
Abstract
Background and Objective:
Opioid-induced nausea and vomiting (OINV) is known to develop not only upon opioid introduction but also during opioid dose escalation, but the actual details are unclear. The aim of this study was to investigate the frequency of OINV in opioid dose escalation at a single center and to identify risk factors.
Methods:
A retrospective analysis of the medical records of hospitalized patients with cancer who underwent increased intake of oral oxycodone extended-release tablets at Komaki City Hospital between January 2016 and December 2019 was performed. Associations between the incidence of OINV and multiple factors were analyzed, including patient demographics, opioid daily dose, comorbidities, history of nausea after opioid introduction, and prophylactic antiemetic drugs.
Results:
Of the 132 patients analyzed, 56 (42.4%; grades 1 and 2, 36 and 20, respectively) developed opioid-induced nausea after opioid dose escalation, 26 (19.7%; grades 1 and 2, 19 and 7, respectively) developed opioid-induced vomiting, 58 (43.9%) had either opioid-induced nausea or vomiting. Thirty-five of 60 patients (55.0%) developed OINV among those who received prophylactic antiemetic drugs at opioid dose escalation. Performance status (≥2) (odds ratio [OR]: 2.36, 95% confidence interval [95% CI]: 1.15–4.84, p = 0.02) and history of nausea for opioid introduction (OR: 2.92, 95% CI: 1.20–7.10, p = 0.02) were detected as risk factors for the development of OINV.
Conclusion:
This study revealed a high incidence of OINV during opioid dose escalation, indicating that careful monitoring is required as at the time of opioid introduction. Further validation by a prospective study is required.
Introduction
Opioid analgesics are widely used to relieve cancer pain, but opioid-induced nausea and vomiting (OINV) is a typical adverse effect. Approximately 60% of patients with advanced cancer who are administered opioids complain of nausea and approximately 30% complain of vomiting. 1 OINV is a highly distressing symptom that can affect oral intake, medication adherence, 2 quality of life, and activities of daily living.
The exact mechanism of OINV is not entirely clear, but it is known to involve multiple complex mechanisms, including (I) increased vestibular sensitivity, (II) direct effects on the chemoreceptor trigger zone (CTZ), and (III) delayed gastric emptying.3,4 The CTZ contains multiple receptors, such as μ-opioid receptor, dopamine D2 receptor, serotonin receptor, and neurokinin-1 receptor, and opioids activate these receptors directly or indirectly, signaling the vomiting center and causing OINV. In the mechanism of motion-induced nausea and vomiting, a conceivable mechanism entails the stimulation of μ-receptors within the vestibular apparatus, which consequently augments histamine release and activates the CTZ and the vomiting center.
Drugs that act on these receptors are used for treatment of OINV, and although there are reports that dopamine D2 receptor antagonists such as prochlorperazine and metoclopramide are not effective in preventing OINV,5,6 these drugs have been used as first-line agents for OINV to relieve nausea and vomiting. If these drugs cannot improve OINV, new antiemetic drugs such as olanzapine that target multiple receptors and may play a role in contributing to nausea and vomiting alleviation or opioid switching are recommended by national 7 and international guidelines. 8 OINV may exhibit significant interindividual variation in the frequency, severity, or development of tolerance of nausea and/or vomiting among patients; thus, nausea and vomiting effects are more difficult to fully control in the majority of patients.
OINV is not uncommon in patients starting opioid therapy, and tolerance to OINV generally tends to occur within days to one week. 9 The precise mechanisms of tolerance to OINV are incompletely understood, and OINV is also known to develop during opioid dose escalation. 7 However, the full understanding of OINV in opioid dose escalation has not been clarified. Some studies have reported on risk factors for OINV at opioid introduction,10–13 but none has examined the risk factors associated with OINV for opioid dose escalation.
The aim of this study was to retrospectively investigate the frequency of OINV for opioid dose escalation at a single center and to identify risk factors. In this study, OINV in opioid dose escalation was defined as nausea and vomiting observed within seven days after opioid dose escalation.
Materials and Methods
Study patients and design
This retrospective study recruited hospitalized patients with cancer (≥20 years old) who had increased their dose of oral oxycodone extended-release tablets at Komaki City Hospital between January 2016 and December 2019. Because differences in opioid and route of administration affect emetogenic effects, this study was limited to patients receiving oral oxycodone, the most commonly administered opioid in our hospital.
Exclusion criteria were as follows: (1) symptoms of nausea and vomiting before opioid dose escalation, (2) brain metastases suspected (or clinically confirmed), (3) hypercalcemia or hyponatremia, (4) impaired cognitive function, (5) cytotoxic anticancer drugs administered from one week before the evaluation period, and (6) head and abdomen or pelvic radiation from one week before the evaluation period. This study was performed in accordance with The Ethical Guidelines for Life Sciences and Medical Research Involving Human Subjects notified by the Japanese Government after approval by the institutional review board of the Komaki City Hospital (approval no.: 191029).
Data collection for eligible patients
Patients' characteristics were extracted from our electronic health record system, including clinical information at opioid dose escalation (age, gender, type of cancer, presence or absence of diabetes mellitus, Eastern Cooperative Oncology Group performance status [ECOG PS], daily dose of opioids, and presence or absence of antiemetic drugs), clinical laboratory data within one week of opioid dose escalation (serum creatinine, serum albumin, serum total bilirubin, aspartate aminotransferase, and alanine aminotransferase), and nausea and vomiting at opioid introduction.
The primary endpoint was the frequency of occurrence of either nausea or vomiting during opioid dose escalation, and secondary endpoints were the frequency and severity of nausea and vomiting and the risk factors for OINV during opioid dose escalation. OINV and other adverse events were investigated from the electronic medical record system and their severity was evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE) Ver. 4.0.
Statistical analyses
Multiple logistic regression analysis used the presence or absence of OINV after increased opioid dose as the dependent variable and factors affecting the OINV as independent variables and was performed using the stepwise variable reduction method for factors that resulted in p < 0.2 in the univariate analysis. Fisher's exact test was used to compare categorical variables in univariate analysis. Clinically meaningful laboratory cutoff values were used, which were established at the time of study design. Odds ratios (ORs) and 95% confidence intervals were calculated, and p < 0.05 was considered significant in all analyses.
All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). More precisely, it is a modified version of R commander designed to add statistical functions frequently used in biostatistics. All reported p-values were two sided, with a value of p < 0.05 considered statistically significant. 14
Results
Patients
This study analyzed 132 patients who met the study inclusion and exclusion criteria out of 200 patients who increased their intake of oral oxycodone extended-release tablets at our hospital during the study period. Patient characteristics are summarized in Table 1. The median age of the patients was 73 (range, 41–91) years, and 91 patients (68.9%) were male. Of the study patients, the number of patients with ECOG PS 0–1, 2, and 3 and over was 70 (53.0%), 35 (26.5%), and 27 (20.5%), respectively, with 22 cases of diabetes mellitus (16.7%).
Patient Characteristics
Data are numbers or the median (range).
Antiemetic drugs: oral metoclopramide or oral prochlorperazine.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ECOG PS, Eastern Cooperative Oncology Group performance status.
The most common cancer type was lung cancer (25 patients, 18.9%), followed by colorectal (15 patients, 11.4%), pancreatic (13 patients, 9.8%), and stomach (10 patients, 7.6%) cancer. In all patients, no emetogenic medications were initiated during the assessment period. Eighty patients (60.6%) were administered prophylactic antiemetic drugs for opioid introduction, and 60 patients (45.5%) received prophylactic antiemetic drugs at the time of opioid dose escalation, whereas 20 patients (15.2%) were administered antiemetic drugs (oral metoclopramide or oral prochlorperazine) as salvage therapy to alleviate nausea and vomiting after opioid dose escalation.
The median daily opioid dose before opioid escalation was 10 (range, 10–60) mg, with 117 patients (88.6%) escalating from 20 mg/day or less. Escalation of opioids from low doses influenced the escalation rate, with 81 patients (61.3%) experiencing 100% increase, 43 patients (32.6%) experiencing 30–50% increase, and the remaining individuals distributed as follows: 2 patients with <30% increase, 5 patients within the range of 51–99% increase, and 1 patient with an excess of 101% increase.
At opioid dose escalation, adverse events other than OINV developed in 100 patients (75.8%); the most common adverse effect was constipation in 73 patients (55.3%), and serious adverse events (Grade 3 or higher) included drowsiness in 2 patients and delirium in 2 patients.
Frequency of OINV after opioid dose escalation
Fifty-six patients (42.4%; 36 with grade 1 and 20 with grade 2) developed opioid-induced nausea after opioid dose escalation, 26 (19.7%; 19 grade 1 and 7 grade 2) developed opioid-induced vomiting, and 58 (43.9%) developed either opioid-induced nausea or vomiting (Fig. 1). The number of patients who did not develop opioid-induced nausea or vomiting after opioid introduction but who went on to develop the adverse effect after dose escalation was 40 (38.5%) of 104 patients (Fig. 2).
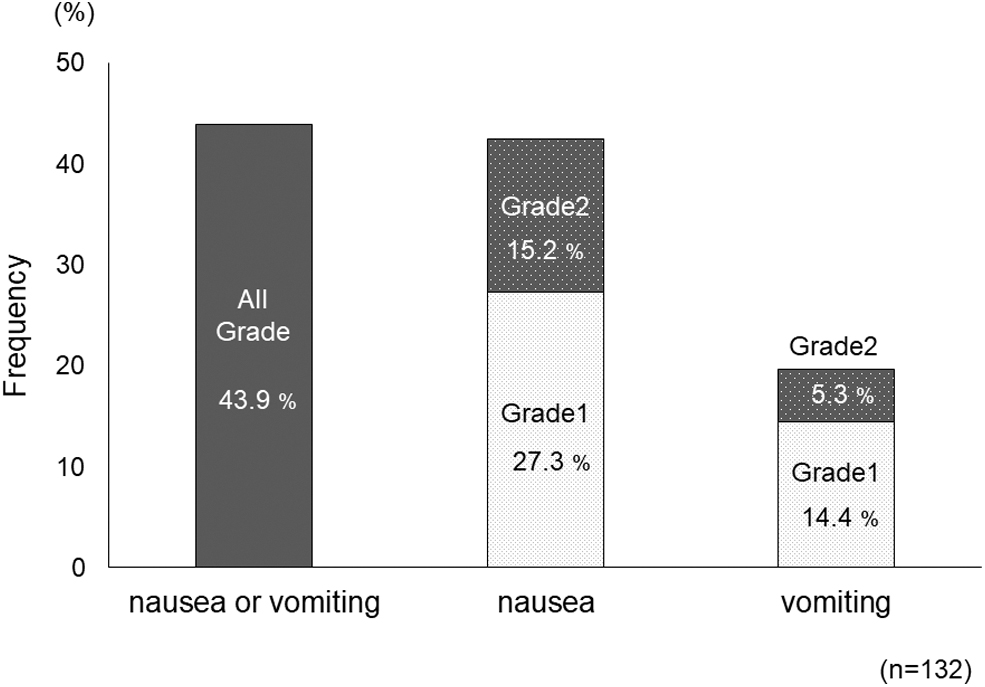
Frequency of OINV in opioid dose escalation. “Nausea or vomiting” is indicated by all grades, and “nausea” and “vomiting” are indicated by grade. OINV, opioid-induced nausea and vomiting.
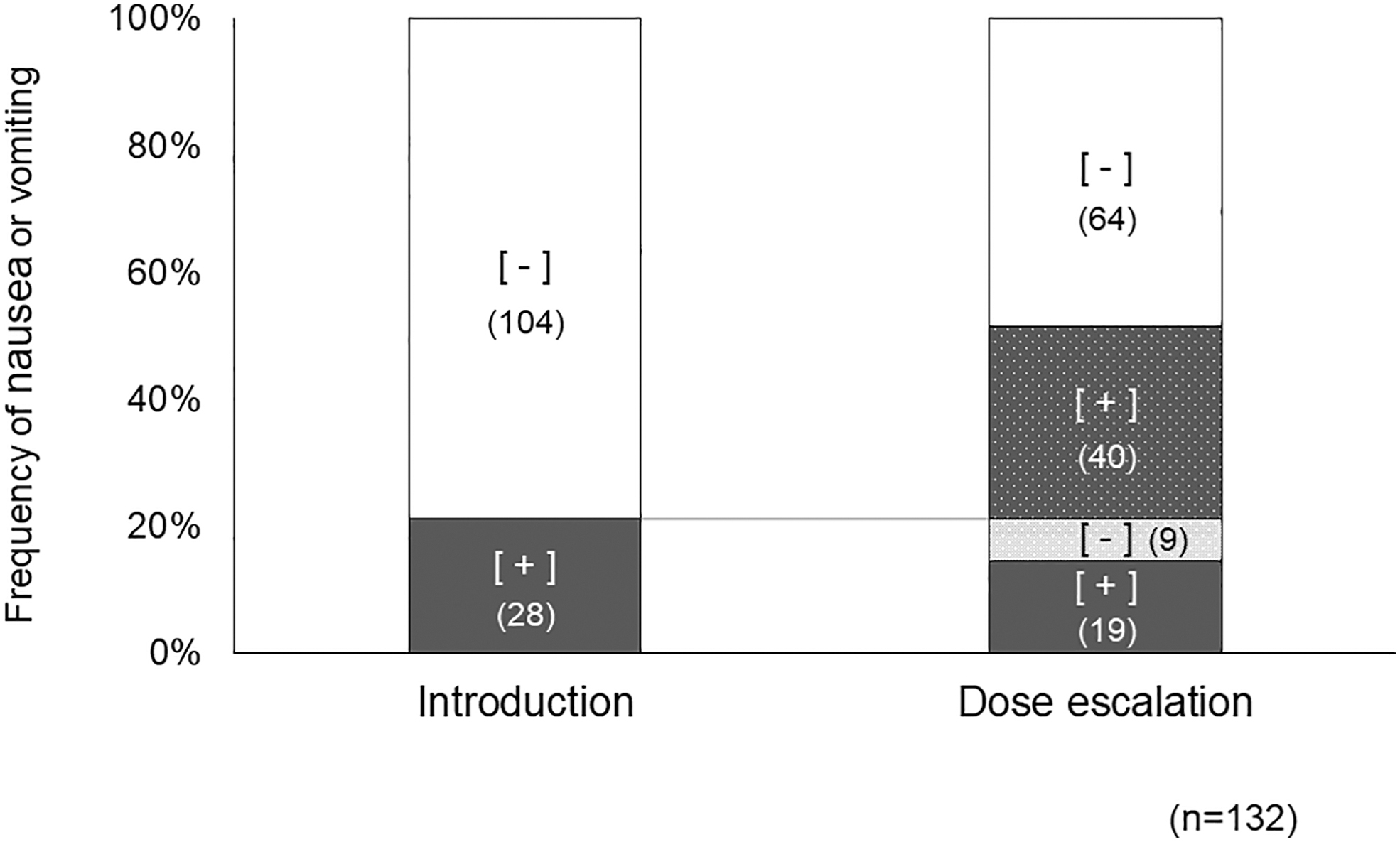
Association of OINV at opioid introduction and dose escalation. The black columns indicate OINV. This figure shows that even patients without OINV at opioid introduction may develop OINV at opioid dose escalation.
Opioid-induced nausea or vomiting occurred in 18 (64.3%) of 28 patients with both opioid introduction and opioid dose escalation, and in 35.7% (n = 10) with only opioid introduction (Fig. 2). Thirty-five of 60 patients (55.0%) developed opioid-induced nausea or vomiting among those who received prophylactic antiemetic drugs at opioid dose escalation (Fig. 3).
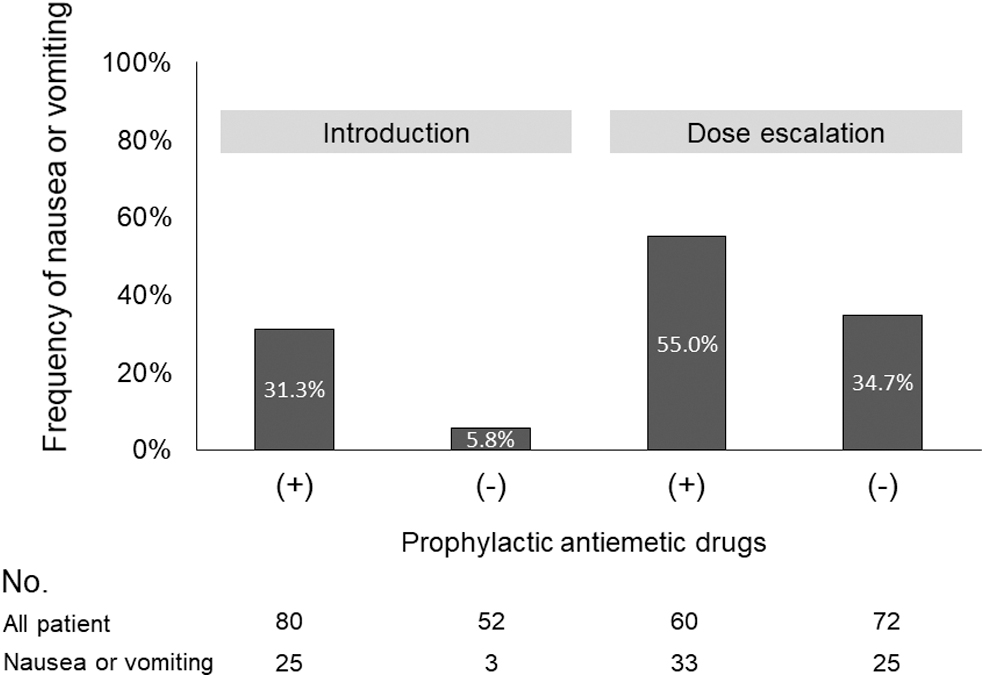
Association of OINV at opioid introduction and with/without prophylactic antiemetic drugs. This figure shows the relationship between OINV and prophylactic antiemetic drugs at opioid introduction and dose escalation. Although prophylactic antiemetic drugs were given to many patients at both opioid introduction and dose escalation, no clear benefit was demonstrated.
Risk factors for OINV during opioid dose escalation
Table 2 displays the relationship between each factor determined by univariate analysis. ECOG PS (≥2), history of OINV after opioid introduction, gastrointestinal cancer, prophylactic antiemetic drugs for opioid dose escalation, and diabetes mellitus were identified as significant risk factors of OINV after opioid dose escalation in the univariate analysis. Multivariate analysis using these parameters showed that ECOG PS (≥2) (OR: 2.36, p = 0.02) and a history of OINV after opioid introduction (OR: 2.92, p = 0.02) were independent risk factors for OINV after opioid dose escalation.
Univariate and Multivariate Analysis for Risk Factors for Opioid-Induced Nausea or Vomiting
95% CI, 95% confidence interval; OR, odds ratio.
Discussion
In this study, the incidence of OINV after opioid dose escalation was relatively high at 43.9%, of which <15% were grade 2 events, indicating that careful monitoring is required as at the time of opioid introduction. This study signifies the first investigation to suggest that increasing opioid dose affects the development of OINV though a retrospective observational analysis.
The prophylactic administration of antiemetic drugs for opioid dose escalation had no effect on preventing the occurrence of OINV in this study. Tukuura et al. conducted a double-blind randomized controlled trial to evaluate the efficacy of prophylactic antiemetic treatment with prochlorperazine for OINV and concluded that routine prophylactic administration of prochlorperazine was not beneficial because there was no difference in efficacy between the intervention and control groups; in fact, the intervention group had a higher incidence of severe somnolence and delirium. 5
We consider that this result is similar to the previous report, and indicates that routine prophylactic administration of antiemetic agents is not suitable for OINV, as recommended by national and international guidelines.7,8 However, prophylactic administration of dopamine blockers such as metoclopramide has not been completely ruled out because there have been no trials in patients at high risk of nausea and vomiting, and because prophylactic administration is allowed in patients prone to nausea in the Japanese guidelines, 7 administration may be considered on a patient-specific basis.
The antiemetic agents used in this study were oral metoclopramide and prochlorperazine, and the usefulness of prophylactic administration of antiemetic agents for multiacting receptor-targeted antipsychotics such as olanzapine is still unknown and needs to be verified.
In this study, a history of OINV after opioid introduction was confirmed to be a risk factor for OINV in opioid dose escalation. Inadequate response to past nausea is generically known to cause anticipatory nausea and vomiting owing to anxiety and other psychological factors. 15 We consider that the results of previous studies related to cancer chemotherapy-induced nausea and vomiting 16 and postoperative nausea and vomiting 17 also support the present results. Genetic involvement may also be a consideration because several potential genetic studies on postoperative nausea and vomiting have reported genes that predispose to OINV, 18 although the details are not clear. On the basis of these results, it is necessary to consider whether or not to prescribe antiemetic drugs in advance, depending on the OINV status at the time of introduction.
ECOG PS (≥2) was also a significant risk factor of OINV in opioid dose escalation in this study. Kishi et al. reported that ECOG PS 3 or higher is a risk factor for OINV and opioid-induced constipation at the time of introduction, 19 and the results of this study also confirm their report. They suspected that in patients with lowered ECOG PS, the decrease in gastrointestinal tract function due to prolonged bed rest may exacerbate constipation and nausea. It has been reported that patients with lowered ECOG PS are also vulnerable to the development of cancer chemotherapy-induced nausea and vomiting, 20 and further investigation is needed.
There are several limitations of this study, including its single-center design, small sample size, and retrospective nature. Factors such as young age and female gender, which were detected in reports10–13 of risk factors for OINV in opioid introduction, were not risk factors in this study but should be examined in the future in a prospective observational study with a larger number of patients. Second, the study was limited to hospital admissions. However, many patients also received increased doses of opioids in the outpatient setting, and it is possible that this study did not represent all cases of OINV with increased opioid doses.
Third, this study insufficiently assessed the ramifications of aggravated constipation on OINV. Although no severe constipation (grade 3) was observed in this study using the CTCAE grading scale, leaving the precise impact of constipation on OINV unidentified because constipation was not assessed using assessment tools such as the Bowel Function Index or Patient Assessment of Constipation-Symptoms (PAC-SYM) that are based on judgments of stool appearance, perceived discomfort, and ease of defecation. 21
To ascertain whether constipation acts as a predisposing factor for OINV, it is imperative to validate this hypothesis through prospective observational research that comprehensively assesses constipation, incorporating assessment tool such as bowel function index, commencing before opioid dose escalation. Fourth, this study has not successfully elucidated the correlation between OINV and the rate of escalation in opioid dosage. As 88.6% of the participants in this study received doses of 20 mg per day or less before opioid dose escalation, we posit that the participants in this study are insufficient to substantiate an association between OINV and opioid dose escalation rates.
To ameliorate this quandary, it is imperative to gather a substantial corpus of cases encompassing a diverse range of opioid daily doses. Moreover, opioid dose escalation was defined as an augmentation in the daily dosage of the extended-release formulation, whereas the utilization of fast-release formulations for managing unexpected pain episodes was not taken into account in this study.
Given the diurnal fluctuations in the utilization of fast-acting opioid preparations even among patients experiencing consistent pain symptoms, it becomes imperative to formulate a precise definition of opioid dose escalation and assessment period by means of pilot studies in future investigations. Finally, because the study was limited to patients receiving oral oxycodone, the frequency of OINV during dose escalation with other opioids remains unknown.
Conclusions
In conclusion, this study revealed that the incidence of OINV in opioid escalation, and a history of OINV during opioid introduction and ECOG PS (≥2), were significant risk factors, and we should be careful when increasing opioid doses in patients with these risk factors. We look forward to further research in this area.
Funding Information
No funding was received for this article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.