
Abstract
Background:
Black Americans experience the highest prevalence of heart failure (HF) and the worst clinical outcomes of any racial or ethnic group, but little is known about end-of-life care for this population.
Objective:
Compare treatment intensity between Black and White older adults with HF near the end of life.
Design:
Negative binomial and logistic regression analyses of pooled, cross-sectional data from the Health and Retirement Study (HRS).
Setting/Subjects:
A total of 1607 U.S. adults aged 65 years and older with HF who identify as Black or White, and whose proxy informant participated in an HRS exit interview between 2002 and 2016.
Measurements:
We compared four common measures of treatment intensity at the end of life (number of hospital admissions, receipt of care in an intensive care unit (ICU), utilization of life support, and whether the decedent died in a hospital) between Black and White HF patients, controlling for demographic, social, and health characteristics.
Results:
Racial identity was not significantly associated with the number of hospital admissions or admission to an ICU in the last 24 months of life. However, Black HF patients were more likely to spend time on life support (odds ratio [OR] = 2.16, confidence interval [CI] = 1.35–3.44, p = 0.00) and more likely to die in a hospital (OR = 1.53, CI = 1.03–2.28, p = 0.04) than White HF patients.
Conclusion:
Black HF patients were more likely to die in a hospital and to spend time on life support than White HF patients. Thoughtful and consistent engagement with HF patients regarding treatment preferences is an important step in addressing inequities.
Introduction
Currently, an estimated 6 million adults have a heart failure (HF) diagnosis in the United States, and this number is expected to increase to 8 million by 2030. 1 HF is most prevalent among older adults, with people 65 years and older constituting over 80% of HF patients. 1 Racial and ethnic minority groups are disproportionately affected by HF, with Black Americans experiencing the highest incidence and prevalence of HF and the worst clinical outcomes of any racial or ethnic group.1–3 Despite advancement in available HF treatments and gains in overall HF survival in the last two decades, racial and ethnic inequities in HF burden and mortality persist. 4
For adults with HF, the final months of life are characterized by increasing illness severity, new and worsening symptoms, greater disability, and emotional distress.5,6 HF patients often receive intensive and burdensome treatment at the end of life, including numerous hospital admissions, admission to the intensive care unit (ICU), dying in a hospital, and invasive procedures such as the insertion of implantable cardioverter defibrillators and mechanical ventilation with little hope of survival.7,8 Such treatment persists despite research suggesting that HF patients largely prefer symptom relief over longer survival time. 9
Given the large physical and psychological burden of end-stage HF, treatment guidelines from the American College of Cardiology emphasize involvement of a palliative care team 10 ; however, palliative care utilization for HF patients remains low when compared with other disease categories such as cancer. 11 Contributing factors include a lack of consensus regarding palliative care referral criteria for HF patients, an unpredictable disease trajectory, limited patient and provider knowledge about palliative care, lower rates of advance care planning, and variable access to specialty palliative care.11–14
Disparities in end-of-life care are often exacerbated among minoritized groups. Non-White patients, particularly Black patients, are less likely than White patients to receive palliative care and more likely to experience intensive treatment at the end of life.15–18 These disparities are consistent across multiple disease conditions. Research focused specifically on HF patients has identified racial and ethnic disparities in hospice admissions19,20 and inpatient palliative care consultations21,22; however, little is known about racial inequities in treatment intensity at the end of life among HF patients specifically. This study contributes to the literature by using data from the nationally representative Health and Retirement Study (HRS)23,24 to examine differences in inpatient treatment intensity at the end of life between deceased non-Hispanic Black and non-Hispanic White HF patients.
Methods
Data source
The HRS is a longitudinal survey of American adults 51 years of age and older sponsored by the National Institute on Aging (grant number NIA U01AG009740) and conducted by the University of Michigan. The survey provides insight into health and economic circumstances associated with aging at individual and population levels. 25 Sampled individuals have been interviewed biannually since 1992, with new cohorts added over time to maintain the nationally representative nature of the survey. After a respondent dies, the HRS conducts an exit interview with a knowledgeable proxy reporter, typically a surviving spouse or adult child, to obtain information about the respondent, including end of life experiences and circumstances of death. 26
Sample
We examined deceased HRS participants ages 65 years and older with HF whose proxy informant participated in an exit interview between 2002 and 2016 (n = 2333). Advance directive data became available beginning in 2002, thus we excluded previous years from our analysis. We excluded 182 subjects who did not identify as either non-Hispanic White or non-Hispanic Black. Additionally, we excluded 7 subjects who were uninsured as this category was too small for meaningful analysis, and 537 subjects with missing data. 27 Our final analytic sample included 1607 older adults with HF.
We created a subsample of HF patients with at least one hospital admission in the last two years of life to ensure a more homogenous population for analysis of hospital-based care (n = 1242).
Measures
Outcome variables
We constructed four outcome variables based on proxy response to HRS exit interview questions regarding treatment intensity in the last 24 months of life, including: (1) number of hospital admissions; (2) receipt of care in an ICU (yes or no); (3) utilization of life support (yes or no); and (4) whether the decedent died in a hospital (yes or no).
Primary independent variable
Racial identity was our primary predictor of interest, including non-Hispanic Black and non-Hispanic White (reference category).
Covariates
We controlled for eight demographic, social, and health characteristics. Insurance status, a proxy for health care access and socioeconomic status, 28 was constructed as Medicare and private insurance (reference category), Medicare and Medicaid (dual-enrolled), and Medicare-only. Religiosity represents a potential factor in end-of-life decision-making, with studies suggesting that more religious individuals are less likely to engage in advance care planning and more likely to desire aggressive medical intervention at the end of life. 29 In this study, religiosity was constructed as religious (attended religious services in the last 24 months of life), and not religious (did not attend religious services in the last 24 months of life). Additional covariates included decedent sex (female or male), age at death, marital status (unmarried [including divorced, widowed, and never married] or married), educational attainment (less than high school, high school graduate, college, and above), number of comorbidities, and presence of an advance directive (yes or no).
Analyses
Descriptive statistics were used to characterize our study sample. We used negative binomial regression to identify factors associated with the number of hospital admissions in the full sample. Logistic regression models were used in the subsample to examine factors associated with ICU admissions, utilization of life support, and dying in a hospital. For ease of interpreting model results, we used the margins command to calculate predicted probabilities.
Respondent-level sampling weights in the HRS survey wave before death ensured that results were representative of the U.S. older adult population. 30 Analyses were performed using Stata version 17. This study was approved by the Institutional Review Board at the University of California, Los Angeles.
Results
Decedent demographics are described in Table 1. The majority of our sample was White, female, and on average 83 years old at time of death.
Characteristics of Patients with Heart Failure Diagnosis Age 65 Years and Older, Health and Retirement Study Exit Interviews 2002–2016
HF, heart failure; HS, high school; ICU, intensive care unit; SD, standard deviation.
In adjusted analyses, racial identity was not significantly associated with the number of hospital admissions or admission to the ICU in the last 24 months of life (Table 2). However, Black HF patients were more likely to spend time on life support (odds ratio [OR] = 2.16, confidence interval [CI] = 1.35–3.44, p = 0.00) and more likely to die in a hospital (OR = 1.53, CI = 1.03–2.28, p = 0.04) than White HF patients. Black HF patients had a 41% predicted probability of spending time on life support and a 42% predicted probability of dying in a hospital, compared with 26% and 32% for White HF patients respectively (Fig. 1).
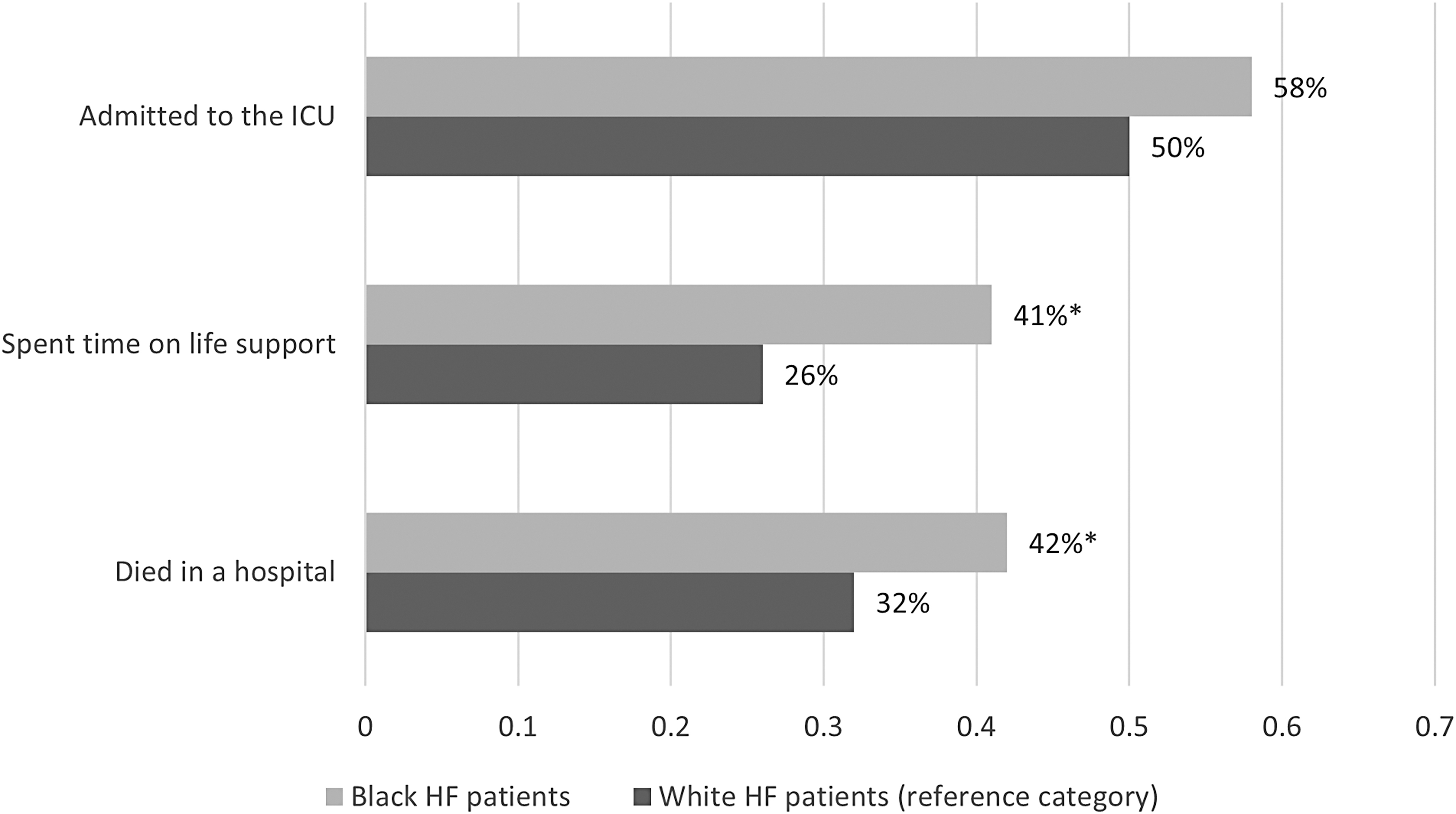
Predicted probabilities of treatment intensity by racial identity. Source: Authors' analyses of HRS exit interview data from 2002 to 2016 for respondents 65 years and older with HF. *p < 0.05. HF, heart failure; HRS, Health and Retirement Study; ICU, intensive care unit.
Association of Patient Characteristics with Treatment Intensity in the Last 24 Months of Life
p < 0.05.
CI, confidence interval; OR, odds ratio.
Other factors associated with treatment intensity included (1) age (i.e., older decedents were less likely to be admitted to the ICU, spend time on life support, or die in a hospital compared with younger patients); (2) insurance status (i.e., dual-enrolled decedents were less likely to be admitted to the ICU than Medicare and private insurance); and (3) education (i.e., decedents who attended college or above were more likely to spend time on life support than those without a high school degree) (Table 2).
Discussion
In this study of adults with HF from a nationally representative sample of Americans ages 65 years and older, we found that Black HF patients were more likely to die in a hospital and more likely to spend time on life support in the last months of life when compared with White HF patients. Our findings highlight racial differences in health care utilization patterns near the end of life among HF patients and have implications for better supporting HF patients across the disease trajectory.
The racial differences in treatment intensity observed in our sample are in line with extensive literature indicating that racially minoritized groups across disease categories are more likely to receive high intensity care at the end of life, particularly Black Americans.16–18,31 However, to our knowledge, our study is among the first to examine racial differences in treatment intensity in the context of HF specifically. Given the growing number of adults with HF and the increased burden and mortality experienced by HF patients from minoritized groups, understanding the health care utilization patterns of people with HF and how these patterns might differ by race and ethnicity is of high clinical relevance.1–3
Several factors may explain the differences in treatment intensity observed in our sample. First, patient preferences for care likely play a substantial role in medical treatment received near the end of life. 32 Prior research indicates that White older adults frequently express a preference against intensive medical care at the end of life and a desire to die at home rather than in a hospital,33,34 while Black older adults are more likely to express a preference for life-sustaining interventions over palliative care.35,36 Death and dying are highly charged personal topics, and differences in patient preferences for care in the terminal stages of life do not automatically indicate disparity. 37 Factors such as cultural values, individual preferences, religious beliefs, and differing ideas around what constitutes high quality of life may influence treatment choices. 38 Thus, racial differences in treatment intensity may not necessarily warrant intervention, but only if end-of-life decision-making is informed by collaborative and culturally relevant communication with clinicians about treatment options.
The presence of a written advance directive provides some evidence that proactive conversations about end-of-life care preferences may have occurred. In HF specifically, research shows that advance care planning improves quality of life, patient satisfaction with end-of-life care, and the quality of end-of-life communication; however, advance care planning and goals of care discussions between HF patients and clinicians are often limited and initiated late in the course of the disease.14,39 This is compounded for minoritized groups, who have significantly lower rates of advance directive completion when compared with White populations.40,41 These differences highlight an opportunity for better routinization of goals of care conversations into HF treatment. As suggested in prior work, clinicians should consider speaking with HF patients about their end-of-life care options early in the course of the disease; clear guidelines for advance care planning initiation in HF and efforts to integrate these guidelines more fully into clinical practice may be useful. 14 However, there are myriad reasons Black patients in particular might be less likely to engage in advance care planning, such as poor clinician communication, religious and spiritual beliefs, or family relationships. 38 Some evidence even suggests negative ramifications, such as increased emotional distress, when Black patients do engage in advance care planning. 42 This points to a continued need for culturally relevant, person-centered interventions throughout the care trajectory. 43
Finally, underlying all of these explanations for the differences observed in our sample is the potential influence of racism and discrimination. Previous work has demonstrated that race and ethnicity are correlated with end-of-life treatment intensity independent of other social determinants of health, and that structural racism endured throughout the life course has substantial negative consequences for health.15,44 A complex history of medical racism in the United States, coupled with racial inequities in access to health care and negative personal experiences within the health care system, may influence decision-making, trust in health care providers, and communication at the end of life. 45 While personal preferences resulting from informed decision-making should be respected, differences in end-of-life care resulting from discrimination, poor communication, or mistrust must be addressed. Our study was not designed to determine whether racism, bias, or discrimination contributed to our findings; however, the existence of treatment intensity differences in our sample supports continued efforts to identify and intervene on racism in the health care system.
This study has several limitations. First, due to small sample sizes in the HRS Exit Interview data, we were unable to examine additional racial and ethnic groups beyond non-Hispanic Black and non-Hispanic White. Hispanic/Latinx and Chinese American populations in particular are at high risk of developing HF and experience persistent inequities in health care access and quality throughout the life course. 1 The ongoing issue of study recruitment for minority groups requires urgent attention as inequities grow in HF epidemiology, clinical severity, and access to care at the end of life. Second, while the HRS Exit Interviews attempt to capture the end-of-life experience of patients, proxy respondents are often interviewed one to three years after a decedent's death and asked to consider the decedent's last two years of life. This broad timeframe may not represent a precise measurement of the end of life and may introduce recall bias. Nevertheless, we were able to identify racial differences in treatment intensity and these findings are likely magnified closer to the time of death. Third, we did not include decedent year of death or geographical information, such as region, state, or rural versus urban. These factors are likely to inform patterns of care access and utilization near the end of life. Finally, although we control for a wide range of factors associated with treatment intensity at the end of life, secondary data analysis of these topics limits the inclusion of other important determinants of end-of-life care. Relevant unobserved measures in our study include information on patient or family preferences for care, whether the treatment received was concordant with preferences, or direct narrative experiences of study participants. Future research should proactively engage with minoritized communities to gain a better understanding of their needs, perspectives, and experiences with end-of-life issues.
Conclusion
As the number of U.S. older adults with HF continues to increase, particularly among minoritized groups, careful consideration of racial and ethnic differences in health care utilization is warranted. Our results suggest that Black HF patients experience higher treatment intensity near the end of life when compared with White patients. While care received at the end of life is influenced by a complex range of factors, thoughtful and consistent engagement with HF patients about treatment preferences and goals of care is an important step in addressing racial and ethnic inequities.
Footnotes
Acknowledgments
Funding Information
This research was supported by the NIH/National Center for Advancing Translational Science (NCATS) UCLA CTSI Grant Numbers 5TL1TR000121-05 and 1TL1TR001883-01. Research was made possible by data from the HRS, sponsored by the National Institute on Aging (grant number NIA U01AG009740) and conducted by the University of Michigan.
Author Disclosure Statement
No competing financial interests exist.