
Abstract
Background:
Many older adults with advanced heart failure receive home health rehabilitation after hospitalization. Yet, integration of palliative care skills into rehabilitation is limited.
Objective:
Describe using the Multiphase Optimization Strategy (MOST) framework with human-centered design principles to engage clinical partners in the Preparation phase of palliative physical therapy intervention development.
Design:
We convened a home-based physical therapy advisory team (four clinicians, three clinical leaders) to identify physical therapist needs and preferences for incorporating palliative care skills in rehabilitation and design an intervention prototype.
Results:
Between 2022 and 2023, we held five advisory team meetings. Initial feedback on palliative care skill preferences and training needs directly informed refinement of our conceptual model and skills in the intervention prototype. Later feedback focused on reviewing and revising intervention content, delivery strategy, and training considerations.
Conclusion:
Incorporating human-centered design principles within the MOST provided a useful framework to partner with clinical colleagues in intervention design.
Introduction
Heart failure (HF) is the leading cause of acute hospitalization for older adults in the United States 1 which results in significant psychological and physical symptom burden and functional impairment.2,3 As a result, one-third of older adults receive postacute home health services4,5; physical therapy is prescribed to address functional limitations, optimize safety, and train care partners to support patient's needs in the home environment.
One-quarter of older adults hospitalized with HF die within six months of discharge, regardless of HF stage or phenotype. 5 Palliative care, which alleviates the symptoms and stress of advanced illness to improve quality of life, is highly recommended although underutilized.6–9 Despite the dual needs of the advanced HF population for both rehabilitation and palliation, in the United States, the two treatments are rarely combined and clinicians caring for individuals with HF often lack structured training in palliative care skills. 6 Thus, this population is in need of efforts to rigorously develop and test rehabilitation interventions with integrated palliative care skills.
We propose that integrating palliative care skills within home-based physical therapy received by older adults after hospitalization for advanced HF may represent one pragmatic strategy to address the unmet need for palliative care in this population. The Multiphase Optimization Strategy (MOST) 10 framework was recently recommended to systematically develop and test multicomponent palliative care interventions. 11 In this brief report, we describe how we used the MOST Preparation phase to engage clinical partners in intervention design to create LiveWell-HF, a multicomponent intervention that integrates palliative care skills from Early Integrated Palliative Care12–16 into home-based physical therapy.
Methods
MOST preparation phase and human-centered design
The MOST is an engineering informed framework for complex intervention development to produce efficient, effective, and scalable interventions 10 that complements the NIH Stage Model 17 and UK Medical Research Council Framework. 18 There are three phases—Preparation (intervention development), Optimization (intervention component refinement), and Evaluation (efficacy and effectiveness clinical trials; Fig. 1). The Preparation phase includes developing a strong conceptual model, determining stakeholder objectives for optimizing the intervention, creating evidence-based intervention components, and pilot testing to improve feasibility, acceptability, and usability. 10 Recognizing a growing need to engage stakeholders from the outset of intervention development to enhance future implementation, O'Hara et al. proposed Discover, Design & Build, and Test (DDBT), a structured process to incorporate human-centered design principles in the MOST Preparation phase. 19 Below we describe how we used DDBT principles to systematically engage clinical partners within the Preparation phase of LiveWell-HF design to ensure that palliative care skills chosen for the intervention were relevant to and aligned with home-based physical therapist practice. Future reports will describe implementation of the Optimization and Evaluation phases of MOST.
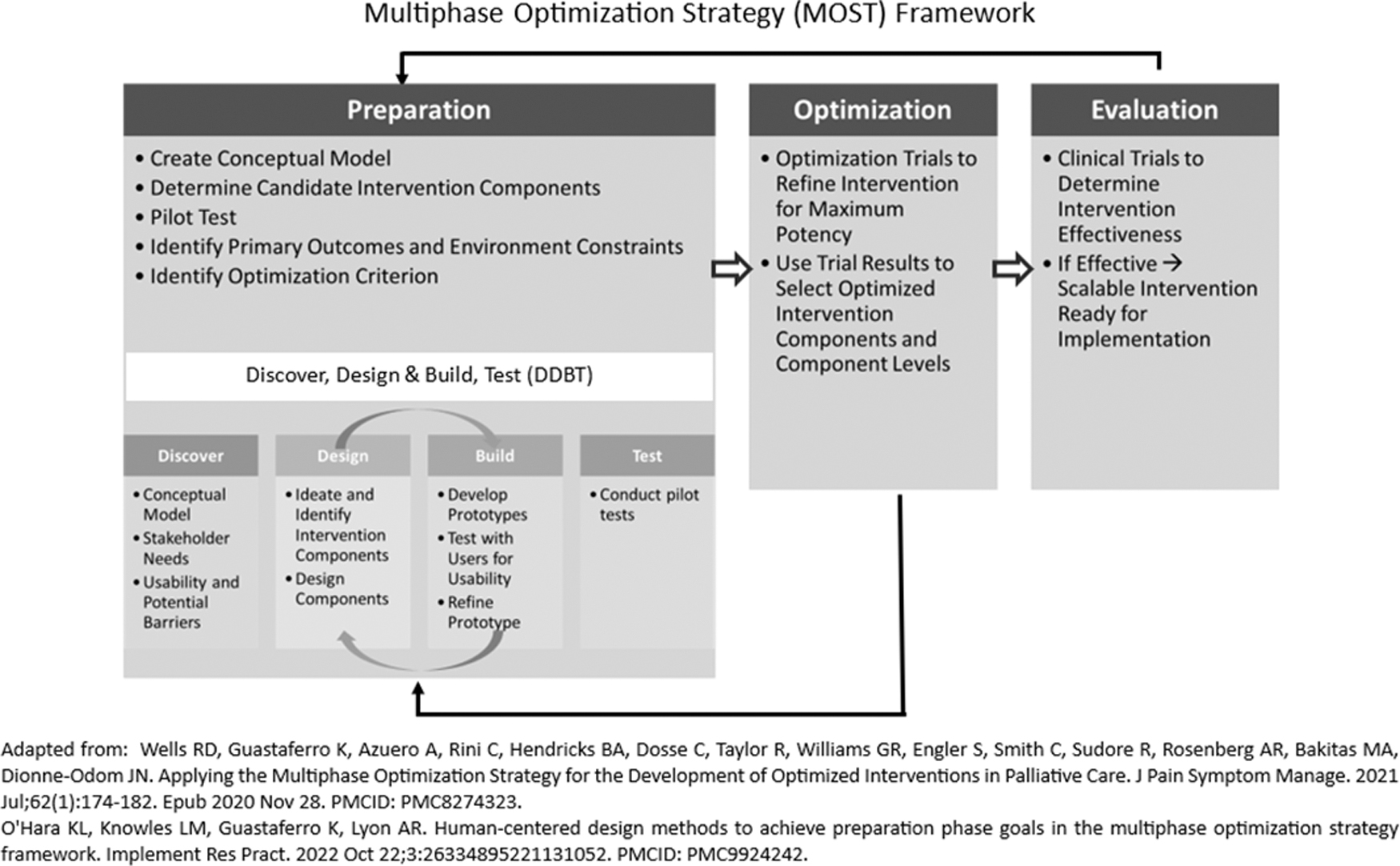
An overview of the MOST framework and DDBT human centered design principles to supplement the MOST preparation phase. DDBT, Discover, Design & Build, and Test; MOST, Multiphase Optimization Strategy.
Engaging clinical partners
Our research team partnered with Mass General Brigham Home Care (MGB Home Care), our affiliated home health agency and one of the largest nonprofit home health agencies in New England. We reviewed our project goals with MGB Home Care leadership to ensure alignment with system priorities and identified physical therapists and clinical leaders to participate in this work. Our advisory team consisted of four front-line physical therapists and three clinical leaders—a Regional Director of Physical Therapy, Learning and Professional Development Specialist, and Quality and Compliance Specialist.
DDBT “Discover” and “Design & Build” activities
Our Discover phase focused on the conceptual model, environmental context, physical therapist needs and preferences, and essential design considerations (Fig. 2). Our interdisciplinary research team with expertise in palliative care, rehabilitation, and intervention development began developing the LiveWell-HF conceptual model by conducting a scoping review of the palliative rehabilitation, HF rehabilitation, and Early Integrated Palliative Care literature, consistent with MOST and DDBT methodology (Fig. 3a). The synergy between rehabilitation interventions and palliative care were well recognized in advanced cancer20–22 and other chronic conditions, including HF.23,24 However, this synergy primarily focused on collaborative care models22,25 rather than enhancing established models of rehabilitative care with palliative care skills tailored to fit within rehabilitation delivery. Therefore, our model focused on supplementing usual home-based physical therapy with coping skill domains developed and tested in Early Integrated Palliative Care, which we hypothesize will decrease emotional distress and symptom impact, improve coping and self-efficacy, and ultimately optimize quality of life, consistent with prior research (Supplementary Table S1).12–16 To ground the conceptual model into the day-to-day operations of home-based physical therapy, the principal investigator (TK) observed sessions with two home health therapists to learn about the context and constraints of providing home-based physical therapy. We then conducted Discover advisory team meetings to solicit feedback on our conceptual model and coping skill domains, which we used to refine the model and develop a LiveWell-HF prototype. Our Design & Build advisory team meetings focused on reviewing the revised model and prototype.
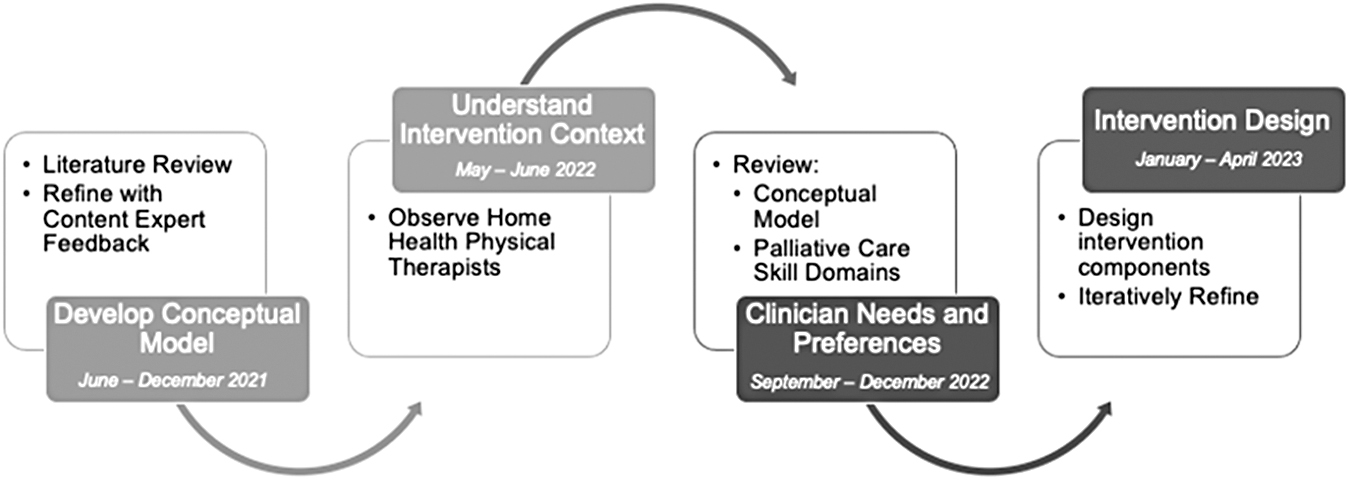
Discover and design and build activities used in the preparation phase of LiveWell-HF prototype development. Hf, heart failure.

Data sources and analysis
The principal investigator (T.K.) and study staff (S.S., A.T.) led Discover and Design & Build meetings. Meeting agendas used DDBT principles and components of the Heuristic Evaluation Rubric for Evidence-Based Psychosocial Interventions 26 to elicit feedback to inform intervention development (Supplementary Table S2). Advisory team meetings were not recorded. Rather, we used and applied rapid qualitative analysis27,28 to code de-identified data from agenda templates into a matrix to reduce data and identify themes important to LiveWell-HF prototype development. This study received exempt approval from our Institutional Review Board.
Results
We held 5, 60-minute meetings—2 in Discover phase (n = 7) and 3 in Design & Build phase (n = 4–6).
DDBT “Discover” phase feedback
Discover meetings reviewed the conceptual model and proposed palliative care coping skill domains (detailed in Supplementary Table S1). The model and coping skill domains resonated with advisory team members, who endorsed that skills were “things we are already doing, but not well operationalized or standardized.” The team thought a domain-based format would be feasible to implement (Table 1) and identified that including caregivers, when possible, would optimize engagement. While emotional and existential skills were thought to be important, the team worried about skill complexity and recommended that a simpler, standardized intervention framework with scripts would be needed to successfully train therapists. Some team members had participated in serious illness communication (SIC) training and recommended using a SIC skill framework instead of the existential domain content, given similarities in proposed content. We used feedback to simplify our conceptual model to focus explicitly on three palliative care skill modules—behavioral coping skills, symptom management, and SIC to cultivate function-directed prognostic awareness (Fig. 3b). 29 We then developed LiveWell-HF prototype materials with standardized skills (Supplementary Fig. S1) to review in Design & Build phase meetings.
Key Themes from LiveWell-Heart Failure Advisory Team Feedback in Discover Phase
HF, heart failure; SIC, serious illness communication.
DDBT “Design & Build” phase feedback
Design & Build meetings reviewed session-by-session content that included LiveWell-HF module skill scripts, proposed workflow integration, symptom assessment tools, and an adapted SIC guide (Table 2). The advisory team endorsed that the simplified LiveWell-HF modular-based skills would be more realistic to implement in clinical practice and that standardized module skills and scripts target questions commonly encountered by physical therapists. When reviewing session content and workflow, the team liked the simplified module skills, but worried that care interruptions (e.g., hospitalization) could impact session timing and completion. These concerns reinforced our optimization objective, which focuses on ensuring flexibility of session timing and delivery to meet the competing demands of the home care environment. Overall, team members felt that the prototype was of high quality and would add value to rehabilitation for older adults with advanced HF.
Key Themes from LiveWell-Heart Failure Advisory Team Feedback in Design and Build Phase
Discussion
This study is the first to describe the use of DDBT principles within the MOST Preparation phase to rigorously develop LiveWell-HF, a multicomponent home-based physical therapy intervention that integrates modularized palliative care skills into usual care. Incorporating human-centered design principles in our intervention development approach enabled us to meaningfully engage clinical advisors to ensure that LiveWell-HF aligns with physical therapist practice and meets the unique needs of home-based care.
While the benefits of collaboration between rehabilitation care and palliative care are widely noted in oncology, rigorous development and testing of palliative-informed rehabilitation interventions in the United States is nascent. Promising trials of tailored palliative rehabilitation models for patients with advanced cancers by Bayly and Nottelmann have demonstrated feasibility of intervention delivery 30 and positive impacts on quality of life,31,32 respectively. Yet research on palliative rehabilitation in HF or settings other than outpatient clinics is lacking. This is an important gap in the literature, as many older adults living with advanced HF experience distress over loss of function33–35 and frustration with lack of personalized recommendations or approaches to adapt exercise and activity late in the disease course. 35 Additionally, many articles using MOST lack clear description of Preparation phase activities 36 and structured approaches to incorporate stakeholder input within the MOST framework are limited. 37 We expand on prior work by articulating how we incorporated DDBT principles in the Preparation phase of LiveWell-HF development to engage physical therapists in intervention design. In doing so, we anticipate that we enhanced the efficiency of our design process while setting the stage for future optimization trials. As our Preparation phase advances, our team is refining our prototype with a broader set of clinicians and patients and conducting a pilot feasibility trial. We plan to use MOST Optimization phase trial designs to further refine LiveWell-HF into its most potent form followed by MOST Evaluation phase efficacy testing using a randomized control trial.
Conclusion
Using DDBT principles within the MOST Preparation phase provided a systematic approach to partner with clinicians to integrate palliative care skills into a new home-based physical therapy intervention for older adults with advanced HF.
Footnotes
Acknowledgments
Our team would like to express our gratitude to our colleagues at MGB Home Care for their partnership in this work: Judy Flynn, Octavia Moniz, Robin Beaulieu, Robin White, Lisa Moran, and Shannon Roldan.
Authors' Contributions
Dr. T.K. conceptualized the study, led data curation and analysis, drafted the original article, and approved the final version of the article. Dr. C.W. and Ms. A.S. helped to identify and recruit Advisory Team members, reviewed the original article, and approved the final version. Ms. S.S. and Ms. A.T. assisted with data curation and analysis and approved the final version of the article. Dr. A-.M.V., Dr. K.S., and Dr. J.G. provided critical feedback on the original article and approved the final version. Dr. A.M.P. and Dr. C.R. assisted with conceptualization of the study, supervised data curation and analysis, provided critical feedback on the original article, and approved the final version.
Funding Information
This work was supported in part by a Kornfeld Scholar Grant from the National Palliative Care Research Center (Dr. T.K.) and a grant from the National Institute on Aging (P30AG028716; Dr. A.M.P.).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.