (LR), predicted probabilities, and 95% confidence intervals (CI) from a modified Poisson model with robust variance adjusted for variables previously described. Subgroup analyses were performed for BIPOC patients, White patients, and patients with solid organ malignancies. Analyses were performed using SAS© software, version 9.4 (SAS Institute, Cary, NC).
Results
Sample characteristics
Of 1209 patients with PRO survey data, patients were predominantly female (70%), White (73%), married (59%), had early-stage cancer without progression (60%), and had an ECOG Performance Status of 0 or 1 (74%, Table 1). A total of 28 patients (2%) did not identify as “Black or African American” or “White.” The most common types of malignancy were gynecologic (32%) and hematologic (18%). Treatment (47%) and survivorship (39%) phases of care were predominant. In the sample, 60% of patients perceived their cancer as curable.
Patient Demographics and Clinical Characteristics by Completion of Advance Directive (N = 1209)
BIPOC from patients self-identifying as American Indian/Alaskan Native, Black/African American, Native Hawaiian/Pacific Islander, Asian, or Other. Other cancers included: central nervous system cancer, head and neck cancer, thyroid cancer, lung cancer, melanoma, neuroendocrine tumor, skin cancer, soft tissue sarcoma, cancer of unknown primary, hepatobiliary cancer, and squamous cell carcinoma of penis/scrotum. ECOG performance status ranges from 0 (normal activity with no limitations) to 4 (bedridden).
BIPOC, Black, Indigenous, or People of Color; ECOG, Eastern Cooperative Oncology Group; IQR, interquartile range.
Completion of advance directives and association with perceived curability
AD was completed by 42% of patients. Of those who perceived their cancer as curable, 57% had completed AD, whereas 43% of those who perceived their cancer as incurable completed AD (Table 1). In adjusted analysis, there was no difference in the likelihood of AD completion by disease curability (LR 0.94, 95% CI 0.78–1.13; Table 2). Predicted probabilities for AD completion were similar for patients believing their cancers are curable (0.37, 95% CI 0.31–0.44) and incurable (0.39, 95% CI 0.32–0.48). In subgroup analyses, no associations were found between disease curability and likelihood of AD completion among patients who were BIPOC (LR 0.93, 95% CI 0.60–1.44), White (LR 1.09, 95% CI 0.89–1.35), or with solid organ cancers (LR 1.10, 95% CI 0.88–1.36; Table 2 and Fig. 1 and Supplementary Table S1).
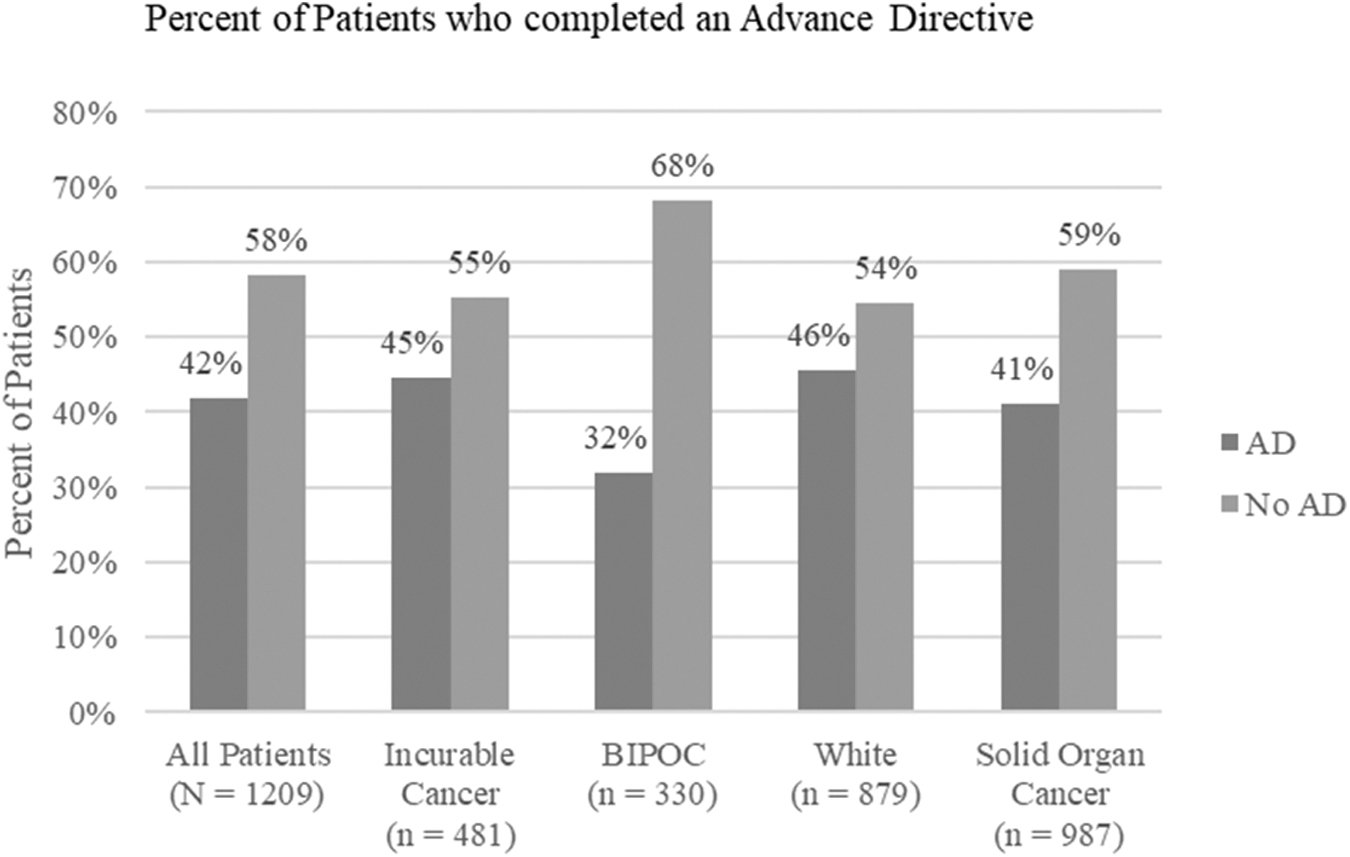
Percent of Patients who completed an AD, including subgroups by perceived curability, race and ethnicity, and solid organ malignancy. Patients who completed AD, when taken in aggregate as well as in subsets analyzed for sensitivity analyses. Incurable Cancer = as perceived by patient. AD, advance directive; BIPOC, Black, Indigenous, or People of Color.
Model-Estimated Likelihood Ratios, Predicted Probabilities, and 95% Confidence Intervals of Advance Directive Completion for All Patients, Patients Grouped by Race and Ethnicity, and Patients With Solid Organ Cancers
Models adjusted for age, race and ethnicity, sex, marital status, and disease-related factors, including cancer stage, phase of care, and ECOG Performance Status.
CI, confidence interval; LR, likelihood ratio; Ref., reference population.
Discussion
Less than half of patients in our study had completed AD. There was no association between perceived cancer incurability and AD completion overall, by race, or by cancer subtype. Age was a confounder for increased AD completion, but our model adjusted for this, and the difference was not clinically significant, as shown in Table 1 and Supplementary Table S1. The lack of association between perceived curability and AD completion addresses criticisms that lack of AD completion may be secondary to lack of prognostic awareness. This finding should be put in context of recent publications by Morrison highlighting the vast resources devoted to AD and ACP with the goal of better patient outcomes remaining unmet.24,25 Despite work to improve use of AD, meta-analyses and numerous trials have not shown overall positive impact. Furthermore, the specifics and complexities of future situations may not be reflected in AD and ACP, where hypothetical situations are used. For example, in one study, while end-of-life care was overwhelmingly (>90%) in line with patient's wishes from the perspective of families and physicians, it was consistent with preferences stated in AD in only 65% of cases. 26
Furthermore, goals may change over time once there is a diagnosis around which decisions can be made and as a disease progresses.27,28 Based on this literature and our findings, we recommend transitioning away from a focus on AD documentation as a quality metric. However, we note that AD is a poor surrogate for ACP, which retains value. Willis differentiates instrumental value from intrinsic value—the latter focusing on a person's story, which may help guide decision making rather than dictate it. 29 Sudore and colleagues outlined outcomes of specific interest for ACP, with highest priority assigned to goal-concordant care and designation of a surrogate decision maker. 30
The lack of a relationship between curability and AD may also reflect gaps in patient understanding as described earlier. These findings highlight the importance of clear and iterative communication about goals of care. While our study included potentially incorrect patient-perceived curability, as this perception likely informed decision to complete AD or not, it strengthens this study.
This study has limitations. It was conducted at a single tertiary center in the United States. The focus was AD specifically; therefore, broader ACP discussions may not have been captured which may relate to perception of curability. We also did not capture the accuracy of the patient's perception of curability. The health care team may have been more likely to approach those with incurable disease who lack prognostic awareness, which may result in overestimation of AD in patients who perceive themselves to be curable. An ACP tab was implemented in our EMR toward the end of the study period, which may have increased AD discussions, although this function was utilized more in the inpatient setting.
Conclusion
While AD is recommended for patients with cancer, uptake remains low. This is observed even among those who believe their disease is incurable. Results were similar among patients regardless of racial and ethnic background and when hematologic malignancies were omitted. Taking this study in context of the literature, we recommend turning focus away from AD and toward ACP—conversations of goals, values, and mutual understanding—processes to help patients create a framework for later concrete decision making.
Footnotes
Acknowledgment
The authors would like to thank Rachel Charles, MD for assistance on this project.
Authors' Contributions
C.M.P.: Writing original draft, investigation, conceptualization. N.E.C.: Methodology, formal analysis, and writing—review and editing. A.D.G.: Methodology, formal analysis, and writing—review and editing. C.P.W.: Methodology, formal analysis, and writing—review and editing. S.Y.: Investigation, and writing—review and editing. A.A.: Formal analysis, and writing—review and editing. G.B.R.: Conceptualization, supervision, writing—review and editing, and project administration.
Funding Information
No funding was received for this article.
Author Disclosure Statement
G.B.R.: Research Funding: Genentech, Pfizer, American Cancer Society Consulting: Pfizer, Gilead, Flatiron Travel: Gilead.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.