
Abstract
Purpose:
Individual genetic variation can affect both pain expression and opioid response. Large cohort datasets are required to validate evidence influencing genomic factors in opioid response. This study examined the feasibility of establishing an opioid pharmacogenomics registry for cancer patients containing longitudinal matched clinical, symptom, pharmacological, and genomic data, with an a priori feasibility target of 50 participants within 12 months.
Methods:
Consecutive patients with advanced cancer receiving opioids across five palliative care services were recruited. Clinical data (demographics, pain data, adverse effects, medications) and blood (DNA, RNA, pharmacokinetics) were collected over two time points. Patient and clinician qualitative interviews were conducted to assess acceptability. This study was approved by the SVHA Ethics Committee, Melbourne, Australia (HREC 252/18).
Results:
Enrollment for the registry was deemed feasible. Fifty-eight participants were recruited (median age 63.7, 45% female, 83% complete data), with the most frequent diagnosis being lung cancer (n = 18, 33%) and oxycodone the most frequently prescribed opioid (n = 30, 52%). Qualitative data indicated positive engagement from both patients and clinicians.
Conclusion:
Establishing a longitudinal opioid pharmacogenomic registry in patients with cancer receiving palliative care is feasible and readily acceptable.
Introduction
Pain is a common symptom among people with cancer, with prevalence rates of up to 66% for those with advanced disease. 1 Opioids remain the mainstay of cancer pain management, 2 with most (19 of 20) people experiencing at least moderate pain in a setting of cancer and who are able to tolerate opioids achieving pain, which is reduced to mild or no pain within 14 days. 3 Although population studies reveal that opioids appear to be equally effective and well tolerated, 4 individuals appear to respond unpredictably to different opioids manifesting as variable analgesic efficacy and/or adverse effect profiles.
This has led to the practice of “opioid switching,” where if an opioid is either ineffective or causes unacceptable side effects, it is replaced with an alternative. 5 This is implemented in up to one in five cancer patients, and although the underlying mechanisms are unknown, improvements may be seen in analgesic control, and reduction of adverse effects such as nausea, myoclonus, and or cognitive dysfunction. 5
Several factors may influence the initial choice of opioid, such as renal or liver dysfunction, pain etiology, comorbidities, and patient preference. 4 When these factors are inconsequential, clinicians use a “trial and error” approach for opioid switching. This can take time (which is often limited in those with advanced cancer) and may mean patients may experience poor symptom control until a suitable opioid is found.
It has become increasingly recognized that individual genetic variation can affect both pain expression and opioid analgesic and side effect profiles,6,7 and it may be an important factor explaining individual differences in response. 8
Pharmacogenomics is the study and translatability of genomic variation and how it influences the pharmacokinetic and pharmacodynamic profiles of a drug, thereby affecting an individual's response (efficacy/adverse effects). Over the past decade, the upsurge of pharmacogenomic research has identified various genomic influences on opioid response, on different steps of the pathway, such as the function of opioid transporters (e.g., P-glycoprotein), metabolism (e.g., CYP2D6, CYP2B6), receptors (e.g., OPRM1), and signal transduction and enzymes (e.g., ANKK1, COMT).9–12
International bodies have developed sophisticated methods to rate the quality of this evidence,6,7 and there is a growing evidence base on the clinical applicability of opioid pharmacogenomics in guiding clinical practice.10,13–15 The Pharmacogenomics Knowledge Base curates and updates summary information about the relationship between gene variants and drug response from published research and pharmacogenomic-based drug dosing guidelines. 6
The Clinical Pharmacogenetics Implementation Consortium is an international peak body for describing actionable pharmacogenetic variants, collating evidence and providing guidance for pharmacogenomic-guided prescribing, including those for opioids. 16 To establish pharmacogenomic dosing guidelines in this clinical setting, it is important to carefully describe the phenotype of those taking opioids in a clinical context, and to link this with genetic and pharmacologic information. 10
The evidence base evaluating pharmacogenomic-based opioid dosing guidelines remains limited. The European Pharmacogenetics of Opioid Study (EPOS) gathered point prevalence data of stable opioid prescription, pain type, pain relief, and genomic and pharmacokinetic data for patients with cancer and demonstrated associations between clinical effects and genetic variability.13–15 However, the EPOS group has also highlighted a number of inconsistencies in these data that require further examination.17,18
In an expert commentary published in Pain, Klepstad and Skorpen suggest a multi-faceted approach be taken to include basic research into cancer pain mechanisms and the role of genetic variability, clinical studies of selected populations, and subsequent clinical studies of “real world” patient populations encountered in practice whereby the role of genetic guidelines for therapy could be tested. 18 Similarly, Droney and Riley have called for a careful description of detailed phenotypes in the clinical context, and emerging adverse effects associated with opioids as a key area of focus. 10
To address these gaps, a study was conducted to establish the OPioid PharmacogenomiC (OPPtiC) Registry of matched longitudinal clinical, symptom, pharmacokinetic, and genomic data from patients with cancer pain.
This clinical registry would enable exploratory interrogation of genomic characteristics of patients matched to clinical outcomes to monitor change over time, and it would supplement existing registries in pain and palliative care.10,14 As a first step, this study therefore establishes feasibility and acceptance of the OPPtiC Registry of matched longitudinal data collection, before seeking the significant investment required for a larger scale registry.
Methods
Study design and setting
Phase 2 pilot study tested the feasibility of building a clinical registry of linked clinical phenotype and biological/genetic information from patients with cancer treated with opioids across five hospital cancer and palliative care services in Melbourne, Australia. The study was approved by the St Vincent's Hospital Melbourne Ethics Committee (HREC 252/18) and registered on the Australian New Zealand Clinical Trial Registry (ACTRN12619000591156) and date of registration: April 17, 2019.
Population
Adult patients with pain (defined by their treating clinician and of sufficient severity to have required opioid therapy) from any advanced cancer diagnosis receiving palliative care services, on the same opioid for at least three days before enrollment, English speaking, and able to complete the requisite patient reported study measures. Participants were recruited into two groups—the “switch group” for those requiring an opioid switch at enrollment, and the “control group” for those not requiring an opioid switch. The treating physician was responsible for the decision to switch opioids.
Data collection
Consecutive eligible patients were approached.
Data collection was undertaken at enrollment (T0) and seven days later (T1). Clinical trial staff collected study data, including patient-reported outcome measures at the two time points. The control group had the same opioid at both timepoints. For the switch group, the last dose of their initial opioid was at T0. They then switched to a different opioid immediately after T0, with data collected at day seven (T1) relating to their responses to the new opioid. The seven-day window was a pragmatic decision based upon the half-lives and times to steady state of opioids as well as convenience of attendance at hospital clinics. Data measures taken to populate the registry are described in Table 1.
Data Gathered to Populate the Registry, Collected at T0 (Enrollment) and T1 (T0 +Seven Days)
BPI-SF, Brief Pain Inventory - Short Form; CGI-C, clinical global impression of change; ECS-CP, Edmonton Classification System for Cancer Pain; EDTA, ethylenediaminetetraacetic acid; ESAS-R, Edmonton Symptom Assessment System-revised; MDAS, Memorial Delirium Assessment Scale; NUDESC, Nursing Delirium Screening Scale; S-LANNS, Self report - Leeds Assessment of Neuropathic Symptoms and Signs.
Interview Questions
Participants across sites who completed study data were invited to be interviewed, with interview questions exploring acceptability detailed in Box 1. Clinicians involved in data collection were interviewed at study completion.
Consecutive participants from across sites who completed T1 data at study mid-point (six to eight months) were invited to be interviewed and qualitative data collection continued until saturation was reached. Trial clinicians from the five participating sites were invited (and participated) in interviews.
Privacy of genomic data was managed in accordance with the Australian National Statement on Ethical Conduct in Human Research. 28
Outcome measures
The primary end point of feasibility for this study was considered, a priori, as the enrollment of 50 participants within 12 months as an indicator of recruitment and participation rates. This definition of feasibility was a pragmatic decision based upon the perceived ability to maintain clinical site enthusiasm for building the OPPtiC Registry and ensuring currency of the data within.
Secondary endpoints included percentage of those identified as eligible agreeing to participate, attrition across data collection points (patient-reported measures and blood sample collection), and views of acceptability (qualitative interviews). 29
Analysis
Descriptive statistics were used to report all feasibility measures. Qualitative acceptability data were subjected to a deductive thematic analysis, with data coding according to question stems within the semi-structured interviews. The qualitative analysis was conducted independently by two researchers (J.P., A.W.) who then met to compare, discuss, and reach a consensus on outcomes. As an exploratory pilot study, sample size calculation was not performed.
Results
Between April 2019 and May 2020, 58 participants (median age 63.7 [interquartile range: 55.4–72.9]; 45% females) were recruited to the OPPtiC Registry. Of these, 50 participants were recruited in the first 11 months across all sites, highlighting the feasibility of the study. Of the 190 screened, 92 were eligible and 58 consented (63%), including 34 switch group and 24 control group participants. The most frequent reasons for ineligibility and non-participation were poor performance status and logistics of care. Fifty-three (91%) participants had complete T0 data, and 48 participants (83%) had both complete T0 and T1 data (Fig. 1).
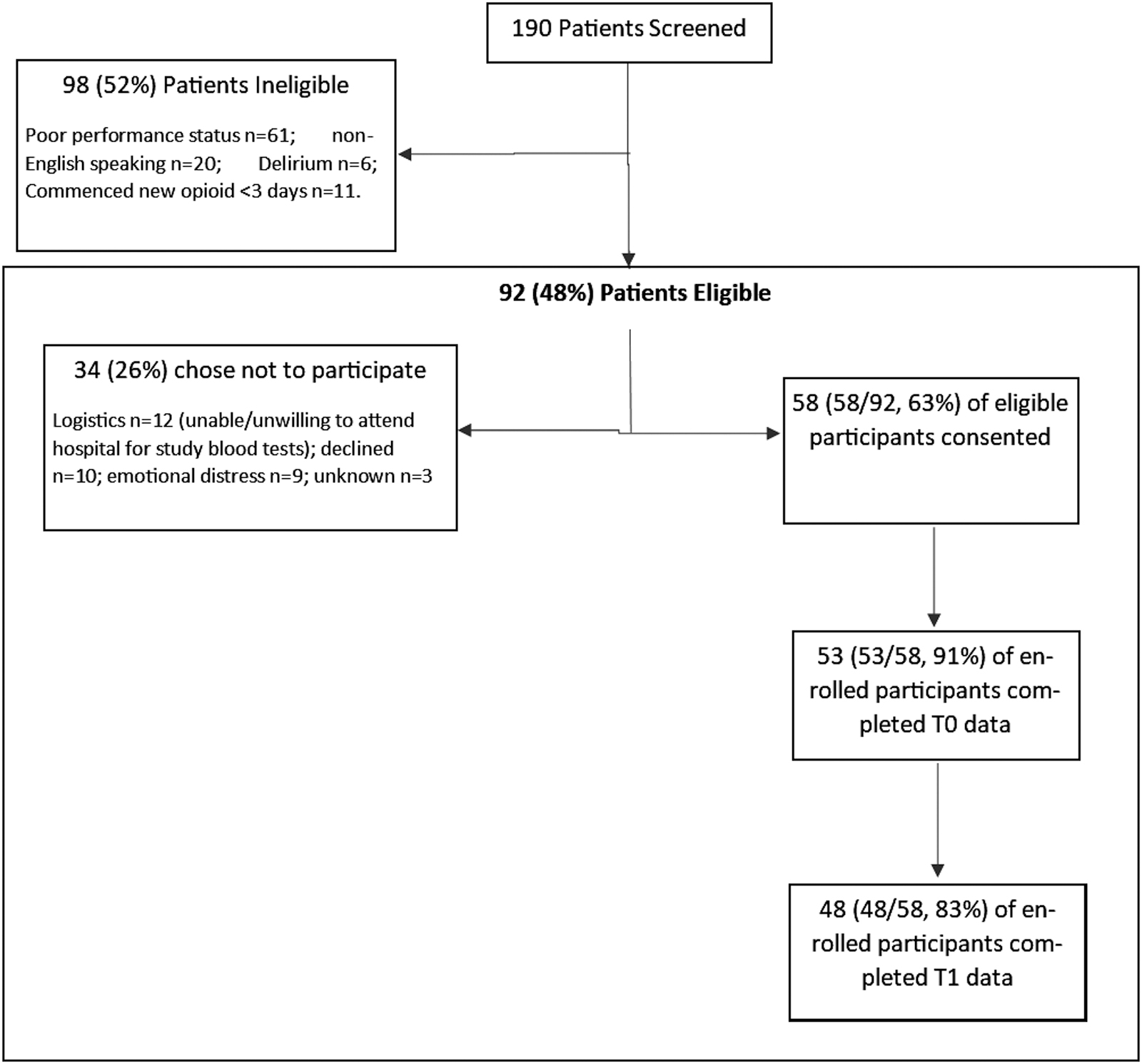
Eligibility and completion of participants.
The final sample (Table 2) had a range of cancer types, most frequently lung (n = 18, 33%) and upper gastrointestinal (n = 9, 16%), and the most frequent opioid prescribed for both switch and control groups was oxycodone (n = 30, 52%) followed by morphine (n = 10, 17%). Reasons for incomplete participant data largely related to difficulty obtaining venous access, 9% (5/58) at T0 and 14% (8/58) at T1, with all but one of these participants being inpatients in a palliative care unit and close to death.
Characteristics of Participants
GIT, gastrointestinal.
All trial clinicians involved in study recruitment (n = 5) agreed to be interviewed, including three nurses and two doctors, all of whom had previous clinical trial experience and had been in the role as trial clinician for median five years. Eight out of the 12 eligible participants agreed to be interviewed (five women, three men, median age 58 years) (Table 3). Qualitative data from clinical trial staff from each site highlighted that recruitment was relatively easy with “patients happy to participate, (and) quite interested,” the study outcomes were readily collected. However, four patients found the information and consent form unnecessarily complex and were “too tired to read it.”
Reflections from Study Participants and Health Professionals About the Study
“I thought the patients were surprisingly receptive to this. I never imagined that the populations that were very close to death would entertain the idea. But they have.” (Clinical trial nurse)
At study exit, participants reported high levels of satisfaction with involvement in the study, including unexpected benefits such as providing “relief from boredom” along with a sense of feeling involved in care. Although privacy was not a focus of the interviews, no concerns about the use of genomic data were expressed by patient participants. Rather, participants were seemingly engaged in the registry goals, with one participant commenting: “It is fascinating to be involved so early in the research. The project as a whole – bloods, questionnaires – are not an issue at all. … The proposal captures a really important need that is so obvious.”
Discussion
Personalizing analgesic therapy is an increasingly integral part of cancer care. This pilot study, assessing the feasibility of creating a registry of matched longitudinal biological and clinical data collection in a palliative care cancer population treated with opioids, suggests that establishing such a registry is both feasible and also acceptable for patients and clinicians.
Although recruitment to palliative care studies is always challenging, this current study, whereby 63% of eligible patients elected to participate, compares favorably with another multisite prospective observational palliative care study involving participant completed questionnaires and blood sampling, which cites recruitment rates of 15%–43%.30,31 Once enrolled, the attrition rate of 17% in this study again provides a favorable comparison to a median of 44% attrition rate in palliative oncological clinical trials. 32 These data highlight the high interest expressed by patients in this work and confirm the findings of White and Hardy, who showed that participation in research was not routinely conceived as an additional burden. 33
This study proves that collection of longitudinal data for a multi-site opioid genomics registry is feasible and acceptable. It is anticipated that going forward, more ambitious recruitment will be achievable, thereby enabling the registry's aims of exploring the associations between linked genomic, clinical, and pharmacological characteristics to predict responses of individual patients to specific opioids. The expanded registry will enroll at minimum 300 patients, providing valuable information for multi-omic interrogation.
Some initial areas for exploration include closer review of single or multigene variations in DNA and RNA on opioid response. In addition to exploring the frequencies of established opioid pharmacogenomic variants, the availability of this registry data allows for multi-omic analyses on linkages between the genome, epigenome, transcriptome, and pharmacokinetic data, and clinical phenotype to determine signals for future personalized opioid prescribing as well as mechanistic insights into opioid switching. The prospective longitudinal registry of an enriched cohort of cancer patients with severe pain is ideal for such interrogation.
A key limitation of this study is that participants represented only 31% (58/190) of screened patients, raising questions of biased representation, with implications for the generalizability of the findings. Moving forward, creating opportunities to collect data from patients earlier in their cancer illness may overcome the recruitment barriers of poor performance status, and enhance the representativeness of the sample.
This study has revealed the feasibility and acceptability of including palliative care patients treated with opioids in a clinical registry and answered several practical questions about patient and clinician engagement and participation. This is useful information, as the next steps are taken toward expansion of a larger multi-site opioid pharmacogenomic registry with the translational potential to transform opioid and symptom prescribing from a trial-and-error approach to one that is efficient, targeted, and personalized—the hallmarks of precision medicine.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by J.P., A.W., L.P., and B.L. The first draft of the article was written by J.P., and all authors commented on previous versions of the article. All authors read and approved the final article.
Consent
Informed consent was obtained from all individual participants included in the study.
Availability of Data and Material
The data supporting this work comply with the standards of the field.
Funding Information
This study was supported by peer-reviewed philanthropic grants from Research Endowment Fund, St Vincent's Hospital, Melbourne, the Bethlehem Griffiths Research Foundation, and the Australian and New Zealand College of Anaesthetists (Russell Cole Memorial Research Award).
Author Disclosure Statement
No competing financial interests exist.