
Abstract
Background:
Pediatric patients often undergo surgery during terminal admissions. However, the involvement and timing of palliative care consults in caring for these patients has not been readily described.
Objective:
To describe the presence and timing of palliative care consults for pediatric patients who undergo surgical procedures during terminal admissions.
Design:
Retrospective cohort study using data from the electronic health record.
Setting and Participants:
Pediatric patients who underwent at least one surgical procedure during a terminal admission at an urban, quaternary hospital in the United States from January 1, 2016 to December 31, 2021.
Main Outcomes and Measures:
Patients' medical, surgical, and admission-level characteristics were abstracted. Associations were evaluated between these characteristics and the occurrence and timing of a palliative care consult relative to surgery and death.
Results:
Of 134 patients, 84% received a palliative care consult during their terminal admission. Approximately 36% of consults occurred before surgery, and 12% were within one day of death. Children without a palliative care consult were more likely than children with a consult to die during surgery (19.1% vs. 2.7%, p = 0.02), have surgery within 24 hours of death (52.4% vs. 15.9%, p < 0.001), and undergo a full resuscitation attempt (47.6% vs. 12.4%, p = 0.002). Receipt of a palliative care consultation did not differ by patient sex, reported race and ethnicity, language, insurance, or income level.
Conclusions and Relevance:
Palliative care consults support high-quality end-of-life care for children and impact perioperative outcomes, including intensity of surgical care and resuscitation in the final hours of life.
Introduction
The number of children living with complex chronic illness is growing, and many of these children die in hospital settings.1,2 Recent increases in the number of inpatient pediatric deaths has coincided with an increase in the number of surgical interventions for children during terminal admissions. Up to 50% of children now undergo a surgical procedure during an admission that ultimately ends in their death. 2 The reported goals of these procedures include diagnostic, therapeutic, and palliative aims. 3 Decisions to offer and perform these procedures are affected by the input of a variety of teams that care for children during these admissions. These teams include, but are not limited to, intensive care teams, hospital medicine, surgical specialties, anesthesia providers, and, increasingly, palliative care teams.
Involvement of palliative care services allows for identification of goals of care and can help address shared decision making, a process that has been shown to reduce decisional conflict and improve patient and family knowledge. Prior research has confirmed that families desire to be involved in decisions regarding the care of their loved ones via shared decision making.4–7 During this process, families specifically wish for their preferences and values to be considered when making major life decisions. 5 It has also been demonstrated that lack of shared decision making can directly affect clinical outcomes. Of note, a recent investigation of extremely premature neonates found that parents would have selected a palliative approach significantly more often than intensive or invasive treatment if palliation had been recommended by clinicians using a shared decision-making model. 8
A growing body of literature has called for increased integration of palliative care in surgically managing children with serious illness as well as a collaborative approach between families, surgeons, primary care, and perioperative physicians.2,3,9–11 Additional emphasis has been placed on increased education surrounding the facilitation of palliative care discussions specifically for pediatric surgeons. 12 However, the literature has not described how the involvement and timing of palliative care consults relates to the frequency and timing of surgical interventions, or whether potential discrepancies in palliative care use exist across demographics. In this study, we sought to identify the frequency and timing of palliative care consults for pediatric patients who underwent a surgical procedure during a terminal hospitalization.
Methods
Study design, setting, and participants
This retrospective study assessed all pediatric patients (≤18 years old) who had a terminal inpatient admission at an urban, quaternary care hospital from January 1, 2016, to December 31, 2021, and underwent at least one surgical procedure during that admission. Patients admitted for acute trauma were excluded. Of note, the institution in this study has a high-capacity Level IV Neonatal Intensive Care Unit, advanced fetal care center, and is the only hospital in the state to offer a congenital heart program and pediatric extracorporeal membrane oxygenation. The medical facility likewise hosts a robust palliative care service consisting of two full-time physicians, several nurse practitioners, a bereavement nurse, social worker, and chaplain.
Historically, palliative care services are requested across all service lines but most frequently within the neonatal and pediatric cardiac intensives care units. The Medical University of South Carolina institutional review board approved the study and waived the requirement for informed consent given minimal risk to patients and use of retrospective data available within the electronic health record. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 13
Data collection
Sociodemographics (including self-reported race and ethnicity), primary diagnosis (including malignancy), comorbidities, extreme prematurity (defined as birth at <27 weeks gestational age), and quantitative encounter characteristics were collected for each patient. The occurrence and timing of an initial palliative care consult was identified by the presence of an order and completed consult note in the electronic health record. Patient records were also assessed for a recent hospital admission or emergency department evaluation within the six months before terminal admission. For each patient, the details of death were manually abstracted. These details included hospital location (intensive care unit, regular ward, operating room) and any resuscitation measures received. Manner of death was abstracted as comfort (no prior invasive therapies received), no escalation (received advanced therapies but then no further interventions), resuscitation (received chest compressions, electrocardioversion, intubation), or transitioned away from invasive care (care shifted from life-sustaining therapies to comfort focused, noninvasive care). Patients who were admitted at birth and did not survive to discharge were described as “never discharged.” Household median income by zip code county was obtained via the South Carolina Census State Data Center as reported by the South Carolina Revenue and Fiscal Affairs Office. 14
Statistical analysis
Descriptive statistics were determined for patient demographic and clinical characteristics. Chi-square or Fisher's exact test, when appropriate, were used to test univariate associations of categorical patient characteristics with whether or not the patient received a palliative care consult, a consult within 24 hours of death, and a consult before surgery. A Wilcoxon rank-sum test was used to evaluate associations with continuous patient characteristics. Multivariable analyses were not considered owing to sample size limitations. Competing risk regression was used to account for death as a competing risk when evaluating associations of patient characteristics with the time when they received a palliative care consult. All statistical assumptions were checked graphically, and transformations were considered if needed. All analyses were conducted in SAS v9.4 and R v4.1.
Results
Cohort characteristics and association with palliative care consults
Of the 134 patients included in this study, 57.5% were women and 42.5% were men. For patients with a reported race and ethnicity, 8.2% were Hispanic, 35.8% were non-Hispanic Black, and 50.7% were non-Hispanic White. The median age was four months (range: 0 months to 18 years), and 74.6% of patients were less than one-year old.
Of all patients, 113 (84%) received a palliative care consult. Receiving a palliative care consult was associated with age less than one year, presence of a cardiac condition, and extreme prematurity (Table 1). Patients who were less than one-year old had 2.6 times the odds of receiving a palliative care consult [odds ratio (OR), 2.64; 95% confidence interval (CI): 1.00–6.98; p = 0.045]. Patients with a cardiac condition also had 2.6 times the odds of receiving a palliative care consult (OR, 2.65; 95% CI: 1.01–6.90; p = 0.042). Patients born extremely premature had 76% lower odds of having a palliative care consult relative to those not born premature (OR, 0.24; 95% CI: 0.07–0.77; p = 0.016). A larger proportion of patients who did not receive a consult had a malignancy versus those who did receive a consult (19.0% without consult vs. 6.2% with consult; p = 0.071). Receiving a palliative care consult was not associated with patient sex, reported race and ethnicity, primary language, insurance status, or median household income in the patient's zip code.
Patient Characteristics by Whether or Not They Received a Palliative Care Consult
IQR, interquartile range.
Hospitalization characteristics and association with consults
Compared with patients who did not receive a palliative care consult, patients who received a consult died later and had a longer LOS. However, for both groups, the median LOS exceeded two weeks (Table 2). More than half of patients in each group were admitted at birth and died before discharge. Compared with patients who did not receive a palliative care consult, patients who received a consult were less likely to undergo surgery within 24 hours of death (15.9% with consult vs. 52.4% without consult; p < 0.001). Conversely, there was an association between number of surgeries and palliative care consult, where patients who had more than one surgery had 3.5 times the odds of receiving a palliative care consult (OR, 3.50; 95% CI: 1.20–10.2; p = 0.022). Across the entire cohort, patients underwent a total of 337 procedures. These are described in detail in Supplementary Table S1, but the most frequent procedure types were abdominal (75 procedures, 22.3%), cardiac catheterization (64, 19.0%), or cardiac surgery (62, 18.4%) in nature.
Hospital Admissions Factors by Whether or Not Patients Received a Palliative Care Consult
Of note, the location and manner of death were both associated with having received a palliative care consult. A significantly smaller proportion of patients who received a palliative care consult died in the operating room as compared with those who did not receive a consult (three patients with a consult vs. four patients without a consult; 2.7% vs. 19.1% respectively; p = 0.021). Of the 126 patients who died within an intensive care unit, 42 patients (33.3%) died in the neonatal unit, 35 patients (27.8%) died in the pediatric unit, 48 patients (38.1%) died in the pediatric cardiac unit, and 1 patient (0.79%) died in the neurologic unit. Patients who received a palliative care consult were likewise less likely to undergo a full resuscitation attempt as opposed to those who did not receive a consult (12.4% with consult vs. 47.6% without consult; p = 0.002). Compared with those for whom palliative care was not consulted, patients who received a consult were instead more frequently transitioned away from intensive care (69.0% with consult vs. 38.1% without consult; p = 0.002). A similar proportion of patients without and without a palliative care consult received early comfort-based care and no intensive or life-sustaining therapies (4.4% with consult vs. 4.8% without consult). Receiving a palliative care consult was not associated with recent admission to the emergency department or hospital (Table 2).
Timing of consult relative to surgery and death
Of the 113 patients who received a palliative care consult, 41 (36.3%) received the consult before surgery. Consults occurred within one day of death in 12.4% of patients and within three days of death in 22.1% of patients (Fig. 1). In patients with an LOS <14 days, a greater number of patients received a palliative care consult within the last day of life. Among all patients, roughly one in five had surgery within one day of death (Fig. 2), with a greater proportion among patients with an LOS <14 days (47%). In patients with an LOS exceeding 58 days, three patients (8.8%) underwent surgery within three days of death.
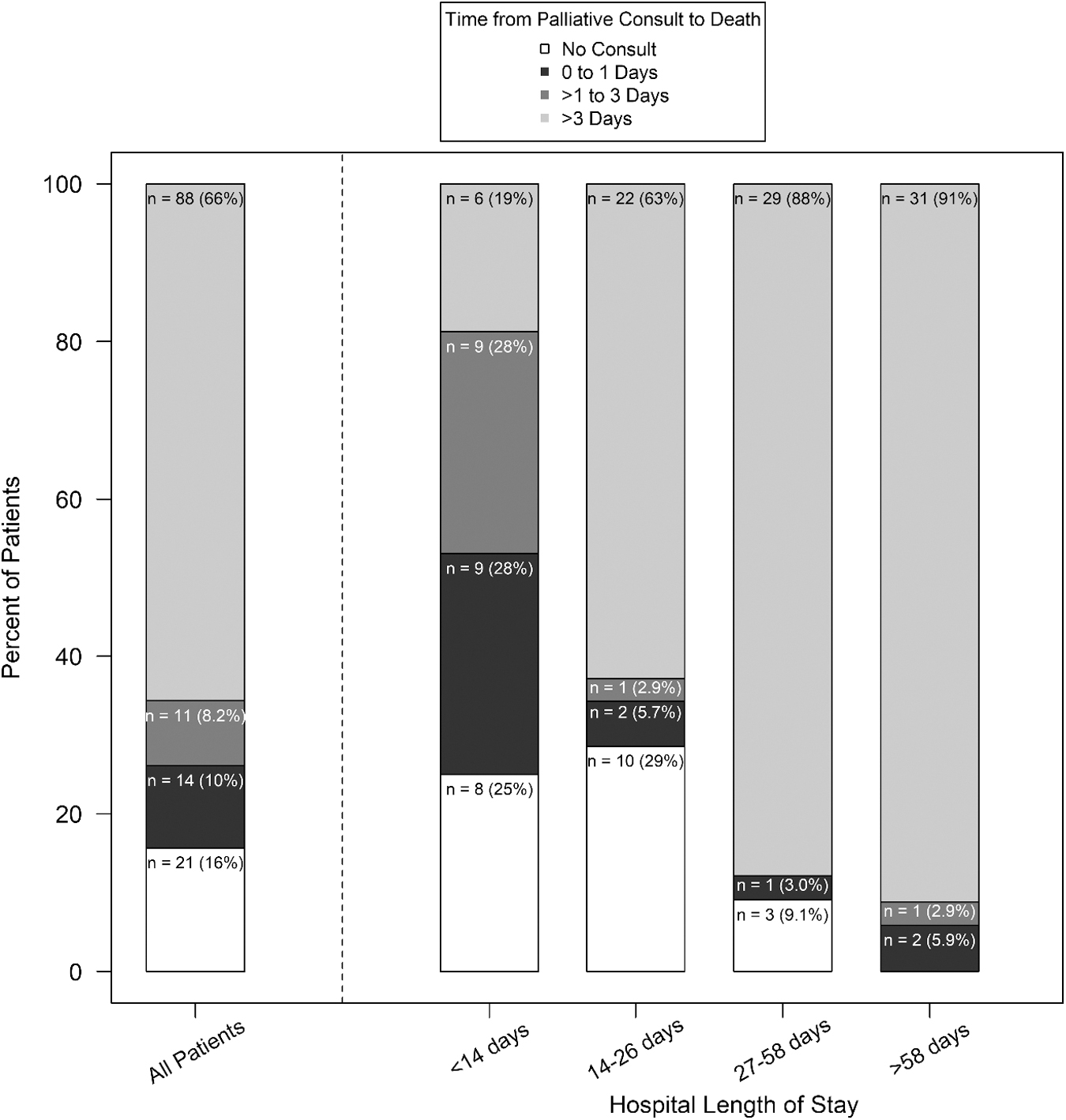
Proportion of patients who did and did not receive a palliative care consult overall and by quartiles of hospital length of stay.

Proportion of patients who died since surgery overall and by quartiles of hospital length of stay.
Discussion
In this retrospective study, we sought to identify the frequency and timing of palliative care consults for pediatric patients who underwent a surgical procedure during a terminal hospitalization and the characteristics of death of these children. Of the 134 patients who had a procedure during their terminal admission, we found that the majority of children received a palliative care consult. Of note, most consults occurred after at least one procedure, and a significant proportion occurred within the last three days of life. The receipt of a palliative care consult was associated with presence of a cardiac condition or age less than one year but was found to be less common in children with a history of malignancy or extreme prematurity.
Presence of a palliative care consult was not associated with patient sex, reported race and ethnicity, primary language, insurance status, or median household income in the patient's zip code in this cohort. Although we did not identify racial or ethnic disparities within our study patient population (as opposed to clear disparities noted in the previous work), 2 our study was not specifically powered to detect significant differences in a small cohort.
In addition to trends in consult timing and relation to specific patient conditions, we found whether a patient received a palliative care consult was associated with different locations of death. Of the 134 patients included for analysis, 94% died in the intensive care unit. However, a significantly higher percentage of patients who did not receive a consult died in the operating room compared with those who did receive a consult. Although the overall number of patients in our cohort who died in the operating room was small (seven patients), death in the operating room can be traumatic for families and care providers.
Although each of these patients had an order for full code preoperatively and underwent a complete resuscitation attempt in the operating room, we did not otherwise analyze the circumstances surrounding the intraoperative deaths or perform a multivariate analysis to assess for possible confounding between the two groups. However, the trend indicates an area of further research and potential improvement. Intraoperative deaths should rarely occur, and palliative care could benefit patients and families in preparing for and/or recovering from an intraoperative death.
In our patient cohort, we found that the manner of death was associated with receipt of a palliative care consult. A higher percentage of patients who received a consult were transitioned away from invasive care (69% vs. 38.1%). In contrast, a higher percentage of patients who did not receive a consult died during an attempted resuscitation (47.6% vs. 12.4%). These findings suggest that obtaining a palliative care consult may promote more goal-concordant care. This effect is important because health care providers frequently express concerns of conscience and moral distress in end-of-life care. In a multi-institutional study, many clinicians shared that they felt they were saving children who should not be saved, whereas a smaller number of clinicians expressed that they felt like they gave up too soon. 15 Greater involvement of palliative care professionals in navigating goals-of-care discussions and care-transition choices using a shared decision-making model represents another potential avenue for intervention.
Greater integration of palliative care is critical in caring for children with serious illness because these patients often undergo surgical procedures during their terminal admission. 16 These surgical procedures may be performed for a variety of reasons, such as relieving symptoms or suffering, clarifying the clinical diagnosis, or attempting a cure or rescue. 2 Approximately 20% of pediatric patients with cancer will have a major surgical procedure during a terminal admission, of which 20% will die within 48 hours of surgery. 17 A larger study of >30,000 pediatric patients found that nearly half of patients admitted for nontrauma diagnoses underwent a surgical procedure during their terminal hospitalization. 2
Another study found that among children undergoing surgery in the last six months of life, most had palliative care involved, more than one procedure, and a final procedure described as palliative in nature. 3 With such high stakes and a vulnerable population, the patient's primary medical team and surgical team must be supported in multidisciplinary decision-making and goals-of-care discussions with the patient and patient's family to ensure the goals of care align with the potential benefits and risks of the proposed procedure.
The palliative care team can be instrumental in facilitating goals-of-care conversations between the primary and surgical team members, patient, and patient's family. Despite this knowledge, many health care providers believe that palliative care consults occur too late for pediatric patients. 18 Similarly, guidelines recommend that pediatric patients receive early consults when they are diagnosed with a serious illness, such as malignancy or end-stage organ dysfunction. 18 This early involvement supports honest discussions about prognosis, goals of treatment, and open communication with patients and families, which improves the quality of care. 9 To align with the best practice of patient- and family-centered care, many health care providers consider palliative care involvement as a new standard of care for patients facing severe and potentially fatal conditions. 3
The results of this study should be interpreted in the context of a few limitations. First, the small sample size, single-center, and retrospective nature of the study could introduce bias and limit generalizability. Second, this study included patients who underwent at least one surgical procedure and died while hospitalized and excluded patients who had a terminal admission without undergoing surgery or who died after being transitioned to hospice. Our methodology thus may underestimate the number of patients who died shortly after operative intervention at another location (such as hospice or home) and likewise does not characterize or quantify the patients who may have been considered for surgery but ultimately deferred. Third, although our cohort reflected general trends in annual pediatric deaths (age at time of death and comorbidity burden), we had relatively few patients with a malignancy diagnosis, which may not accurately represent patients at other academic pediatric institutions. 1 Finally, we did not abstract specific characteristics and the purpose of the surgical interventions received by the patients, so we cannot describe how these factors may differ from surgical intervention patterns at other children's hospitals.
Conclusions
This study describes trends in palliative care consults for pediatric surgical patients during terminal hospital admissions and how these consults are associated with important patient outcomes. Our data suggest that even in a quaternary children's hospital with a well-established palliative care service and frequent use of consults during terminal admissions with surgical care, there remains room for improvement in the provision of high-quality end-of-life care to children with life-limiting illnesses. Although more studies in larger cohorts are needed to fully understand the effect of palliative care consults on patient outcomes and potential disparities in care delivery, our study uncovered valuable insights that could inform initiatives to advance the care of pediatric patients hospitalized with a terminal disease process.
Footnotes
Authors' Contributions
M.T. and J.A. conceptualized and designed the study. M.T., C.B., and N.B. collected data. B.J.W. conducted the statistical analyses. M.T., C.B., N.B., J.A., N.C.M., and B.J.W. contributed to drafting the article.
Acknowledgment
The authors thank Crystal Herron, PhD, ELS, of Redwood Ink, LLC, for her assistance preparing the article for publication.
Funding Information
No funding was received for this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.