
Abstract
Hospice and palliative medicine (HPM) educators must often give up the satisfaction of working one-on-one with patients, to allow learners the opportunity to practice key communication skills and form their own therapeutic bonds with patients. Though the loss of that primary relationship with patients may feel challenging, educators may find new opportunity for professional impact and satisfaction by investing in their relationship with learners. This case discussion explores the challenges of bedside teaching in HPM, including the educator's looser connection with patients, need to withhold their own communication skills, and decision of when to interject into a trainee–patient conversation. We then propose strategies to help educators find renewed professional fulfillment in the teacher–learner relationship. By partnering intentionally with learners before, during, and after shared visits, inviting informal reflection between encounters, and preserving independent clinical time, we believe educators may cultivate a more sustainable and meaningful clinical teaching practice.
Dr. Morgan, a palliative care attending physician two years out of training, is working on the inpatient consult service with Dr. Stuart, a palliative care fellow. They are caring for Ms. Rhodes, a 52-year-old woman with metastatic ovarian cancer who has worsening cancer-related pain and progressive disease despite multiple lines of treatment. In addition to addressing Ms. Rhodes' pain, they discuss her illness understanding and probe her hopes and worries about the future. During these conversations, fellow Dr. Stuart takes the lead, exploring Ms. Rhodes' concerns, while seated in a chair at the edge of the patient's bed.
Dr. Morgan largely observes these discussions from a perch on the room's windowsill. While tempted to jump in more often, Dr. Morgan limits her comments to an occasional clarifying question or an empathic statement at moments of high emotion. After each visit, the fellow and attending have a short debrief outside the room, reflecting on a few specific questions regarding what went well and where opportunities exist for improvement in future communication. At the end of the week, the clinicians participate in a meeting with Ms. Rhodes and her family, during which the team recommends against further cancer-directed treatments and suggests referral to an inpatient hospice facility.
Dr. Stuart ably leads the meeting, although less skillfully and efficiently than Dr. Morgan might have done herself. As the clinicians prepare to leave, Ms. Rhodes takes Dr. Stuart's hand and says, “Thank you, Dr. Stuart, you have helped me so much.” Driving home later that day, Dr. Morgan finds herself reflecting on the case; she notices a twinge of emotion when she thinks of the effort she took to provide excellent palliative care—made somewhat more complicated by simultaneously precepting Dr. Stuart—and the fact that it was Dr. Stuart who received Ms. Rhodes' gratitude. She feels both proud of her learner and also somewhat empty about her own clinical bond with the patient—can this be right?
Introduction: How Does the Presence of a Learner Change Clinical Relationships?
H
In this case discussion, we explore the challenges faced by HPM educators when seeing patients with learners and highlight the potential for renewed professional fulfillment in the teacher–learner relationship. We hope that by reflecting on the interpersonal complexities of bedside teaching, HPM educators may cultivate a more sustainable and meaningful practice.
The Teacher–Learner–Patient Triad
Clinical relationships can be framed as a dyad, a therapeutic partnership between the clinician and the patient. Two becomes three when a learner enters, infusing the clinical encounter with an educational mission (Fig. 1). Now a part of a triad, the patient often views the learner as the primary clinician, particularly in the later stages of clinical training. Concurrently, the learner and teacher often form a supportive partnership before, during, and after the patient encounter. As these two legs of the triad (learner–patient and educator–learner) strengthen, the educator–patient side may recede. In our case, Ms. Rhodes views Dr. Stuart, the HPM fellow, as her primary HPM clinician, whereas Dr. Morgan, the HPM attending, intentionally “steps back” to foster the growth of Dr. Stuart's clinical skills.
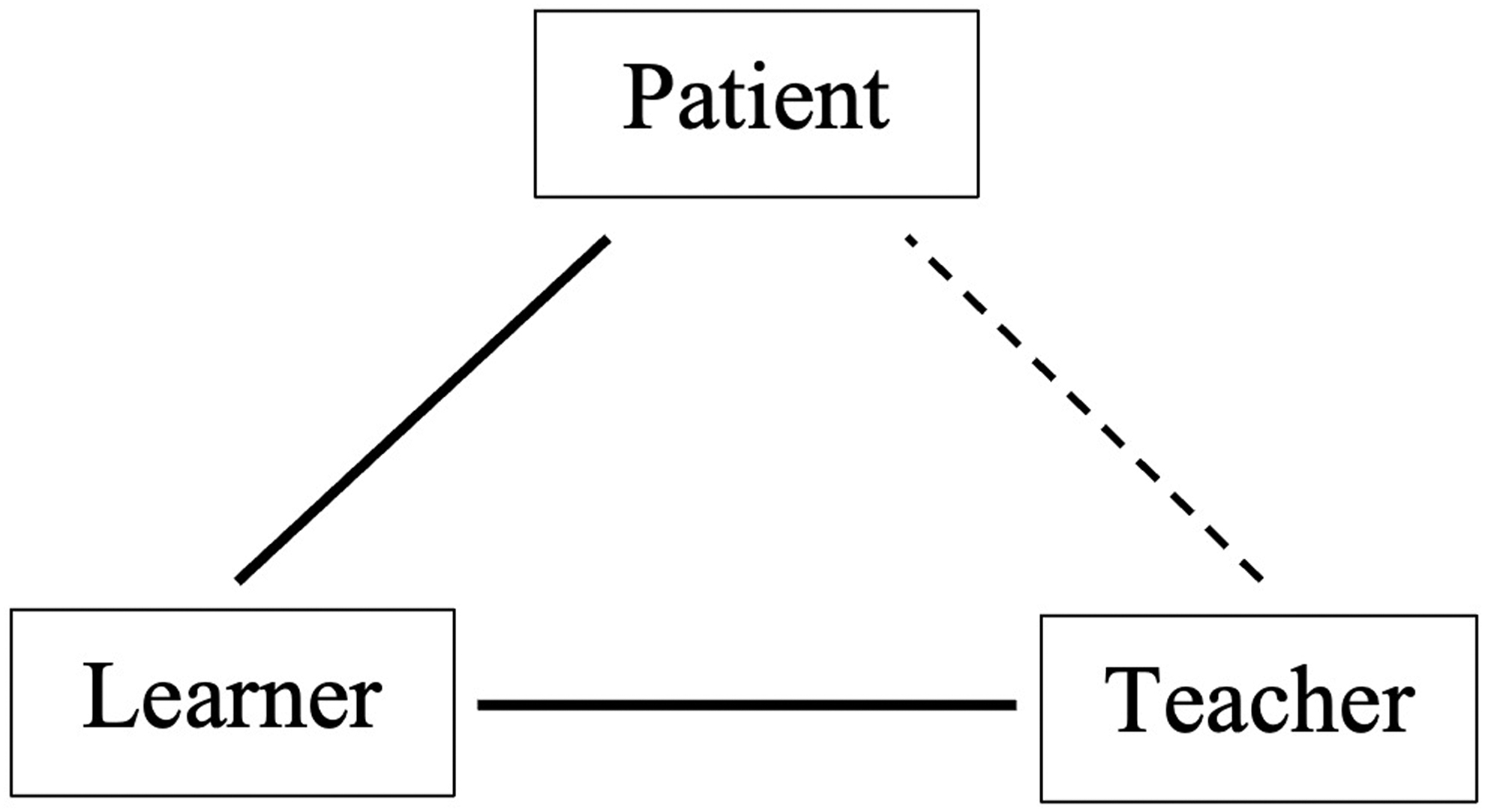
The teacher–learner–patient triad. When teachers share encounters with advanced clinical learners, the patient–learner connection is often strong, as the patient views the learner as their primary clinician. The teacher–learner connection may also be strong, as they partner in patient care and develop the learner's clinical skills. The patient–teacher connection is often less strong, as the teacher intentionally “steps back” to allow the learner space to practice important skills and develop a therapeutic bond with the patient.
Challenges of the Bedside Teaching Role for HPM Educators
Table 1 lists three challenges faced by HPM educators while navigating shared visits with learners.
Challenges of the Bedside Teaching Role for Hospice and Palliative Medicine Educators
Challenge 1: Educator senses a looser bond with the patient
Although the complexities of the teacher–learner–patient triad are seen throughout clinical teaching environments, the “loss” of the primary relationship with the patient can be particularly poignant for HPM clinicians. Many are drawn to HPM practice by the opportunity to relieve suffering and communicate effectively with patients, 1 and upon completion of fellowship training, the opportunity for meaningful clinical work remains among the most appealing aspects of the specialty. 2
In our experience, the loss, then, of that primary clinical relationship can be one of the most challenging aspects of the HPM educator role especially for those, such as Dr. Morgan, who are early in their careers. Such educators may miss the satisfaction of working one-on-one with patients and may feel uncertain about the clinical value they add, as they are now positioned—literally and figuratively—farther from the bedside.
Challenge 2: Educators must refrain from using their own skills
HPM clinicians may commonly view their ability to communicate authentically and forge a trusting relationship with the patient and family as central to their therapeutic intervention. 3 And yet, to foster skill building among their trainees, HPM educators such as Dr. Morgan must withhold some of their own expert-level communication in the service of trainee education, often sacrificing a measure of effectiveness, efficiency, or both. In our case, Dr. Stuart's growing competence as a learner requires Dr. Morgan to exert self-restraint during daily visits with Ms. Rhodes and in the family meeting.
Challenge 3: Educator must gauge when to interject
While passing the reins of communication over to the learner, HPM educators must also decide whether and when to insert themselves into the conversation and are at risk of several pitfalls in this regard. Interrupting and taking over the conversation risks deskilling the learner and hindering their therapeutic bond with the patient. 4 In our experience, early career educators, especially, may insert themselves into the patient–learner conversation prematurely, before the learner has had a chance to navigate a significant portion of the conversation, or immediately after the learner has had a misstep, not giving the learner a chance to course correct.
An educator may also jump into the conversation at a critical moment, such as during the delivery of serious news, and effectively “steal” the learner's opportunity for skill growth. Supervising clinicians must decide on a threshold for their own interjections into conversations with patients and be transparent with learners about the considerations for doing so. 4 As educators mature in their practice, we have observed that they often develop a higher tolerance for learner variation, conversational missteps, and even communication errors that require repair.
Strategies for Navigating the Challenges of the HPM Educator Role
Table 2 lists several strategies that HPM educators can use to overcome the loss of the primary relationship with the patient and navigate the challenges already described.
Strategies to Mitigate the Challenges of the Hospice and Palliative Medicine Educator Role
Strategy 1: Shift some attention from the patient to the learner
In our experience, educators can find new opportunities for relationship, connection, and professional impact by shifting some of their focus from the patient to the learner. Medical educators have described engagement with learners as an important source of professional joy, 5 and in HPM, the very skills that allow supervising clinicians to form strong bonds quickly with patients can be used similarly with learners: asking open-ended questions to identify learning needs, understanding the learner's perspective, aligning with a learner's strengths while helping with growth areas, and serving as advocate and champion to promote the learner's interests.
HPM educators such as Dr. Morgan may reflect on questions regarding the learner that parallel typical work with patients: What does the learner already understand about navigating difficult conversations? What are their goals for growing their clinical skills? How can I be most helpful? As this relationship grows and the teacher supports the learner in taking risks, tackling challenges, and growing their skills, the teacher may experience a new form of professional satisfaction and meaning—recovering, in a sense, the connection and fulfillment no longer directly experienced as the patient's sole clinician.
Strategy 2: Make a plan with the learner before shared encounters
HPM educators and trainees can discuss specific communication learning goals when starting to work together and make a plan before entering patients' rooms. Supervising clinicians can narrow the scope of potential learning and feedback from the full breadth of HPM to more manageable chunks, sketching an approach that includes specific communication tasks as well as delineating which clinician will “take the lead” in each discussion. This can support educators in refraining from jumping in too soon at a critical moment.
With advanced learners such as Dr. Stuart, the teacher can demonstrate support before the visit, while also committing to staying in the background if possible; “You're going to take the lead, and I'll be there to observe and offer support if needed. If you're feeling stuck, you can look toward me and ask me if I have anything to add. I may also step in by saying ‘May I add something?’ if I think I can be helpful.”4,6 Saying these words aloud can remind the teacher of the educational aim of allowing the learner to have the primary relationship with the patient and imply that her own focus is shifting partially from the patient to the learner.
Educators can also use physical space intentionally during the set-up of encounter to foster the patient–learner relationship, inviting the learner to sit in proximity to the patient and positioning themselves farther away, affording availability for support but remaining demonstrably “in the background.”
Strategy 3: Efficiently debrief with the learner after shared encounters
Having a systematic way of debriefing shared clinical encounters can help learners distill the visit into a few key learning points and allow educators to invest in their relationships with trainees, all while preserving efficiency within the clinical day. We recommend using the approach described by Topoll and colleagues, in which debriefing consists of three questions (How did that go? What went well? What would you have done differently?) and ends with the learner identifying one concise learning point to use in the future. 6 In our experience, this approach can foster rich yet time-efficient debriefs, which are didactic for the learner and fulfilling for the educator.
Strategy 4: Designate independent clinical time for both educators and learners
Affording opportunities for supervising clinicians and learners to have independent clinical time can often benefit both. By preserving some time for one-on-one work with patients and families, educators can experience some of the emotional connection and therapeutic relationship that they may miss when a learner is present. Similarly, encouraging learners to see patients independently during the clinical day or rotation can provide opportunity for them to stretch their skills and deepen their relationship with patients without being constantly monitored. Encouraging this autonomy often feels easier as learners gain experience and reach more advanced stages of training, as is the case for HPM fellow Dr. Stuart.
Strategy 5: Lean into informal moments with learners between encounters
Important clinical learning happens not only during shared patient encounters and postencounter debriefs, but also through less formal conversations between teachers and learners between clinical encounters. In our experience, hallway and stairwell conversations that unpack the shared experience of caring for a young dying patient or explore how we find sustainability in our practice—these are the moments that often foster the deepest connection between teacher and learner and provide clinical educators with fulfillment in their teaching practice. In our case, Dr. Morgan can stay mindful of time between encounters with Dr. Stuart, when there may be space for informal reflection and conversation that solidify learning and deepen the teacher–learner bond.
Conclusions
HPM clinician educators face a variety of challenges when working with learners, including giving up some of their own connection to the patient, refraining from using their own skills, and gauging when to interject and when not to. The strategies listed here are designed to cultivate intentionality in the preceptor–student relationship, building in moments to draw closer and reflect together along with moments to step back and operate more independently.
With this intentionality, we believe that the challenges of the clinical supervisor role start to fade compared with the rewards, especially when these precepting strategies lead to improvement in the learner's performance and a richer relationship between educator and student. We believe that uplifting learners can emerge as a new source of professional impact and satisfaction, thereby deepening our teaching and professional practice.
Author Disclosure Statement
No competing financial interests exist.