
Abstract
Background:
Access to supportive services in community-based oncology is challenging but essential, particularly for underserved populations.
Methods:
We developed the Supportive Oncology Collaborative (SOC), built upon the tenets of Collaborative Care, an existing model used to increase access to behavioral health in community settings. Using a population-health-based approach with screening, a registry, and shared care, we added palliative care specialists to a team of social workers and a consulting psychiatrist. We provided integrated psychosocial and palliative care at community-based sites of a large comprehensive cancer center.
Results:
We implemented the model in 2020 at a community site with a racially and ethnically diverse patient population. Encounters grew from 527 in our first year to 2,130 in 2022. Using screening tools, we identify the highest-risk patients for discussion in team meetings.
Discussion:
We are expanding the SOC across the Dana-Farber Cancer Institute regional campuses and believe it can increase access to integrated psychosocial and palliative care in cancer centers across the country.
Introduction
Palliative care provided concurrently with oncology care significantly improves mood, alleviates symptoms, and enhances quality of life. 1 As a result, multiple organizations recommend the integration of palliative care with standard oncologic care for patients with metastatic cancer.2–4 Unfortunately, access to palliative care is limited in many communities, especially for historically marginalized populations and those with mental health concerns.5–9 In addition, the delivery of palliative care is not standardized for individuals with serious mental illness, who are at risk of premature mortality. 10 Achieving universal access to palliative care for the population with coexisting mental illness remains an unmet goal.
Behavioral health clinicians face similar challenges in access. As a result, population-based approaches, such as Collaborative Care, were developed to improve access to behavioral health clinicians. Collaborative Care was originally designed to integrate mental health care into primary care and has proven effective for expanding behavioral health services with a limited workforce. It demonstrates positive outcomes across diverse patient populations.11–13 Unfortunately, palliative care and psychosocial services in cancer centers are usually delivered through traditional referral-based models rather than through Collaborative Care models.
Although models have been proposed to address the lack of integrated mental health and palliative care services in community settings, there are challenges in operationalizing and implementing these models into practice.14–15 The Supportive Oncology Collaborative (SOC) at the Dana-Farber Cancer Institute (DFCI) regional campuses is an example of implementation at a DFCI campus that serves the towns of Lawrence and Haverhill, both listed as high-poverty sites in the state of Massachusetts. 16 Before the program’s implementation, patients at regional campuses requiring specialty consultations in psychiatry, psychology, or palliative care were referred to metro Boston. This process significantly limited access due to constraints in transportation, staffing limitations, and the reliance on a referral-based system. We outline key components of the SOC at the DFCI Merrimack Valley regional campus and discuss how it adheres to the four tenets of Collaborative Care: (1) an interdisciplinary team with a care manager or primary clinician; (2) population health using a registry; (3) measurement-based care and treating patients to specific targets; (4) weekly team meetings with the consulting psychiatrist and palliative care physician. 17
Methods
The SOC is an interdisciplinary, team-based model aimed at providing patient-centered palliative and psychosocial care across the DFCI network of regional campuses. It bridges the gap between the high volume of oncology patients needing supportive services at community-based sites and the limited availability of behavioral health and palliative care clinicians. This model has been developed in collaboration with the Dana-Farber Patient and Family Advisory Committee. Initially implemented in 2020 at the DFCI Merrimack Valley campus, the SOC consists of two full-time equivalents (FTEs) of community-based, on-site oncology social workers, and 0.5 FTE palliative care advanced practice practitioner (APP) who conduct weekly case reviews and collaborate with a psychiatrist, psychologist, and palliative care physician virtually (approximately 0.1 FTE each; Fig. 1).
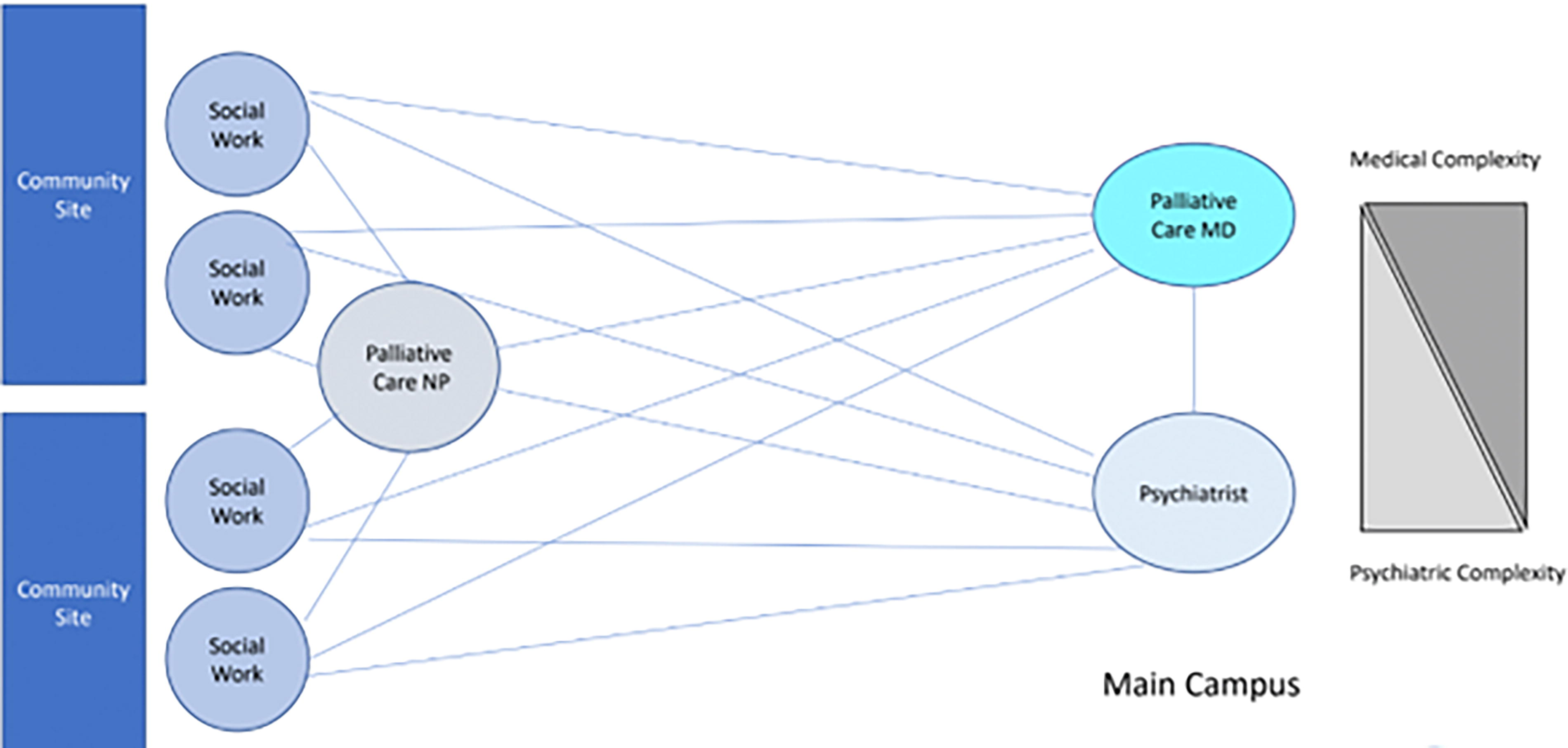
Clinical structure of the Supportive Oncology Collaborative. NP, Nurse Practitioner; MD, Medical Doctor;MOLST, Medical Orders for Life Sustaining Treatment; POLST, Physician Orders for Life Sustaining Treatment.
Patients are referred to the SOC by their oncology teams or by universal screening for distress which includes the Patient Health Questionnaire-4 (PHQ-4), Patient-Reported Outcomes Measurement Information System (PROMIS-10), Tobacco, Alcohol, Prescriptions Medication and Other Substance (TAPS) tool along with questions regarding resource needs and impact of illness and symptoms.18–20 Upon being screened in for, or referred to, the SOC, patient names are added to a registry and the patient undergoes a comprehensive psychosocial assessment by a social worker.
A reason for referral to the SOC is identified either by the referring clinician or by the social worker at the time of assessment and interventions are based on the reason for referral. Common reasons for referral include pain management, non-pain symptom management, coping, depression/anxiety, serious mental illness, goals of care, end-of-life, and early palliative care. The social worker serves as the primary clinician and assesses all patients, regardless of the reason for referral. If the patient is referred for a reason that requires additional palliative expertise, they are also seen by the palliative care APP. Together, the social worker and APP form an initial treatment plan, which is presented at a weekly interdisciplinary team meeting attended by the remote psychologist, psychiatrist, and palliative care physician. The team discusses the patient and may augment or modify the initial treatment plan, such as making recommendations for evidence-based behavioral interventions, adjusting psychiatric medications, or suggesting a more intensive pain regimen. If, after team discussion, additional supports are deemed necessary, the patient is referred for an in-person or virtual visit with a psychologist, psychiatrist, or palliative care physician on the Boston DFCI campus. An example of how care might be delivered to a patient with metastatic cancer referred for pain is illustrated in Figure 2.
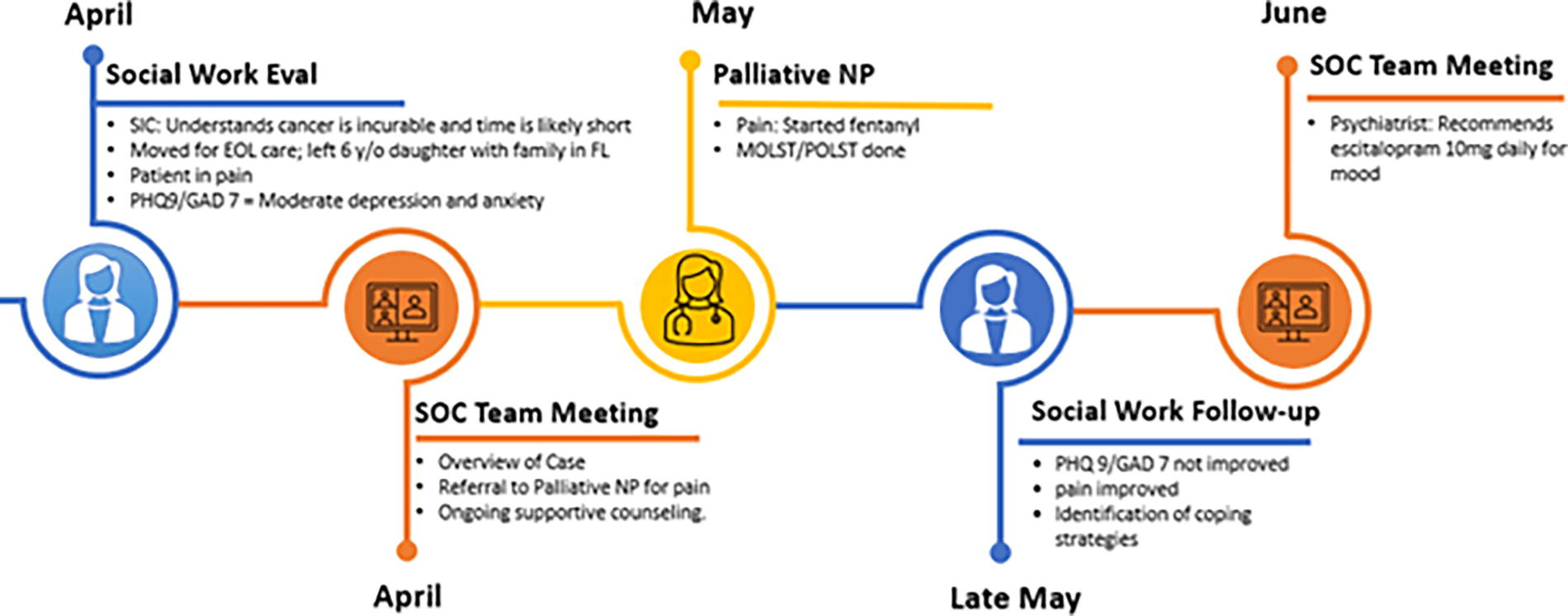
Patient flow through the Supportive Oncology Collaborative. GAD, Generalized Anxiety Disorder; PHQ, Patient Health Questionnaire.
A core principle of the SOC is measurement-based care and treatment to target: patients receiving care by the SOC continue to complete validated tools including the PHQ-9 and Generalized Anxiety Disorder-7 (GAD-7) at follow-up appointments to assess levels of depression and anxiety. 21 These assessments are sent to patients electronically via the electronic medical record (EMR) patient gateway, offered on a tablet when they come on-site for a clinic visit, or administered by the social worker during the visit. Patient responses to these two instruments are tracked, and if scores rise above a cut-off of 10 in either metric, it is used to trigger discussions of treatment plans in the team meeting. Pain and other symptom scores are monitored via nursing-reported pain scores and patient-reported data tools sent to patients via the patient portal. Patients with persistent pain scores above 6 out of 10 are triggered for discussion in team meetings. In addition, serious illness conversations are documented in the advanced care planning module of the EMR and shared with the SOC and oncology teams.
After each patient is presented at the weekly team meeting, the discussion is documented in the EMR in a structured note which identifies the reason for referral to the SOC, each issue discussed (pain, coping, advance care planning, etc.) as well as the team members who participate in the discussion.
Results
Over time, the SOC has served a large number of patients and seen substantial growth from 527 encounters in the first year to 2130 encounters in 2022 (Table 1) at the first site, the DFCI Merrimack Valley regional campus. This site has a diverse overall patient population that is 71.4% White, 4% Black, and 29.6% Hispanic/Latino, with 18.6% who speak Spanish as a primary language. The patients seen by palliative care providers via the SOC are similar to this overall patient population with more patients identifying as Hispanic/Latino and less identifying as White than patients seen by palliative care at the DFCI main campus in Boston (Table 2). In addition, this regional campus serves an under-resourced population via its contractual relationship with Lawrence General Hospital and Holy Family Hospital, where DFCI is the primary provider of oncology care. Both of these hospitals are high public payer sites that serve a racially and ethnically diverse patient population. 22
Clinical Volume Over Time
Demographics of Patients Seen by Palliative Care Clinicians in 2022
DFCI, Dana-Farber Cancer Institute; SOC, Supportive Oncology Collaborative.
As a population health initiative, the SOC uses patient-reported data to identify individuals who may benefit from intervention. Patients are identified as being at high, medium, or low risk for anxiety or depression based on their scores on the PHQ-9 or GAD-7. A score in either instrument of 10–14 is considered medium risk for depression or anxiety and a score of ≥15 is considered high risk. Of the patients who have completed an initial GAD-7, 30% (71/237) have scored either medium to high risk for anxiety, and of the patients who have completed and PHQ-9, 41.6% (97/233) scored either medium or high risk for depression. We track the number of patients with an elevated PHQ-9 or GAD-7 who are discussed in an interdisciplinary team meeting. Sixty percent of patients with a PHQ-9 of >10 and 75% of patients with a GAD of >10 are discussed at weekly team meetings.
Discussion
The National Coalition for Hospice and Palliative Care has placed a call to action to address the disparities that exist in accessing palliative care services in disparate community locations. 23 To meet this goal of increased access, we developed the SOC, which incorporates the key components of Collaborative Care and integrated palliative care and behavioral services in a novel way. Mental health needs are highly prevalent in people experiencing serious illnesses, either as pre-existing conditions or newly developed as a direct manifestation or complication of their serious illness. 24 Delivering psychosocial care along with palliative care is critical to address these needs effectively. By incorporating palliative care services and leveraging Collaborative Care models for mental health integration, we can capitalize on existing approaches that have demonstrated strong evidence of efficacy.
The goal of this model was to increase access to supportive care services for as many patients as possible. The weekly team meetings allowed specialty clinicians to review and provide recommendations for a large population of patients without being seen, while also identifying patients who could most benefit from additional individual consultation with a psychiatrist, psychologist, or palliative care physician.
One of the initial challenges we encountered was securing buy-in from social workers and oncologists when the program was first introduced. A contributing factor was the virtual nature of our team meetings, as we were coordinating expertise across various campuses. To address this, we decided to organize at least one in-person meeting annually at the regional campus, which significantly improved collaboration and engagement. In addition, involving the on-site social workers and the palliative care APP—who frequently collaborate closely with oncologists—in promoting the program was highly effective. Adopting this team-based approach for information sharing proved to be a valuable strategy in fostering mutual understanding and support for the program.
This descriptive report is limited in that it focuses on a clinical intervention in a single site in a relatively well-resourced part of the United States. Although there are years of research supporting the use of Collaborative Care to treat mental health concerns, expanding this to palliative care is novel. Behavioral health outcome metrics such as PHQ-9 and GAD-7 are well established, but it is not as clear what palliative care-focused outcomes would be optimal to target. Our current method involves using pain scores to monitor patients’ symptom burden, yet we continue to explore more effective ways to track outcomes related to physical symptoms. In the future, we hope to trial tools such as the Palliative Outcomes Scale, which focuses on the impact of symptoms on patient well-being. 25 A weakness of this model is the absence of comprehensive outcome metrics, patient satisfaction data, and cost analyses, which would encourage others to support its implementation. As we expand this model, our aim is to develop and track palliative care-focused outcome measures. In addition, the Collaborative Care model, as it stands, may not suffice for patients requiring more intensive services. For patients with serious mental illness, social workers, psychiatrists, and psychologists provide connections to community resources and serve as a liaison between those resources and the oncology and palliative care teams.
Leadership at the DFCI views this model as a successful implementation of clinical innovation and has invested in developing it. The SOC has recently expanded to three other DFCI regional campuses in the New England area. Each community location presents a unique context and set of challenges, and by learning from the individual sites, we can adapt and refine the SOC model to better suit the specific needs of each community. The SOC allows us to optimize resources, enhance coordination among health care professionals, and ensure that seriously ill patients receive the holistic care they require in the face of increasing demand.
Footnotes
Funding Information
No funding was received for this article.
Author Disclosure Statement
The authors have nothing to disclose.