
Abstract
Background:
Underserved Hispanic patients often experience unmet palliative care (PC) needs, particularly those with noncancer diagnoses such as Alzheimer's disease and related dementias. Most caregivers for Hispanic patients are family relatives who are less likely to use health care and community resources and experience high caregiver burden. We adapted a culturally tailored patient navigator (PN) intervention to provide support and improve PC outcomes for Hispanics with Alzheimer's disease and related dementias and their family caregivers (FCGs).
Objectives:
To explore Hispanic FCGs' experiences and perceptions of caregiving for a loved one, and how our PN intervention impacted their needs.
Design:
Qualitative descriptive.
Setting/Subjects:
FCG participants (n = 10) from our randomized control trial's intervention group were recruited from academic and safety net hospitals and community-based clinics across urban and rural Colorado in the United States.
Measurements:
Data obtained from individual, semistructured, 30-minute telephone interviews were recorded, transcribed, translated, and analyzed using NVivo and qualitative thematic analyses.
Results:
Four major themes emerged: Methods of Support, Cultural Expectations and Varying Family Contributions, Lack of Self-Care, and Awareness. Subthemes highlighted differing definitions of “contributing,” role resentment, and interpersonal issues. Varying familial expectations underscore FCG strain when the burden of caregiving is not shared. Participants used various coping strategies as necessary support and gained awareness through education, guidance, and referrals to resources.
Conclusions:
PNs helped FCGs and patients beyond the intervention's scope. Providing support and awareness to FCGs, and incorporating cultural beliefs, may improve PC access to disparate populations and guide future interventions. Clinical Trial Registration Number NCT03181750.
Introduction
Palliative care (PC) improves quality of life, symptom distress, and supports patients with serious illness and family caregivers (FCGs) to align goals of care. 1 Yet, underserved populations often experience unmet PC needs, for example, lack of an advance directive, increased symptom burden, and decreased hospice utilization, particularly those with noncancer diagnoses (e.g., Alzheimer's disease and related dementias [ADRD]), complicated by multiple comorbidities.2,3 It is well documented that Hispanic persons have higher rates of dementia and experience worse health outcomes compared with non-Hispanic White persons. 4
By 2060, the number of Hispanics ≥65 years is expected to quadruple, facing the largest increase in ADRD cases of any racial/ethnic group in the United States. 5 The Hispanic community is at higher risk for ADRD due to age and a higher prevalence of underlying cardiovascular disease, diabetes, high blood pressure, and obesity when compared with the non-Hispanic White community. 5 Hispanic older adults also have low rates of formal education, potentially lacking an important safeguard to cognitive decline.6,7 Since Hispanics experience a higher prevalence of ADRD, increased symptoms and/or pain, and comorbidities that impact care needs, these disparities can also potentially impact caregiver burden, stress, and well-being.8,9
Most caregivers for Hispanic patients are relatives and care for older adult family who are in poorer health than their non-Hispanic counterparts. 10 Compared with other ethnic groups, they spend more time caregiving, are less likely to use available health care or community resources, or have loved ones in a facility compared with other ethnic groups; consequently, they experience increased caregiver burden.9,11,12
There is a paucity of research addressing heath disparities in ADRD. 13 Persons from minority ethnic backgrounds and their FCGs remain underrepresented in traditional dementia efficacy clinical trials. 14 Our previous work found that a culturally tailored lay patient navigator (PN) intervention is feasible in cancer and noncancer Hispanic populations and improves key PC outcomes: advance care planning (ACP) completion, pain, and hospice use and acceptance.15–19 As part of a larger randomized control trial of Hispanic patients with comorbid medical illness, patients with ADRD who lacked decisional capacity and relied on their FCG as proxy were ineligible to participate. 20 With supplemental funding, we aimed to adapt and pilot test our PN intervention in self-identified Hispanic patients with clinically significant ADRD (lacking capacity) and their FCGs. 20
To understand the experiences, concerns, and needs of intervention group Hispanic FCGs, we conducted this descriptive qualitative study. We also examined FCG perspectives around the PN intervention's effectiveness, contributing new insights into the ways Hispanic FCGs perceive and experience caregiving for family members with serious illness.
Methods
The Colorado Multiple Institutional Review Board approved this study, conducted between October 2016 and July 2021. Our established PN framework and manual were adapted to include dyadic participation: all patients who had comorbid medical illness and ADRD were enrolled with their FCG. 20 Participants were eligible if they were FCGs of patients who lacked decisional capacity due to ADRD. Intervention visits and outcome measures were directed toward the FCG, focusing on the patient's care. In the intervention group, bilingual/bicultural lay PNs delivered ∼five home visits and reviewed a bilingual educational packet addressing three PC domains: ACP, pain/symptom screening and management, and hospice. Additional details on the PN intervention are available in our previous work.17,18
Twenty-four patients enrolled from academic (3) and safety net (1) hospitals, and community-based clinics (6) in Colorado. PNs queried intervention arm FCGs (n = 12) about participation willingness in an interview poststudy; 10 consented. In July 2020, a team member (R.M.F.) conducted one-on-one qualitative phone interviews with English -peaking FCGs, uploading audio recordings into a REDCap database. 21 For Spanish-speaking FCG interviews, a bicultural and bilingual PN joined the team member and translated the interview. A nine-question, semistructured interview guide (Supplementary Data) explored FCGs' experiences and perceptions of caregiving, including assignment of cultural meaning and how the intervention impacted perceived needs and gaps. All interviews were transcribed; Spanish interviews were translated into English, back-translated, and reviewed for accuracy by three bilingual/bicultural PNs. FCGs received a $25 grocery gift card for their time.
We used NVivo 12 software to conduct thematic analysis through an inductive approach.22,23 Codes and themes were created and interpreted in context of the intervention's rationale (FCG needs and gaps) and perceived impact, enabling two coders to understand and contextualize the information provided by participants. 24 While we found thematic saturation in eight interviews, we gathered data from 10 participants to fully establish themes/subthemes. Participants' own words were grouped in identifiable sets of ideas. Transcripts were read multiple times for both macro- and microcontextualization through data immersion. A coding manual identified repeated words, phrases, feelings, or emotions, placing similar groupings into codes, further narrowing codes into subthemes. 25 Data coded independently by two team members resulted in 90% agreement. Any lack of compatibility in discussions was brought to the research team for consensus.
Results
Ten FCGs participated (Table 1). Seventy percent of interviews were in English; 30% in Spanish with real-time interpretation from another PN unknown to FCGs to reduce social desirability bias. We found four themes (Fig. 1): Methods of Support; Cultural Expectations and Varying Family Contribution; Lack of Self-Care; and Awareness. Table 2 displays themes, subthemes, and exemplar quotes.
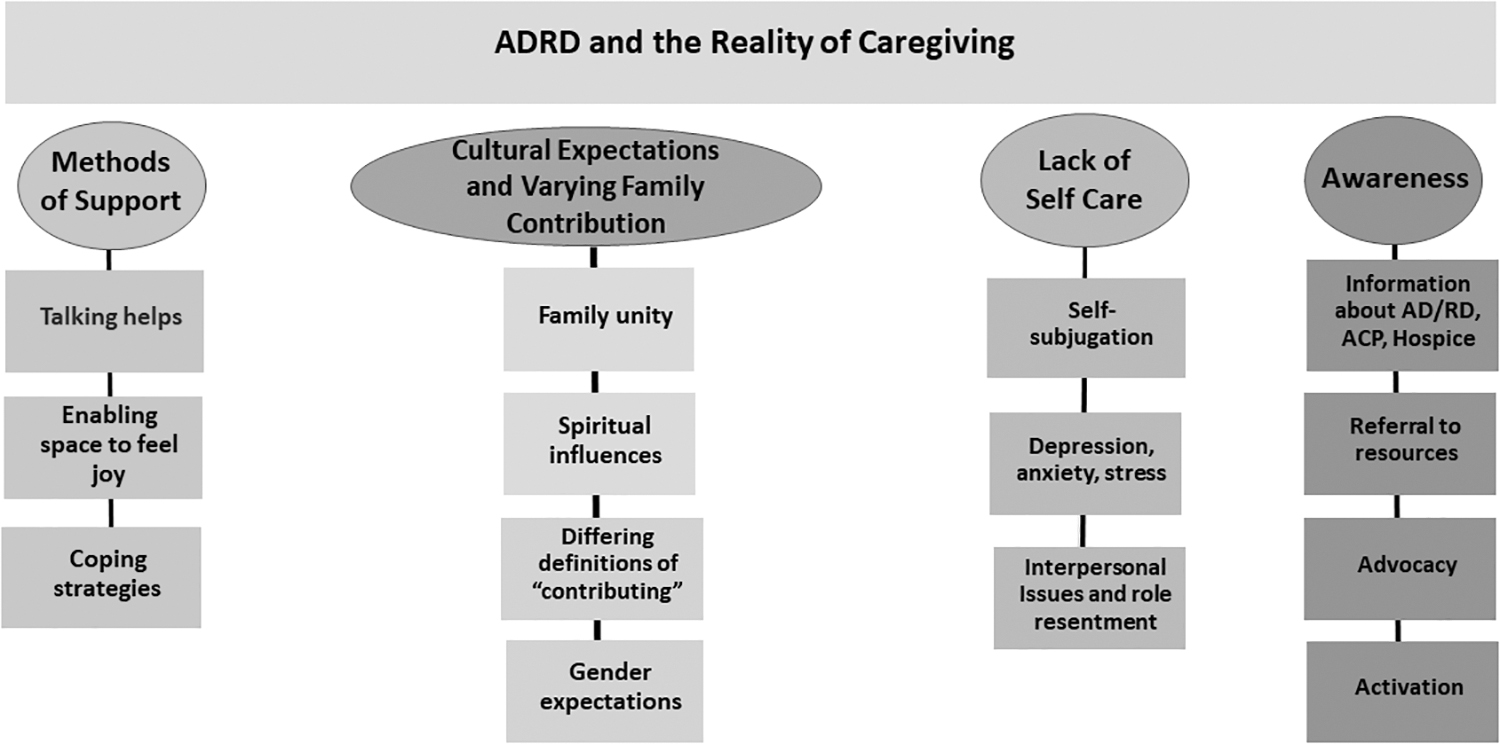
ADRD and the reality of family caregiving. ADRD, Alzheimer's disease and related dementias.
Demographic Characteristics of Family Caregiver Sample
One participant identified as American Indian or Alaska Native.
SD, standard deviation.
Themes, Subthemes, and Exemplar Quotes
ACP, advance care planning; ADRD, Alzheimer's disease and related dementias; PN, patient navigator.
Methods of support
The importance of talking about experiences and how different types of support, for example, various family members and PNs helped alleviate caregiving burden, was found, including subthemes: (1) Talking helps, (2) Enabling space to feel joy, and (3) Coping strategies.
Talking helps
Discussing caregiving revealed that most participants who mentioned having beneficial conversations with PNs discussed how good it felt to have someone with whom to share experiences. Participants spoke about feeling grateful for a PN listening when they felt anxious, stressed, depressed, and discussed how talking with family members, especially sisters, was helpful, sharing they were able to “release everything with each other.”
Enabling space to feel joy
Having additional family members visit at various times provided emotional support and enabled a support system that allowed participants to access feelings of joy, happiness, and love for the care recipient. One participant shared, “My grandma is 90. All I want to do is to be happy and not have any issues right now or anything. We're (all of us) just trying to keep her happy and safe until she's ready.” Another participant who shared caregiving responsibilities with his daughters described how he was “happy to take care of” his wife, which was less of a burden and more of an opportunity to spend time together with his entire family. A third participant explained how being able to care for her husband at home meant she could enjoy being with him and caring for him in a place where they were happy.
Coping strategies
FCG participants suggested several ways they were able to cope with the caregiving role. One participant voiced that what gave her strength was simply being able to stay with and care for her mother. Another participant mentioned having her family available to assist her even though she provided the bulk of caregiving on a day-to-day basis.
Another reflected on how the PNs provided her with coping strategies she and her sisters used with their mother and their father, who also served as an FCG. She explained, “Me and my sisters learned about an Alzheimer's expert and watched her videos on what they go through from the beginning to the end. Then they show what we can do to help.” She stated when she feels overwhelmed, she often relies on her younger sister to come home and provide respite to focus on herself. The same participant also shared how she uses blogging to keep herself motivated, stating that she often relies on her younger sister to come home and provide some respite to focus on herself when she feels overwhelmed. Finally, walking, exercising, and being in nature were suggested as coping strategies used by some participants.
Cultural expectations and varying family contributions
Participants spoke about family expectations, closeness among family members, and how caregiving was a privilege and a way to show love. Subthemes identified were as follows: (1) Family unity, (2) Spiritual influences, (3) Differing definitions of “contributing,” and (4) Gender expectations.
Family unity
Whether having shared responsibilities or being sole primary caregiver, participant responses revealed a sense of unity and respect within the family as beneficial. Participants spoke about cultural norms of keeping family members at home rather than in long-term care, noting how they would “never let mom go.” One participant shared, “In our culture we care for our parents when they're here. We don't send them to a home.” Another expressed how she was raised to respect and care for family regardless of what that person had done previously and to “be with her loved one until the end.”
Others shared how family members provided emotional support by offering respite even when the FCG had not asked for assistance. Participants spoke of differences between Hispanic and non-Hispanic cultures, sharing that caregiving is no different in the younger generations than in their parents' generations. One participant stated, “my mom took care of her mom before she passed, and everybody takes care of each other. And that's how me and my siblings are with my parents.” Another participant accepted responsibility based on a family decision that they, as a family, made “an early agreement that we would not send them to a facility.” Others noted emotional support from the family, stating “if I didn't have some of my family members, neighbors, friends, I'd be in a real downward spiral.”
Spiritual influences
Some participants attributed strength as a caregiver to spiritual/religious beliefs and practices. They often spoke of “praying and knowing,” as paramount to feeling they would be able to provide supportive effective care. One participant said her relationship with God helped her get through the day. Praying enabled her to feel close to God and the care recipient, feel at ease, and fulfill her duties. For others, understanding that the caregiving role is what is wanted or expected by God was what afforded them strength and happiness. Participants also leaned on their spirituality and relationship with God to give them strength through caregiving challenges.
Differing definitions of “contributing”
Participants shared ways families addressed caregiving duties, including different levels of contribution, a lack of shared understanding or willingness to engage in collaborative caregiving, and the expectations of different genders. A daughter-in-law serving as a caregiver for her spouse's mother described experiences with other immediate family members as having little interest in helping with care.
For others, a lack of understanding contributed to stress and burden of caregiving as one participant shared, “Me and my mom are the only ones that took care of her. We're really close as a family, but in regards to all her medical stuff, none of the family understands our role.” Other participants spoke of family members being available at times to help with the caregiving duties, but still did not fully understand the role of being a full-time caregiver.
Gender expectations
A few participants openly discussed cultural differences in caregiving roles expected of men and women. One participant described her relationship with her family as one that had very clear caregiving expectations of her as youngest daughter. There is an expectation that only female family members provide support. While male family members were available, the three daughters were the only ones who provided caregiving, and there was no tension about the expectation.
Other participants recounted how male family members would avoid helping with caregiving duties due to language barriers (e.g., speaking Spanish only, not feeling comfortable interacting with English-speaking health care providers, or attending medical appointments) or because of the emotional stress associated with being around their loved one's weakened and deteriorating condition. One participant mentioned her brother living in Mexico, “he doesn't do it (provide caregiving) because he says he gets depressed by looking at his father like this.” Instead, she relies on her niece to provide support if she needs respite or assistance.
Lack of self-care
Even though several participants indicated they were aware of the need to care for themselves, they also communicated failing to do so. Three subthemes emerged: (1) Self-subjugation, (2) Depression, anxiety, and stress, and (3) Interpersonal issues and role resentment.
Self-subjugation
Some participants appeared resigned to overwhelming feelings and stress of caregiving, stating that these are normal and expected parts of caregiving. Others viewed caring for a family member as a higher priority than their own well-being even when they expressed an understanding of the ramifications of depression, anxiety, and stress. Social isolation, financial challenges, and their own worsening medical conditions were often a result of unbalanced priorities. One participant shared, “I would like to do more for myself, but right now I just can't.” Another explained that even listening to music or watering her plants were not part of her routine because of her caregiving commitment.
Depression, anxiety, stress
For many FCG participants, caregiving appeared to take a toll on their mental health. One participant described feeling “desperate and unsure because right now [the care recipient] needs a lot of help.” Having to worry about issues with COVID-19 compounded her level of stress. Other participants described how even though they have support from family members, at the end of the day, “I still feel like crying,” and “the weight of the world is on my shoulders, and I don't have time for that five-minute phone call.”
Interpersonal issues and role resentment
A few participants discussed how having to be a caregiver contributed to feelings of resentment toward the care recipient and family members who were not willing or available to help with caregiving duties. One participant shared feeling “stuck” providing care for her mother-in-law when her husband went back to work. For others, having no support from immediate family led to tension. One participant stated, “I feel a lot of resentment” toward family members who refuse to provide assistance.
Awareness
A growing awareness of ADRD, resources, and available services as a result of the PN intervention identified four subthemes: (1) Information about ADRD, ACP, and hospice, (2) Referral to resources, (3) Advocacy, and (4) Activation to seek information and help from providers.
Information about ADRD, ACP, and hospice
Participants discussed appreciation for receiving helpful information from the PNs such as educational pamphlets and video links from the Alzheimer's Association about ADRD, ACP, and hospice resources. Others reflected on how talking with PNs provided new insights. Receiving information enabled the FCG to feel less tension and stress caring for her mother-in-law. However, another FCG participant shared they would have preferred their primary care physician/clinician to communicate better with their father about their mother's condition.
I would like the physician and more of [the team] to explain the disease to him so that he can understand what's happening to her and give him ideas about how he can deal with it because he doesn't know anything about it and it stresses him out. He's not understanding what my mother is going through. Me and my sisters do because we watch some videos about ADRD.
Referral to resources
Participants discussed the importance of receiving information from PNs about resources, for example, pamphlets about PC services and ADRD. Participants noted the positive experience of having a PN to provide answers to questions and follow-up on resources and other issues.
Advocacy
Participants mentioned that it felt good to know there were people in health care, for example, PNs and this program, who cared about their loved ones, providing support and encouragement, and empowering FCGs to speak up about concerns. PN were advocates in helping FCGs learn about the disease and the changes in the patient's health condition, accompanying patient/FCG to clinic visits, and being available to assist with phone calls with providers or attend family meetings, if desired by the FCG.
Activation
Others reflected on how speaking with PNs allowed them to feel confident in seeking information, asking further questions such as clarifying care goals, communicating with others about the illness, including the care recipient, and asking for provider's help. A daughter shared her experience of finally being able to communicate with her father because of her participation in the program and the support provided by the PN to role play discussions with health care providers and access community resources, when needed. PNs also help FCGs write questions down for their discussions with providers.
Discussion
In this article, we have critically analyzed FCGs' experiences and considered their cultural environment to discern support needs for Hispanic FCGs caring for older adults with ADRD. We presented experiences and participants' reflections of caring for parents, in-laws, or spouses. We identified insights regarding self-care, familial expectations, awareness of resources and information about ADRD, and the type and amount of support provided by our PNs including interactions with health care professionals. We also identified multiple themes where cultural and support systems impacted caregiving experiences through gender norms, satisfaction, and resource delivery.
Participants spoke openly about gender roles and caregiving expectations. The FCGs interviewed were mostly female, consistent with data on caregivers in general and Hispanic caregivers, specifically.8,26,27 Caregivers identified gender expectations of caregiving roles for women versus men in the family. Cultural values tied to gender role expectations potentially explain this relationship. Marianismo has expectations of female caregivers being the nurturer, self-subjugation, and being totally devoted to the family. 8 This may explain gender role inequality highlighted by some FCGs.
Previous researchers identified mixed findings in Hispanic caregiver burden. Hispanic caregivers have been shown to provide more hands-on care in a given day, care for loved ones with more substantial activities of daily living impairment, and have fewer home services compared with non-Hispanic White caregivers. 12 Regardless, researchers have been mixed on the perceived burden of this caregiving. Similar to our findings, caregivers have reported a sense of purpose and substantial perceived rewards and meaning in providing care. 11 This suggests the cultural expectation to care for one's family serves as a buffer to some of the emotional and physical strain of caregiving. However, researchers have shown that even with lower reported burden, Hispanic caregivers experience downstream negative health effects. 12
We identified themes that corroborated these findings with FCGs describing experiences of depression and anxiety. Future interventions to support Hispanic caregivers can incorporate support while acknowledging and honoring the rewards of being a caregiver. 8
Caregivers expressed high satisfaction and appreciation for education and information delivered by PNs. Reducing barriers to care is fundamental to patient navigation, and this includes addressing cultural and health literacy barriers through education and at times, translation.19,28 This is critical as Hispanic adults disproportionately experience communication challenges and lower health literacy compared with White and Black persons. In 2003, the National Adult Health Literacy study team reported that 41% of Hispanic adults had health literacy scores below basic, with only 4% having proficient health literacy to make complex medical decisions. 29 Researchers found similar results in a population-based study with 35% of Hispanic persons having inadequate health literacy, while another 36% had marginal health literacy. 30
Utilizing a bicultural/bilingual person from the community to address language barriers and provide culturally tailored information has the potential to overcome knowledge and communication barriers and help patients/FCGs prepare for what lies ahead. These results provide a rationale for future research examining how this PN intervention impacts health literacy.
Our findings confirm the relevance of key Hispanic values, identified through community-based research that has grounded our PN research program from its inception, including familia and personalismo. 16 The values of familia, personalismo, and additionally respeto were evident in the majority of interviews. Familia, the importance of family across all aspects of life, was identified by FCGs, including both the importance of family unity and in the frustration expressed when caregivers did not think others in the family were contributing enough to caregiving duties. Personalismo is a concept related to valuing a strong interpersonal connection and willingness to be of service to help others. 8
Our findings also show how personalismo may relate to a preference for care in the home by a person who is personally concerned for the loved one's well-being and the lack of personal connection in a nursing home or facility. Personalismo also underscores the importance of establishing trust and rapport, which was the main goal of our PNs' interaction with patients and their FCGs. Respeto is the belief that all persons, in particular parents, need to be treated with respect, courtesy, and humility. Respect guides the hierarchy of power within family dynamics. 8 Our results suggest that while FCGs described their experience as difficult, it was not seen as a burden but rather an opportunity to feel satisfied that they have done all they can do while fulfilling their responsibilities within their family. 31
While this qualitative analysis is based on a small FCG sample, recruitment was from multiple urban, rural, and frontier communities across Colorado, offering a more diverse perspective. The majority of our FCG participants were adult children rather than spousal caregivers, which is reflective of caregiving patterns for Hispanic persons in general. 32 Our findings generally confirm previous evidence about Hispanic caregivers.8,27 Unique to our study is inclusion of FCGs of persons with more advanced ADRD who are estimated to be in the last year of life. These FCGs may also be uniquely facing the death of their loved one. In addition, given the expected exponential growth of this population and the relative dearth of research, deepening scientific understanding into the perspectives of Hispanic caregivers has the potential to further inform programs and PC research interventions to improve care for older Hispanic adults with ADRD and their caregivers.
Conclusion
We provide a snapshot into the caregiving experience of 10 Hispanic FCGs, highlight challenges, and ways of coping with caregiving. While FCGs experience common frustrations, the ways in which they coped reflect unique experiences, through a cultural lens that can be used to guide future interventions. We underscore a lack of FCG self-care and identify varying familial expectations, which highlight their strain when the burden of caregiving is not shared. PNs can successfully address cultural and educational PC barriers for FCGs in multiple settings. Additional research is needed to identify best practices and evidence to support ADRD caregivers and must examine relationships between cultural values, beliefs, and influences of family support on the extent of perceived burdens, to inform supportive interventions for these caregivers.
Footnotes
Acknowledgments
We wish to thank our PNs who made this research possible: Julianne Mendevil, Irazema Mino, Diane Pacheco, Jeannette Rodriguez, and Jesus Tolivar Bustamante. Appreciation to our participating study sites: University of Colorado Health (North, Central, South), Centura Health (North, South), Denver Health Medical Center, Kaiser Permanente, Colorado Mountain Medical, Mountain Family Health System.
Authors' Contributions
R.M.F.: Conceptualization, methodology, acquisition of data, formal analysis, and writing—original draft preparation. K.G.V.: Formal analysis, data interpretation, and writing—original draft preparation. D.M.K.: Project administration, methodology, investigation, acquisition of data, visualization, and writing—original draft preparation. S.M.F.: Conceptualization, methodology, investigation, writing—original draft preparation, and funding acquisition.
Funding Information
Apoyo Con Carino: Patient Navigation to Improve Palliative Care for Seriously Ill Latinos” (3R01NR016467-03S1) was funded by the National Institute of Nursing Research (NINR).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.